Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Ivan Miguel Pires | + 5582 word(s) | 5582 | 2022-01-17 10:05:47 | | | |
| 2 | Vivi Li | Meta information modification | 5582 | 2022-01-27 10:27:33 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Pires, I.M. Monitoring of Six-Minute Walk Test. Encyclopedia. Available online: https://encyclopedia.pub/entry/18886 (accessed on 08 August 2026).
Pires IM. Monitoring of Six-Minute Walk Test. Encyclopedia. Available at: https://encyclopedia.pub/entry/18886. Accessed August 08, 2026.
Pires, Ivan Miguel. "Monitoring of Six-Minute Walk Test" Encyclopedia, https://encyclopedia.pub/entry/18886 (accessed August 08, 2026).
Pires, I.M. (2022, January 27). Monitoring of Six-Minute Walk Test. In Encyclopedia. https://encyclopedia.pub/entry/18886
Pires, Ivan Miguel. "Monitoring of Six-Minute Walk Test." Encyclopedia. Web. 27 January, 2022.
Copy Citation
In the pandemic time, the monitoring of the progression of some diseases is affected and rehabilitation is more complicated. Remote monitoring may help solve this problem using mobile devices that embed low-cost sensors, which can help measure different physical parameters. Many tests can be applied remotely, one of which is the six-minute walk test (6MWT). The 6MWT is a sub-maximal exercise test that assesses aerobic capacity and endurance, allowing early detection of emerging medical conditions with changes.
six-minute walk test
IoT
systematic review
mobile devices
telemedicine
1. Introduction
The six-minute walk test (6MWT) was officially introduced in 2002 by the American Thoracic Society, providing a detailed guideline for performing, monitoring, and analyzing the physical conditions of the patients [1]. It is a sub-maximal exercise test used to assess aerobic capacity and endurance. Changes in performance capacity are determined based on the distance covered in six minutes [1][2]. The 6MWT is helpful to evaluate performance and identify clinical conditions in preschool children (2–5 years), children (6–12 years), adults (18–64 years), and older adults (65+) with a wide range of diagnoses [3][4][5]. Even though the test was initially used to assess patients with cardiopulmonary issues, it was introduced over time in numerous other conditions [6][7]. It evaluates the individual’s functional capacity and provides valuable information regarding all the systems during physical activity, including pulmonary and cardiovascular systems, blood circulation, neuromuscular units, body metabolism, and peripheral circulation [8][9]. The 6MWT is used for different health conditions, including arthritis, fibromyalgia, geriatrics, multiple sclerosis, Parkinson’s disease, spinal cord injury, stroke, muscle disorders, spinal muscular atrophy, and Charcot–Marie–Tooth disease [10][11].
Motion and inertial sensors embedded in different devices have been used to monitor the 6MWT performance with diverse populations [3][4][5][12]. For example, Qureshi et al. [12] examined the changes in gait speed and gait cycle length variance over six minutes and the relationships between these variables with functional systems scores, modified fatigue impact scale, and multiple sclerosis walking scale. On the other hand, Daines et al. [3] used the 6MWT to develop a smartphone sensor-based fall-risk classification method in persons with lower-limb amputations. In the same line, Drover et al. [4] developed a wearable sensor-based faller classification method for older adults using accelerometer-based features from walking and turns during the 6MWT. Therefore, according to the existing evidence, the 6MWT can help track performance changes and detect emerging medical conditions early.
Despite the increasing work, to our best knowledge, no study synthesized the available evidence regarding the monitoring and detection of emerging medical conditions during the 6MWT using motion and inertial sensors. For example, a previous systematic review examined studies that used wearable inertial sensors for the gait assessment during the 6MWT [13]. However, the study only focused its review on wearable sensors for gait assessment, and none of the articles included pediatric populations [13]. Therefore, in this systematic review, we aim to synthesize the current state-of-the-art approaches for monitoring the 6MWT performance in a wide range of clinical populations. Furthermore, we focus on technological solutions to automate the 6MWT to be performed and measured at persons’ homes without medical personnel supervision. Additionally, we analyze the benefits of its continuous measurement and discuss the potential benefits regarding recovery and early detection of emerging medical conditions.
Different medical conditions need solutions for remote treatment and monitoring. As the sensors are available in commonly used mobile devices, and various physical tests can be performed independently by the population, the automatic analysis of the data can help detect multiple diseases. Automated detection is focused on using technology with artificial intelligence techniques and statistical analysis to identify different patterns related to walking, falls, and others. The system that will be developed will promote continuous measurement with the sensors, and the medical doctors can check the progression of its medical conditions remotely. The performance of these measurements is important for recovering some diseases, e.g., stroke, early detection of diseases, e.g., Parkinson’s disease, or continuous monitoring, e.g., older adults. Other conditions can be monitored, and further development will benefit the system.
2. Current researches
As presented in Figure 1, we identified 341 records from the selected sources. After analyzing each research article’s title and abstract, 231 papers were excluded by the unrelated 6MWT. Next, the literature reviews were excluded, resulting in the exclusion of 27 studies. Another reason for exclusion was the article type, excluding 18 conference abstracts. Then, the full text of the remaining 65 papers was analyzed, resulting in the exclusion of 16 studies that did not consider the sensors. Additionally, 13 studies were excluded because the purpose is not directly related to the 6MWT, 3 studies that did not mention the population or sample studied, and 5 studies that did not present the results. Finally, the remaining 31 research articles were examined and included in the qualitative and quantitative syntheses.
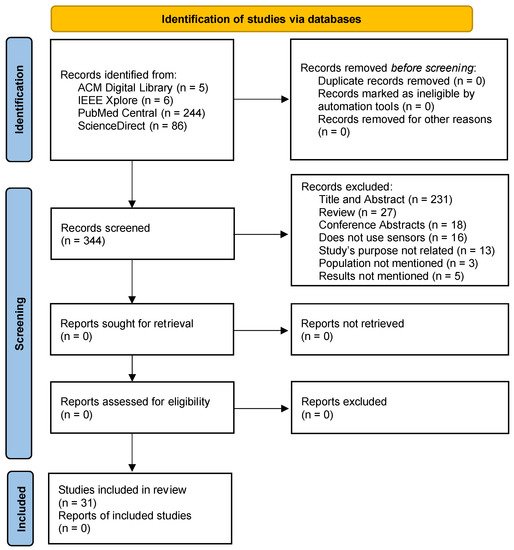
Figure 1. Flow diagram of the selection of the papers.
The selected studies were examined to extract the relevant data. The query performed in this study retrieved papers published between 2016 and 2021. As reported in Table 1, six studies (19%) were published in 2021, seven studies (23%) in 2020, six studies (19%) in 2019, four studies (13%) in 2018, four studies (13%) in 2017, and four studies (13%) in 2016. Regarding the location of the different studies, eight studies (26%) were performed in the USA, five studies (16%) in France, three studies (10%) in Italy, three studies (10%) in the UK, four studies (13%) in Canada, two studies (6%) in Switzerland, and the remaining studies (3%) in different countries, including Brazil, Belgium, Egypt, Australia, Israel, Korea, and Germany. Regarding the sensors used, 29 studies (94%) used motion and inertial sensors embedded in different devices, and the remaining 2 studies used Diffusion Tensor Imaging and Global Positioning System (GPS). Only four studies (13%) did not have medical collaboration. Regarding the type of methods implemented, most (97%) implemented statistical methods for the analysis, and only two studies (6%) used machine learning methods. Finally, 10 studies (32%) were related to multiple sclerosis, 6 studies (19%) to pulmonary diseases, 3 studies (10%) to heart diseases, 2 studies (6%) to brain injuries, 5 studies (16%) to bone diseases, 1 study (3%) to kidney diseases, and 3 studies (10%) did not define any disease.
The authors of [14] used wearable sensors embedded in a BeatWalk device, including ankle-worn and inertial sensors, and individualized musical stimulation for gait auto-rehabilitation with 6MWT performance. A total of 45 patients with Parkinson’s disease have gait disorders, but they walk without aids, aged 65 ± 9 years old, with moderate disease severity. The test was applied before and after the rehabilitation program, revealing that, on average, the distance walked increased by 17.63 m, the number of steps per minute increased by 3.07, the velocity increased by 0.04 m/s, the stride length increased by 0.02 m, and the asymmetry index decreased by 0.01%. The comparison was performed with Wilcoxon signed-rank test, and the whole data was also tested with Chi-squared tests or Fisher’s exact tests. The authors used musical stimulation during the experiments to improve the results on the 6MWT, where they verified that the results improved during and after the training program was applied. The 6MWT is an easy test that allows the authors to evaluate the gait auto-rehabilitation at home. The sensors were used to acquire the spatiotemporal gait parameters to control the variations during the drug cycle.
Hadouiri et al. [15] used the GAITRite walkway system (CIR Systems Inc., Franklin, NJ, USA) and the software PKMAS (ProtoKinetics, Havertown, PA, USA) for the measurement of different spatiotemporal variables during the 6MWT, including velocity, number of steps per minute, stride length, stride width, and double support time. In addition, the authors evaluated the performance of the inverted pendulum (IP) algorithm and an adaptation correcting for lateral step movement. The study consisted of the analysis of 45 patients with multiple sclerosis and 24 healthy individuals. The test was applied before and after the rehabilitation program in the two groups. Regarding the patients with multiple sclerosis, the values revealed that, on average, the distance walked increased by 19 m, the number of steps per minute increased by 3.4, the velocity increased by 0.05 m/s, the stride length increased by 0.01 m, the stride width maintained, and the double support time decreased by 0.89%. Regarding the healthy people, the values revealed that, on average, the distance walked increased by 34 m, the number of steps per minute increased by 5.58, the velocity increased by 0.11 m/s, the stride length increased by 0.03 m, the stride width maintained, and the double support time decreased by 1.2%. Additionally, the data analysis was performed with SAS version 9.4 (SAS Inc., Cary, NC, USA), measuring the mean and standard deviation of the acquired values. Finally, its homogeneity was evaluated with Kolmogorov–Smirnov and Levene’s tests. Thus, the authors accurately measured different spatiotemporal variables during 6MWT, which were used to adapt the rehabilitation care depending on the particular situation of other patients.
In [16], sensorized insoles (FlexInFit®, Sensormedica, Guidonia Montecelio, Rome, Italy) were used by two groups of participants with a total hip replacement, such as the experimental group composed of 19 patients and the control group formed by 21 patients to analyze the visual biofeedback effect for plantar pressure dynamic evaluation. The participants in the experimental group were, on average, 64.12 years old, with a height of 166.42 cm, and a weight of 72.74 kg. The participants in the control group were, on average, aged 61.30 years old, with a height of 172.00 cm, and a weight of 86.29 kg. The analyzed parameter related to the 6MWT was the distance. Thus, the experimental groups reported 194.3 m before the surgery and 308.4 m after the surgery. Additionally, the control group reported, on average, 187.5 m before the surgery and 310.2 m after the surgery. The data were analyzed with Shapiro–Wilk test to test the normality of the average, Pearson’s chi-squared test to test the associations between variables, Student’s t-test, and the analogous nonparametric Mann–Whitney U to test the different variables with the STATA statistical software version 14 (Stata Corporation, College Station, TX, USA, 2015). The authors used the 6MWT to determine the ability to walk after a total hip replacement. The sensors were used to easily measure the different distances during the rehabilitation phase and estimate the timeline to recovery.
Sagawa et al. [17] recruited 41 participants with multiple sclerosis and 16 healthy individuals as the reference group to determine the level of activity and establish associations between clinical parameters. The participants with multiple sclerosis were, on average, aged 51.3 years old, with a height of 1.67 m, and a weight of 75.4 kg, and they were mainly female persons. The healthy participants were, on average, aged 48.7 years old, with a height of 1.72 m, and a weight of 72.3 kg. The authors only measured the distance of the 6MWT, reporting an average of 267 m in participants with multiple sclerosis and 649 m in healthy participants. The Statistica version 10 (StatSoft, Tulsa, OK, USA) was used to evaluate the mean values with Student’s t-test, Chi-square test, one-way analysis of variance, and Tukey post-hoc tests. The 6MWT was used to measure the maximum distance walked for 6 min and the endurance of walking. The sensors were used to measure the different variables easily.
The authors of [18] used a mobile application that collects data from inertial sensors, a global positioning system (GPS) receiver, and a Bluetooth pulse oximeter for the assessment of the accuracy of the indoor 6MWT in clinical settings, the validity, and test–retest reliability of outdoor 6MWT in the community, the compliance, usability, and acceptance of the mobile application, and the feasibility of pulse oximetry during the 6MWT. For the performance of the tests, 30 individuals who participated with pulmonary hypertension were recruited, where 37% were male, and 63% were female, and their age, on average, was 50 years old. The participants used different devices, where three 3 patients used Android phones, twenty 20 used Apple iPhones, and nine 9 used both. In addition, the authors collected various features, e.g., distance. Finally, they were analyzed with statistics for the differences and Bland–Altman plots, revealing that the mobile application was sometimes inaccurate. Still, the results were correlated with the conventional application of the test. The 6MWT was used to assess the distance walked in patients with pulmonary arterial hypertension, where the sensors allow the quick computation of the walking distance in indoor and outdoor environments.
Tan et al. [19] recruited 11 patients aged between 20 and 60 years old with an average of 46 years old with spinal cord injuries. The participants used an optical motion capture system (Optotrak Certus; Northern Digital, Waterloo, ON, Canada) to track movements of infrared light-emitting rigid body sensors to examine the walking performance and intralimb motor coordination. For this purpose, the authors measured the distance. First, they performed different statistical tests with SPSS® 24 statistical software (Version 22, IBM Inc., Armonk, NY, USA), including Shapiro–Wilk’s test, Levene’s test, Greenhouse–Geisser corrections, linear mixed model, repeated-measures analysis of variance (rmANOVA), and Mann–Whitney U tests. The results revealed an increased distance in the performance of the 6MWT. Next, the authors used the 6MWT to quantify the walking performance. Finally, the sensors were used to track the motion of the fifth metatarsophalangeal, ankle, knee, and hip joints to correct the test’s evaluation.
In [20], the authors investigated the presence of local dynamic stability of gait in 80 patients with multiple sclerosis with minimal impairment and 20 participants in a control group during the performance of the 6MWT at their maximum speed. The different variables were measured with inertial sensors, calculating the short-term Lyapunov’s exponents. The acquired data were tested with the Wilcoxon rank-sum test, Fisher’s exact test, and mixed-design ANOVA, revealing that the gait speed was lower in patients with multiple sclerosis, high impact of fatigue, and poor balance. The authors used the 6MWT to assess the gait speed during its performance, where the used sensors allow the easy measurement of the gait speed, promoting remote monitoring.
Gulart et al. [21] used an accelerometer sensor to determine the cut-off point for the London Chest Activity of Daily Living scale to discriminate better functional status and the scores associated with clinical outcomes of a pulmonary rehabilitation program. They analyzed 61 patients with chronic obstructive pulmonary disease who were, on average, 65.5 years old, with a height of 1.67 m, and a weight of 72.7 kg with the distance measurement during the 6MWT. The acquired data were analyzed with SPSS Statistics 20.0 software to apply the Shapiro–Wilk test and calculate the Spearman correlation coefficients. The final comparisons were performed with Mann–Whitney U test, resulting in low correlations. In addition, the authors used the 6MWT to measure the distance walked during the test, where the use of sensors allows its calculation more accurately.
The authors of [22] use the steps measured by a Mi Band 2 device to evaluate its validity and reliability during the 6MWT performance. The study was composed of 14 healthy individuals, which, on average, were 23 years old. The study consisted of measuring the distance and speed during the test for further analysis. The analysis was performed with SPSS Statistical Software (Version 21), measuring the percent errors in the right and left wrist, comparing them with sample t-tests, and calculating the intra-class correlation coefficients. During the test, the patients walked, on average, 528 m with a speed of 5.3 km/h. The 6MWT is an easy test that allows the measurement of the number of steps during its performance. In addition, sensors were used to assess the validity and reliability of the Mi Band 2 wearable activity monitor.
Plotnik et al. [23] used six Opal motion sensor-based gait analysis systems (APDM, Portland, OR, USA) to assess gait asymmetry and bilateral coordination of gait during the 6MWT. They recruited 92 patients with multiple sclerosis and grouped them by disease severity. During the test, the authors acquired the distance covered and gait variably, performed the repeated measures ANOVA treating each 1 min interval, and calculated the correlation coefficients for each variable. They concluded that patients with lower severity presented better results. The 6MWT allows the assessment of persons with multiple sclerosis. The commodity and accurate measurement are important for the different measurements, where the sensors may be robust for these measurements for the other patients.
In [24], the authors used motion and heart rate sensors to compare the 6MWT in 107 patients with different stages of mitral and aortic valve disease. The patients were, on average, aged 66 years old, where 38 have aortic valve diseases, and 69 have mitral valve disease. Furthermore, since 65 participants were male, multiple correlations were performed between gender and disease types. Finally, on average, the participants walked 519 m during the 6MWT. Still, only 96.71% achieved the target of the distance. The 6MWT is commonly used to measure exercise tolerance and predict patient-centered outcomes, allowing the assessment of the exercise capacity and the comparisons between patients. Furthermore, it is important to evaluate the effects of therapeutic interventions and prognosis. In addition to the sensors facilitating the measurement of the distance walked, heart rate sensors detect different events to differentiate the tachyarrhythmia and activity.
The authors of [25] used a 6-channel head coil on a 1.5 T Philips Gyroscan Intera (Philips, Best, The Netherlands) with single-shot echo-planar imaging to measure the changes in vestibulospinal tract and parietoinsular vestibular cortex, and relation to the balance between old and young healthy adults. Regarding the 6MWT, the authors measured the distance in 11 old adults and 12 young adults. The old adults were, on average, aged 63.36 years old, with a height of 1.63 m, and a weight of 62.82 kg. The young adults were, on average, aged 28.42 years old, with a height of 1.71 m, and a weight of 66.42 kg. In addition, the participants were compared with the Mann–Whitney U test and independent t-test, showing a significant decrease in older adults. The 6MWT was used to analyze motor control, using the sensors to measure the distance to detect the changes in different aged participants.
Zeitlberger et al. [26] used a smartphone application to assess self-measured objective functional impairment with the 6MWT in three patients with lumbar degenerative disc disease with a GPS receiver. Unfortunately, the authors did not perform statistical tests with the distance measured. Still, on average, the reported values were between 381 m and 624 m. Thus, the 6MWT easily allows the assessment of functional impairment. Furthermore, measuring the distances with sensors allows easy measurements in the home environment to monitor the diseases constantly.
In [27], the authors used two inertial sensors (Physilog®4, Lausanne, Switzerland) placed on each foot with velcro strips and calculated 25 gait parameters in 20 participants with lower-limb amputation. They were, on average, aged 59 years old, with a height of 1.73 m, and a weight of 74.27 kg. The authors used the R software 3.3.3 to apply ANOVA and Wilcoxon signed-rank tests with the stance, flat foot ratio, minimal toe clearance, cadence, and speed, measured during the 6MWT. As a result, the average values of the stance increased by 0.25%, the flat foot ratio decreased by 3.41%, the minimal toe clearance decreased by 4.91 mm, the cadence decreased by 0.07 steps/min, and the speed was maintained. Thus, the 6MWT was instrumental in this research to monitor the evolution of different gait parameters after amputating a lower limb. Furthermore, it allowed the medical personnel to adapt the rehabilitation protocol depending on personal parameters and recovery speed.
The authors of [28] proposed using a proprietary device named SWING wearable multi-sensor system, which integrates an accelerometer, a gyroscope, a magnetometer, and up to three time-of-flight distance sensors. It was used to create a step counter based on the direct measurement of inter-leg distance. The number of participants in the study were five women and eight men with an average age of 42 years old, an average height of 1.74 m, and an average weight of 75 kg. The measurement of the distance reported an error of 2%. Thus, the 6MWT allowed reliable and relevant measurements of inter-leg distance and accurate step counting using sensors to monitor the progression of patients with multiple sclerosis.
Camp et al. [29] proposed using the SenseWear triaxial accelerometer to assess convergent, discriminant, known-group validity and floor/ceiling effects of the de Morton Mobility Index with the performance of the 6MWT. The 22 participants with acute exacerbation of chronic obstructive pulmonary disease had an average age of 60 years old, mainly had smoking habits and walk with aids. The sensors reported the distance and gait velocity during the test, and the data were analyzed with the SAS 9.4 (SAS Institute, Cary, NC, USA) to estimate the Spearmen’s correlations. The results reported a moderate positive correlation (i.e., correlation coefficient equals 0.61), which showed moderate to strong validity of the implemented method. In this research, the 6MWT was a feasible metric to perform mobility assessment in hospitalized patients with an acute exacerbation of chronic obstructive pulmonary disease. Similar to other research, the different measured parameters with sensors allowed the identification of distinct patterns in the disease progression and the recovery process.
In [30], the authors used three devices, including D-Jogger (Sennheiser, Hamburg, Germany), two iPod devices (Apple, California, USA), and three OPAL wearable sensors (Mobility Lab, APDM, Portland, OR, USA) to measure the spatiotemporal gait parameters and establish the comparison between patients with multiple sclerosis and healthy people. They recruited 31 patients with multiple sclerosis with an average age of 53.45 years old, an average height of 1.71 m, and an average weight of 69.10 kg. Additionally, 30 healthy individuals were recruited with an average age of 51.77 years old, an average height of 1.70 m, and an average weight of 71.15 kg. During the 6MWT performance, the distance was measured and further analyzed with Shapiro–Wilk test, ANOVA test, Student t-test, and Turkey’s test with the SAS JMP Pro 13.2.0 (SAS Institute Inc., Raleigh, NC, USA). The results reported an average distance of 377.56 m in patients with multiple sclerosis and 559.46 m in healthy people. The authors measured the parameters with this test and correlated them with perceived fatigue. Thus, it allowed the establishment of some patterns about how different parameters can help identify patients’ fatigue with multiple sclerosis. Moreover, the authors established a variability of these parameters about whether the test was performed with a metronome, in silence, or to music.
The authors of [31] recruited nine participants with relapsing-remitting multiple sclerosis with an average age of 45 years old and 26 healthy individuals with an average age of 45 years old. They performed the 6MWT equipped with seven wireless inertial sensors MIMUs (Xsens MTw, Xsens Technologies, Enschede, The Netherlands). Each one was placed on the pelvis and thigh, shank, and foot of both lower limbs to measure the changes in gait kinematics due to fatigue. The features extracted from the acquired data are the range of motion related to hip, knee, and ankle joint, tested with the Shapiro–Wilk test, and Student t-test. The reported results discovered significant effects of walking-related fatigue on gait kinematics with reducing the range of motion during the performance of 6MWT.
Tousignant et al. [32] used biomedical sensors wirelessly transmitting a real-time ECG signal (180° eMotion Faros device), oxygen saturation, and heart rate (Nonin WristOx2 3150 device) to evaluate its feasibility in telerehabilitation based on 6MWT. Four male participants with heart failure disease were recruited with an average age of 66.25 years old. However, only statistical measurements have been performed, verifying that the mean variation of walking distance was 44 m. Thus, even though this paper illustrates that sensors are beneficial for obtaining reliable measurements, it did not systematically and thoroughly analyze the direct benefits of the 6MWT.
The authors of [33] researched the relationship between lower limb muscle activation patterns and chronic gait deficits in individuals who previously experienced a traumatic brain injury with accelerometer and electromyography sensors. The sensors measured different parameters, including the distance and walking speed during the 6MWT performance. The study included 44 individuals after traumatic brain injury, which had, on average, 53.4 years old, and 28 were females. Additionally, 20 healthy control subjects, which had, on average, 25.3 years old, and 10 were females, were included. The acquired data was tested with SPSS Statistical Software (v. 24, IBM Corp., Armonk, NY, USA), implementing the Mann–Whitney U tests, Shapiro–Wilk’s test, and Spearman’s rank-order correlation. The results reported that the average distance in the experimental group was 386 m, whereas the standard distance in healthy subjects was between 400 m and 700 m. Additionally, the results were not correlated to walking speeds. Performing such an analysis was only possible because of using systematic sensory measurements.
In [34], the authors used inertial sensors (RehaGait) capturing three-dimensional foot accelerations to evaluate the acceleration gait and the exercise-induced changes in patients with symptomatic lumbar spinal stenosis. The 6MWT was performed by 24 healthy individuals, where 9 were males and 15 were female, and they were, on average, 59.9 years old, with an average height of 1.69 m, and an average weight of 68.5 kg. Additionally, the test included 19 patients with symptomatic lumbar spinal stenosis, where 11 were males and 8 were female, and they were, on average, 73.8 years old, with an average height of 1.68 m, and an average weight of 75.8 kg. The data were analyzed with SPSS Version 21 (IBM Corporation, Armonk, NY, USA), measuring the results of the Shapiro–Wilk test, the Mann–Whitney U test, the ANOVA test, and the Bonferroni post-hoc tests. The average distance measured with healthy individuals was 410.7 m, and the value of the patients with symptomatic lumbar spinal stenosis was 361.4 m. Thus, the 6MWT and the inertial sensor-based measurements allowed the authors to perform statistically significant analysis and comparison of healthy and patients with symptomatic lumbar spinal stenosis.
D’Alessando et al. [35] assessed the prevalence and correlation of sarcopenia among elderly male patients with chronic kidney disease based on SenseWear Armband (SWA, BodyMedia, Inc., Pittsburgh, PA, USA) for the measurement of the distance walked during 6MWT. The participants included 80 patients over the age of 60 with an average weight of 80.6 kg, 40 patients aged 75 or over with an average weight of 77.3 kg, and 40 patients aged between 60 and 74 with an average weight of 84 kg. The distance walked during 6MWT was analyzed with SPSS v.25 (SPSS Inc., Chicago, IL, USA), performing descriptive analysis. The reported average values were 282 m for the patients aged 75 or over and 336 m for those between 60 and 74 years old. The authors identified that the average daily physical activity was lower in the older seniors than younger ones based on the performed measurements. Furthermore, among older seniors, sarcopenic and non-sarcopenic ones differed in age and performance on the 6MWT.
The authors of [36] also used the GAITRite walkway system (CIR Systems Inc., Franklin, NJ, USA) for the measurement of the effect of vascularized fibula free flap (VFFF) harvesting on spatiotemporal gait variables, including distance, cadence, velocity, stride length, stance, and step length, during the 6MWT. The participants in the study were 11 patients with vascularized fibula free flap and 11 healthy individuals. The patients with vascularized fibula free flap were, on average, 59 years old, with an average height of 1.70 m, and an average weight of 66 kg. The healthy individuals were, on average, 53 years old with an average height of 1.72 m and an average weight of 72 kg. The analysis of the acquired data was performed with Statistica version 10 software (Stat-Soft, Inc., Tulsa, OK, USA), measuring the results with descriptive statistics, implementing Mann–Whitney U test, ANOVA test, and Wilcoxon signed-rank test. The average results revealed that the distance was 436 m in patients with vascularized fibula free flap and 632 m in healthy individuals. Next, the velocity along the test decreased 0.1 m/s in patients with vascularized fibula free flap and 0.01 m/s in healthy individuals. Sequentially, the stride length along the test decreased 0.02 m in patients with vascularized fibula free flap and 0.04 m in healthy individuals. Next, the cadence along the test decreased 2.2 steps per minute in patients with vascularized fibula free flap and 4.0 steps per minute in healthy individuals. Sequentially, the stance along the test increased 0.02% in patients with vascularized fibula free flap and 0.35% in healthy individuals. Finally, the step length along the test was maintained in patients with vascularized fibula free flap and decreased 0.01 m in healthy individuals. With the help of the 6MWT, the authors were able to identify a significantly lower velocity between the beginning and end periods only for the VFFF group, suggesting an alteration in physical management. In conclusion, these results indicate that VFFF harvesting could alter gait and joint integrity.
In [37], the authors used spirometry to assess the metabolic disturbance and its reflection on the muscular state in interstitial pulmonary fibrosis patients. Three groups of 22 patients were analyzed, including normal people with an average of 48.9 years old, interstitial pulmonary fibrosis patients with an average age of 55.8 years old, and another group with interstitial pulmonary fibrosis patients with an average age of 51.1 years old. The data were analyzed with SPSS Statistical Software v22 (SPSS Inc., Chicago, IL, USA) for the performance of descriptive statistics, Chi-square or Fisher exact tested proportion independence, ANOVA test, paired t-test, and Mann–Whitney tests. The tests revealed that the average distance during the performance of 6MWT was higher (+148.4 m) in patients without oxygen therapy.
Kennedy et al. [5] also used the GAITRite walkway system (CIR Systems Inc., Franklin, NJ, USA) to research changes in spatiotemporal gait parameters and functional ambulation with several assessments, including the 6MWT. In the study, 27 children with Charcot–Marie–Tooth disease performed the assessments, in which 18 were males, the average age was 12.2 years old, the average height was 1.52 m, and the average weight was 47.1 kg. In addition, the authors performed initial assessments and another set of evaluations after 12 months, where the distance during the test was on the parameters measured. The acquired data were analyzed with the Stata (version 14) software package, descriptive statistics, and Shapiro–Wilk test results. The analysis revealed that the results slightly decreased, i.e., the average distance decreased 1 m in 12 months. The different parameters measured by the sensors during the 6MWT were instrumental in this analysis for an objective comparison between the other groups.
The authors of [38] used BioStampRC devices (MC10, Inc., Lexington, MA, USA), MTx inertial sensors (Xsens Technologies B.V., Overissel, The Netherlands), and tri-axial activity tracker GT3X (Actigraph, Pensacola, FL, USA). The sensors were used to measure gait characteristics, including the distance walked during 6MWT, the number of steps, the stride time, the swing time, and the step time of 45 patients with multiple sclerosis and 15 healthy subjects under controlled conditions. The measurements were analyzed with MATLAB code (The MathWorks, Natick, MA, USA) and IBM SPSS Statistics for Windows (version 22; IBM SPSS Inc., Armonk, NY, USA). The software was used to perform descriptive statistics, Bland–Altman plots, ANOVA analysis, and Mann–Whitney U test for post-hoc analysis. The average distance and the average step number decreased with the severity of the disease. On the other hand, the average stride time, the average swing time, and the average step time increased with the severity of the disease.
In [39], low-cost motion sensors were used to assess the functional capacity in older adults with chronic obstructive pulmonary disease. For this purpose, the 6MWT was applied, and the distance was measured. The sample in the study consisted of 49 individuals, where 30 were males and 19 were female. Firstly, the male subjects were, on average, aged 72 years old, with an average weight of 86.5 kg, and an average height of 1.75 m. Secondly, the female subjects were, on average, aged 71 years old, with an average weight of 71.4 kg, and an average height of 1.59 m. Finally, the whole sample was aged 72 years old, with an average weight of 80.7 kg, and an average height of 1.69 m. The data analysis was performed with JMP version 11 (SAS Institute, Inc., Cary, NC, USA), measuring the different correlations. They also used the multivariable linear regression model, Shapiro–Wilk test, and paired t-test to obtain the results. The results showed a higher average distance in male subjects than female subjects based on the measurements during the 6MWT.
Cheng et al. [40] used the accelerometer and spirometry sensors to create classification models to measure the pulmonary function in 24 patients. The features were extracted with a feature selection approach, where one of them was the cadence. The patients were, on average, aged 76 years old, with an average height of 1.67 m, an average weight of 83 kg, and only nine were female. The data were analyzed with support vector machine (SVM) models, reporting that the patients may use their mobile phones to support automatic computation of pulmonary function. In addition, the accelerometer and spirometer sensors provided reliable time-series data that contained patterns related to the different conditions of the patients.
The authors of [41] used only the accelerometer sensor to implement several models to monitor cardiopulmonary conditions, and they created a new model named DPClass. The study included 55 pulmonary patients and 11 healthy subjects to measure the cadence and velocity with the sensors’ data. Thus, the authors implemented linear and radial basis function (RBF)—SVM models, decision trees, and the DPClass model with pattern classification techniques. The overall results reported that the best accuracy was achieved with the RBF SVM model. The second one was the DPClass model, proving the reliability of the implemented model. Ultimately, the whole approach was reliable on the accelerometer measurements to facilitate the corresponding analysis of the cardiopulmonary conditions.
In [42], the GAITRite walkway system (CIR Systems Inc., Franklin, NJ, USA) was also used to establish the relationship between the walk ratio and other measurements in 229 patients with multiple sclerosis. On average, the patients were aged 43.4 years old, with a height of 1.68 m, a weight of 69.4 kg, and the gender distribution consisted of 143 females and 86 males. The authors acquired the distance during the 6MWT. It was also compared with descriptive statistics, correlation coefficients, and ANOVA tests with SPSS software (Version 23.0 for Windows, SPSS Inc., Chicago, IL, USA). The results reported an average distance of 423.4 m with a low correlation with walk ratio. Thus, the measure of gait control through the walk ratio was facilitated by the 6MWT measurements of patients with multiple sclerosis.
Qureshi et al. [10], a blockchain-based service network (BSN) platform called TEMPO3.1 analyzes changes in gait speed and gait cycle length variance during 6MWT, determining the relationships between these variables and functional systems scores, modified fatigue impact scale, and multiple sclerosis walking scale. The study recruited 28 patients with multiple sclerosis aged between 18 and 65 years old. The results reported that fatigue was high in the analyzed patients, and it reported high variance in the gait cycle length in the last minute of the test.
References
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117.
- Bradley, P.S.; Mohr, M.; Bendiksen, M.; Randers, M.B.; Flindt, M.; Barnes, C.; Hood, P.; Gomez, A.; Andersen, J.L.; Di Mascio, M.; et al. Sub-maximal and maximal Yo–Yo intermittent endurance test level 2: Heart rate response, reproducibility and application to elite soccer. Eur. J. Appl. Physiol. 2011, 111, 969–978.
- Daines, K.J.F.; Baddour, N.; Burger, H.; Bavec, A.; Lemaire, E.D. Fall risk classification for people with lower extremity amputations using random forests and smartphone sensor features from a 6-minute walk test. PLoS ONE 2021, 16, e0247574.
- Drover, D.; Howcroft, J.; Kofman, J.; Lemaire, E. Faller Classification in Older Adults Using Wearable Sensors Based on Turn and Straight-Walking Accelerometer-Based Features. Sensors 2017, 17, 1321.
- Kennedy, R.; Carroll, K.; Paterson, K.L.; Ryan, M.M.; McGinley, J.L. Deterioration in gait and functional ambulation in children and adolescents with Charcot–Marie–Tooth disease over 12 months. Neuromuscul. Disord. 2017, 27, 658–666.
- Thygesen, K.; Mair, J.; Giannitsis, E.; Mueller, C.; Lindahl, B.; Blankenberg, S.; Huber, K.; Plebani, M.; Biasucci, L.M.; Tubaro, M.; et al. How to use high-sensitivity cardiac troponins in acute cardiac care. Eur. Heart J. 2012, 33, 2252–2257.
- Kimberlin, C.L.; Winterstein, A.G. Validity and reliability of measurement instruments used in research. Am. J. Health Syst. Pharm. 2008, 65, 2276–2284.
- Cousins, S.O.B. Exercise, Aging and Health: Overcoming Barriers to an Active Old Age; Taylor & Francis: London, UK, 2014; ISBN 978-1-317-76346-8.
- Granger, C.L.; McDonald, C.F.; Parry, S.M.; Oliveira, C.C.; Denehy, L. Functional capacity, physical activity and muscle strength assessment of individuals with non-small cell lung cancer: A systematic review of instruments and their measurement properties. BMC Cancer 2013, 13, 135.
- Kennedy-Malone, L. Central and Peripheral Nervous System Disorders. Adv. Pract. Nurs. Care Older Adults 2018, 328.
- Volkers, K.M.; Scherder, E.J. The effect of regular walks on various health aspects in older people with dementia: Protocol of a randomized-controlled trial. BMC Geriatr. 2011, 11, 38.
- Qureshi, A.; Brandt-Pearce, M.; Goldman, M.D. Relationship between gait variables and domains of neurologic dysfunction in multiple sclerosis using six-minute walk test. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 4959–4962.
- Storm, F.A.; Cesareo, A.; Reni, G.; Biffi, E. Wearable Inertial Sensors to Assess Gait during the 6-Minute Walk Test: A Systematic Review. Sensors 2020, 20, 2660.
- PRISMA-P Group; Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1.
- Zdravevski, E.; Lameski, P.; Trajkovik, V.; Chorbev, I.; Goleva, R.; Pombo, N.; Garcia, N.M. Automation in Systematic, Scoping and Rapid Reviews by an NLP Toolkit: A Case Study in Enhanced Living Environments. In Enhanced Living Environments; Ganchev, I., Garcia, N.M., Dobre, C., Mavromoustakis, C.X., Goleva, R., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2019; Volume 11369, pp. 1–18. ISBN 978-3-030-10751-2.
- Cochen de Cock, V.; Dotov, D.; Damm, L.; Lacombe, S.; Ihalainen, P.; Picot, M.C.; Galtier, F.; Lebrun, C.; Giordano, A.; Driss, V.; et al. BeatWalk: Personalized Music-Based Gait Rehabilitation in Parkinson’s Disease. Front. Psychol. 2021, 12, 655121.
- Hadouiri, N.; Monnet, E.; Gouelle, A.; Decavel, P.; Sagawa, Y. Evaluation of Prolonged Walking in Persons with Multiple Sclerosis: Reliability of the Spatio-Temporal Walking Variables during the 6-Minute Walk Test. Sensors 2021, 21, 3075.
- Marin, L.; Vandoni, M.; Zaza, G.; Febbi, M.; Pedrotti, L.; Chiodaroli, M.; Lovecchio, N.; Manzoni, F. The Effects of Insole-Based Visual Feedback on Weight-Bearing in Patients Undergoing Total Hip Replacement. Int. J. Environ. Res. Public Health 2021, 18, 3346.
- Sagawa, Y.; Watelain, E.; Moulin, T.; Decavel, P. Physical Activity during Weekdays and Weekends in Persons with Multiple Sclerosis. Sensors 2021, 21, 3617.
- Salvi, D.; Poffley, E.; Tarassenko, L.; Orchard, E. App-Based Versus Standard Six-Minute Walk Test in Pulmonary Hypertension: Mixed Methods Study. JMIR mHealth uHealth 2021, 9, e22748.
- Tan, A.Q.; Sohn, W.J.; Naidu, A.; Trumbower, R.D. Daily acute intermittent hypoxia combined with walking practice enhances walking performance but not intralimb motor coordination in persons with chronic incomplete spinal cord injury. Exp. Neurol. 2021, 340, 113669.
- Caronni, A.; Gervasoni, E.; Ferrarin, M.; Anastasi, D.; Brichetto, G.; Confalonieri, P.; Di Giovanni, R.; Prosperini, L.; Tacchino, A.; Solaro, C.; et al. Local Dynamic Stability of Gait in People with Early Multiple Sclerosis and No-to-Mild Neurological Impairment. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 1389–1396.
- Gulart, A.A.; Munari, A.B.; Klein, S.R.; Venâncio, R.S.; Alexandre, H.F.; Mayer, A.F. The London Chest Activity of Daily Living scale cut-off point to discriminate functional status in patients with chronic obstructive pulmonary disease. Braz. J. Phys. Ther. 2020, 24, 264–272.
- Paradiso, C.; Colino, F.; Liu, S. The Validity and Reliability of the Mi Band Wearable Device for Measuring Steps and Heart Rate. Int. J. Exerc. Sci. 2020, 13, 689–701.
- Plotnik, M.; Wagner, J.M.; Adusumilli, G.; Gottlieb, A.; Naismith, R.T. Gait asymmetry, and bilateral coordination of gait during a six-minute walk test in persons with multiple sclerosis. Sci. Rep. 2020, 10, 12382.
- Schubert, C.; Archer, G.; Zelis, J.M.; Nordmeyer, S.; Runte, K.; Hennemuth, A.; Berger, F.; Falk, V.; Tonino, P.A.L.; Hose, R.; et al. Wearable devices can predict the outcome of standardized 6-minute walk tests in heart disease. NPJ Digit. Med. 2020, 3, 92.
- Yeo, S.S.; Kwon, J.W.; Cho, I.H. Associations between Age-Related Changes in the Core Vestibular Projection Pathway and Balance Ability: A Diffusion Tensor Imaging Study. Behav. Neurol. 2020, 2020, 2825108.
- Zeitlberger, A.M.; Sosnova, M.; Ziga, M.; Steinsiepe, V.; Gautschi, O.P.; Stienen, M.N.; Maldaner, N. Smartphone-Based Self-Assessment of Objective Functional Impairment (6-Minute Walking Test) in Patients Undergoing Epidural Steroid Injection. Neurospine 2020, 17, 136–142.
- Beausoleil, S.; Miramand, L.; Turcot, K. Evolution of gait parameters in individuals with a lower-limb amputation during a six-minute walk test. Gait Posture 2019, 72, 40–45.
- Bertuletti, S.; Salis, F.; Cereatti, A.; Angelini, L.; Buckley, E.; Nair, K.P.S.; Mazza, C.; Croce, U.D. Inter-leg Distance Measurement as a Tool for Accurate Step Counting in Patients with Multiple Sclerosis. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 6413–6417.
- Camp, P.G.; Sima, C.A.; Kirkham, A.; Inskip, J.A.; Parappilly, B. The de Morton mobility index is a feasible and valid mobility assessment tool in hospitalized patients with an acute exacerbation of chronic obstructive pulmonary disease. Chron. Respir. Dis. 2019, 16, 147997311987297.
- Moumdjian, L.; Moens, B.; Maes, P.-J.; van Geel, F.; Ilsbroukx, S.; Borgers, S.; Leman, M.; Feys, P. Continuous 12 min walking to music, metronomes and in silence: Auditory-motor coupling and its effects on perceived fatigue, motivation and gait in persons with multiple sclerosis. Mult. Scler. Relat. Disord. 2019, 35, 92–99.
- Taborri, J.; Studer, V.; Grossi, P.; Brambilla, L.; Ferro, M.T.; Mantegazza, R.; Rossi, S. Measuring changes in gait kinematics due to walking-related fatigue in patients with Multiple Sclerosis. In Proceedings of the 2019 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Istanbul, Turkey, 26–28 June 2019; pp. 1–6.
- Tousignant, M.; Mampuya, W.M.; Bissonnette, J.; Guillemette, E.; Lauriault, F.; Lavoie, J.; St-Laurent, M.-E.; Pagé, C. Telerehabilitation with live-feed biomedical sensor signals for patients with heart failure: A pilot study. Cardiovasc. Diagn. Ther. 2019, 9, 319–327.
- Acuña, S.A.; Tyler, M.E.; Danilov, Y.P.; Thelen, D.G. Abnormal muscle activation patterns are associated with chronic gait deficits following traumatic brain injury. Gait Posture 2018, 62, 510–517.
- Byrnes, S.K.; Nüesch, C.; Loske, S.; Leuenberger, A.; Schären, S.; Netzer, C.; Mündermann, A. Inertial Sensor-Based Gait and Attractor Analysis as Clinical Measurement Tool: Functionality and Sensitivity in Healthy Subjects and Patients with Symptomatic Lumbar Spinal Stenosis. Front. Physiol. 2018, 9, 1095.
- D’Alessandro, C.; Piccoli, G.; Barsotti, M.; Tassi, S.; Giannese, D.; Morganti, R.; Cupisti, A. Prevalence and Correlates of Sarcopenia among Elderly CKD Outpatients on Tertiary Care. Nutrients 2018, 10, 1951.
- Hadouiri, N.; Feuvrier, D.; Pauchot, J.; Decavel, P.; Sagawa, Y. Donor site morbidity after vascularized fibula free flap: Gait analysis during prolonged walk conditions. Int. J. Oral Maxillofac. Surg. 2018, 47, 309–315.
- El Hosainy, A.; Kaddah, S.; Saied, M.; Ibrahim, A.; Darwish, R. Preliminary study of the anabolic/catabolic balance in patients with interstitial pulmonary fibrosis. Egypt. J. Chest Dis. Tuberc. 2017, 66, 497–503.
- Moon, Y.; McGinnis, R.S.; Seagers, K.; Motl, R.W.; Sheth, N.; Wright, J.A.; Ghaffari, R.; Sosnoff, J.J. Monitoring gait in multiple sclerosis with novel wearable motion sensors. PLoS ONE 2017, 12, e0171346.
- Toosizadeh, N.; Berry, C.; Bime, C.; Najafi, B.; Kraft, M.; Mohler, J. Assessing upper-extremity motion: An innovative method to quantify functional capacity in patients with chronic obstructive pulmonary disease. PLoS ONE 2017, 12, e0172766.
- Cheng, Q.; Juen, J.; Bellam, S.; Fulara, N.; Close, D.; Silverstein, J.C.; Schatz, B. Classification Models for Pulmonary Function using Motion Analysis from Phone Sensors. AMIA Annu. Symp. Proc. AMIA Symp. 2016, 2016, 401–410.
More
Information
Contributor
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
1.4K
Revisions:
2 times
(View History)
Update Date:
02 Feb 2022
Table of Contents



Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No