 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Ngan Huang | + 2656 word(s) | 2656 | 2021-12-22 11:38:39 |
Video Upload Options
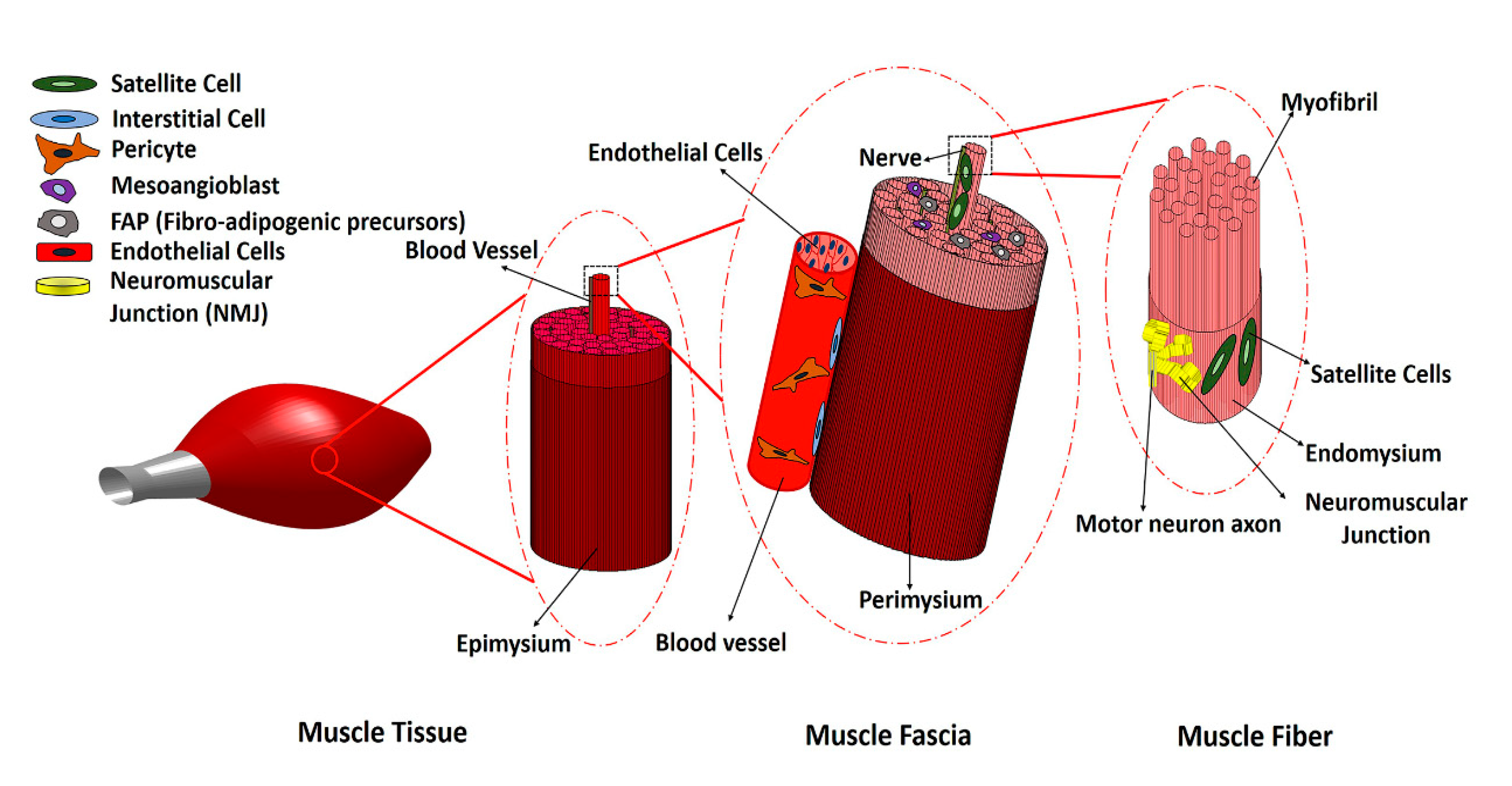
Volumetric muscle loss (VML) is the traumatic, surgical or degenerative loss of a substantial portion of bulk skeletal muscle in a manner that overwhelms the endogenous repair capacity of the muscle and results in impaired scar tissue formation. Cell-based therapies have emerged as a promising approach to promote skeletal muscle regeneration following injury and/or disease. Stem cell populations, such as muscle stem cells, mesenchymal stem cells and induced pluripotent stem cells (iPSCs), have shown a promising capacity for muscle differentiation. Support cells, such as endothelial cells, nerve cells or immune cells, play a pivotal role in providing paracrine signaling cues for myogenesis, along with modulating the processes of inflammation, angiogenesis and innervation.
1. Introduction
2. Main Myogenic Cell Sources
|
Cell Types |
Markers |
Location |
Advantages |
Disadvantages |
Reference |
|---|---|---|---|---|---|
|
MuSCs |
Pax7+, CD56+, MyoD+ |
Under basal lamina of muscle fibers. |
Critical to native skeletal muscle regeneration. High myogenic potential. |
Isolation is invasive and low yield. Loss of self-renewal potential during in vitro expansion. Loss of differentiation potential after in vivo transplantation. |
|
|
Mesenchymal stem cells (MSCs) |
CD90+, CD44+, CD29+, CD105+, CD13+, CD73+, CD166+, CD45−, CD34−, CD14− |
Adipose tissue, bone marrow (BM), umbilical cord (UC). |
Abundance of adipose tissue. Ease of isolation from adipose tissue. Low expression of MHC-I and MHC-II Immunomodulatory effect. |
Invasive isolation for BM-MSCs. Poor myogenic differentiation capacity. |
|
|
Myo-endothelial cells |
CD34+, CD144+, CD56+, CD31+, CD45− |
Periphery of myofibers close to blood vessels. |
Have both angiogenic and myogenic capacity. |
Laborious isolation and purification process. Limited literature on their role in skeletal muscle regeneration. |
[20] |
|
Mesoangioblasts |
CD34+, Sca-1+, CD31+, c-Kit+, CD45− |
Walls of microvessels. |
High proliferative capacity in vitro. Multipotent cells with potential to differentiate into skeletal muscle |
Invasive isolation procedure. Lack of studies for VML treatment. |
[21] |
|
Pericytes |
CD146+, NG2+, ALP+, PDGFR-β+ |
Periphery of capillaries and microvessels. |
Pericyte myogenesis naturally occurs during development and regeneration of muscle. High muscle differentiation potential. Lack of MHCII expression. |
Limited literature on their potential in skeletal muscle regeneration and VML. |
|
|
CD133+ progenitor cells |
CD133+, CD34+/−, CD90+/−, CD146+ |
Periphery of myofibers close to blood vessels. |
Availability and ease of purification from peripheral blood Myogenic and angiogenic capacity. |
Reduction of myogenic potential following in vitro culture. |
|
|
Induced pluripotent stem cells (iPSCs) |
Oct4+, Sox2+, KLF4+, and c-Myc+ |
All tissues, mainly skin. |
Unlimited self-renewal in vitro. Patient-derived autologous cells. Myogenic differentiation capacity. |
Risk of tumorigenicity and genetic instability. |
|
|
Embryonic stem cells (ESCs) |
Oct4+, Sox2+, KLF4+, and c-Myc+ |
Inner cell mass of blastocyst. |
Unlimited self-renewal in vitro. Myogenic differentiation capacity |
Ethical concerns Inefficient isolation process. Risk of tumorigenicity. Risk associated with immune response. |
[6] |
|
Muscle side population cells (SPs) |
CD45−, c-Kit−, Sca1+, ABCG2+, Pax7−, Myf5−, Desmin− |
Interstitial space of skeletal muscle. |
Myogenic differentiation capacity in vivo. |
Low availability Lack of specific phenotypic markers. Poor myogenic differentiation in vitro. Limited literature on their potential for skeletal muscle regeneration and VML. |
Abbreviations: Stem cells antigen -1 (Sca-1), Alkaline phosphatase (ALP), Platelet-derived growth factor receptor beta (PDGFR-β), Neural/glial antigen 2 (NG 2), ATP binding cassette subfamily G member 2 (ABCG-2), Octamer-binding transcription factor 4 (Oct-4), SRY (sex determining region Y)-box 2 (Sox-2), Kruppel-like factor 4 (KLF4), Myogenic factor 5 (Myf5).
3. Non-Myogenic Cells
4. Preclinical VML Treatment Studies
4.1. Animal Models of VML
4.2. Cell-Seeded Scaffolds for Preclinical Treatment of VML
4.3. MuSC-Based Therapies for Preclinical Treatment of VML
4.4. MSC-Based Therapies for Preclinical Treatment of VML
References
- Corona, B.T.; Rivera, J.C.; Owens, J.G.; Wenke, J.C.; Rathbone, C.R. Volumetric muscle loss leads to permanent disability following extremity trauma. J. Rehabil. Res. Dev. 2015, 52, 785–792.
- Garg, K.; Ward, C.L.; Hurtgen, B.J.; Wilken, J.M.; Stinner, D.J.; Wenke, J.C.; Owens, J.G.; Corona, B.T. Volumetric muscle loss: Persistent functional deficits beyond frank loss of tissue. J. Orthop. Res. 2014, 33, 40–46.
- Corona, B.T.; Wenke, J.C.; Ward, C.L. Pathophysiology of volumetric muscle loss injury. Cells Tissues Organs 2016, 202, 180–188.
- Lin, C.-H.; Lin, Y.-T.; Yeh, J.-T.; Chen, C.-T. Free Functioning muscle transfer for lower extremity posttraumatic composite structure and functional defect. Plast. Reconstr. Surg. 2007, 119, 2118–2126.
- Ding, S.; Wang, F.; Liu, Y.; Li, S.; Zhou, G.; Hu, P. Characterization and isolation of highly purified porcine satellite cells. Cell Death Discov. 2017, 3, 17003.
- Pantelic, M.N.; Larkin, L.M.; Pantellic, M.N. Stem cells for skeletal muscle tissue engineering. Tissue Eng. Part B Rev. 2018, 24, 373–391.
- Garcia, J.M.S.; Panitch, A.; Calve, S. Functionalization of hyaluronic acid hydrogels with ECM-derived peptides to control myoblast behavior. Acta Biomater. 2019, 84, 169–179.
- Patel, K.H.; Dunn, A.J.; Talovic, M.; Haas, G.J.; Marcinczyk, M.; Elmashhady, H.; Kalaf, E.A.G.; Sell, S.A.; Garg, K.; Growney, E. Aligned nanofibers of decellularized muscle ECM support myogenic activity in primary satellite cells in vitro. Biomed. Mater. 2019, 14, 035010.
- Prueller, J.; Mannhardt, I.; Eschenhagen, T.; Zammit, P.S.; Figeac, N. Satellite cells delivered in their niche efficiently generate functional myotubes in three-dimensional cell culture. PLoS ONE 2018, 13, e0202574.
- Gilbert, P.M.; Havenstrite, K.L.; Magnusson, K.E.G.; Sacco, A.; Leonardi, N.A.; Kraft, P.; Nguyen, N.K.; Thrun, S.; Lutolf, M.P.; Blau, H.M. Substrate elasticity regulates skeletal muscle stem sell self-renewal in culture. Science 2010, 329, 1078–1081.
- Mori, R.; Kamei, N.; Okawa, S.; Nakabayashi, A.; Yokota, K.; Higashi, Y.; Ochi, M. Promotion of skeletal muscle repair in a rat skeletal muscle injury model by local injection of human adipose tissue-derived regenerative cells. J. Tissue Eng. Regen. Med. 2012, 9, 1150–1160.
- Berebichez-Fridman, R.; Montero-Olvera, P.R. Sources and Clinical Applications of Mesenchymal Stem Cells. Sultan Qaboos Univ. Med. J. 2018, 18, 264–277.
- Jacobs, S.A.; Roobrouck, V.D.; Verfaillie, C.M.; Van Gool, S.W. Immunological characteristics of human mesenchymal stem cells and multipotent adult progenitor cells. Immunol. Cell Biol. 2013, 91, 32–39.
- Kodaka, Y.; Rabu, G.; Asakura, A. Skeletal Muscle Cell Induction from Pluripotent Stem Cells. Stem Cells Int. 2017, 2017, 1–16.
- del Carmen Ortuño-Costela, M.; García-López, M.; Cerrada, V.; Gallardo, M.E. iPSC s: A powerful tool for skeletal muscle tissue engineering. J. Cell. Mol. Med. 2019, 23, 3784–3794.
- Rao, L.; Qian, Y.; Khodabukus, A.; Ribar, T.; Bursac, N. Engineering human pluripotent stem cells into a functional skeletal muscle tissue. Nat. Commun. 2018, 9, 126.
- De Micheli, A.J.; Laurilliard, E.J.; Heinke, C.L.; Ravichandran, H.; Fraczek, P.; Soueid-Baumgarten, S.; De Vlaminck, I.; Elemento, O.; Cosgrove, B.D. Single-Cell Analysis of the Muscle Stem Cell Hierarchy Identifies Heterotypic Communication Signals Involved in Skeletal Muscle Regeneration. Cell Rep. 2020, 30, 3583–3595.e5.
- Dunn, A.; Talovic, M.; Patel, K.; Patel, A.; Marcinczyk, M.; Garg, K. Biomaterial and stem cell-based strategies for skeletal muscle regeneration. J. Orthop. Res. 2019, 37, 1246–1262.
- Yin, H.; Price, F.; Rudnicki, M.A. Satellite Cells and the Muscle Stem Cell Niche. Physiol. Rev. 2013, 93, 23–67.
- Zheng, B.; Cao, B.; Crisan, M.; Sun, B.; Li, G.; Logar, A.; Yap, S.; Pollett, J.B.; Drowley, L.; Cassino, T.; et al. Prospective identification of myogenic endothelial cells in human skeletal muscle. Nat. Biotechnol. 2007, 25, 1025–1034.
- Sirabella, D.; De Angelis, L.; Berghella, L. Sources for skeletal muscle repair: From satellite cells to reprogramming. J. Cachexia Sarcopenia Muscle 2013, 4, 125–136.
- Torrente, Y.; Belicchi, M.; Marchesi, C.; D’Antona, G.; Cogiamanian, F.; Pisati, F.; Gavina, M.; Giordano, R.; Tonlorenzi, R.; Fagiolari, G.; et al. Autologous transplantation of muscle-derived CD133+ stem cells in Duchenne muscle patients. Cell Transplant. 2007, 16, 563–577.
- Asakura, A.; Seale, P.; Girgis-Gabardo, A.; Rudnicki, M.A. Myogenic specification of side population cells in skeletal muscle. J. Cell Boil. 2002, 159, 123–134.
- Joe, A.W.B.; Yi, L.; Natarajan, A.; Le Grand, F.; So, L.; Wang, J.; Rudnicki, M.A.; Rossi, F.M. Muscle injury activates resident fibro/adipogenic progenitors that facilitate myogenesis. Nature 2010, 12, 153–163.
- Wosczyna, M.N.; Rando, T.A. A Muscle Stem Cell Support Group: Coordinated Cellular Responses in Muscle Regeneration. Dev. Cell 2018, 46, 135–143.
- Ostrovidov, S.; Ahadian, S.; Ramon-Azcon, J.; Hosseini, V.; Fujie, T.; Parthiban, S.P.; Shiku, H.; Matsue, T.; Kaji, H.; Ramalingam, M. Three-dimensional co-culture of C2C12/PC12 cells improves skeletal muscle tissue formation and function. J. Tissue Eng. Regen. Med. 2017, 11, 582–595.
- Biferali, B.; Proietti, D.; Mozzetta, C.; Madaro, L. Fibro–Adipogenic Progenitors Cross-Talk in Skeletal Muscle: The Social Network. Front. Physiol. 2019, 10, 10.
- Gao, F.; Chiu, S.M.; Motan, D.A.L.; Zhang, Z.; Chen, L.; Ji, H.-L.; Tse, H.-F.; Fu, Q.-L.; Lian, Q. Mesenchymal stem cells and immunomodulation: Current status and future prospects. Cell Death Dis. 2016, 7, 2062.
- Kim, J.H.; Kim, I.; Seol, Y.-J.; Ko, I.K.; Yoo, J.J.; Atala, A.; Lee, S.J. Neural cell integration into 3D bioprinted skeletal muscle constructs accelerates restoration of muscle function. Nat. Commun. 2020, 11, 1–12.
- Laternser, S.; Keller, H.; Leupin, O.; Rausch, M.; Graf-Hausner, U.; Rimann, M. A Novel Microplate 3D Bioprinting Platform for the Engineering of Muscle and Tendon Tissues. SLAS Technol. Transl. Life Sci. Innov. 2018, 23, 599–613.
- Latroche, C.; Weiss-Gayet, M.; Muller, L.; Gitiaux, C.; Leblanc, P.; Liot, S.; Ben-Larbi, S.; Abou-Khalil, R.; Verger, N.; Bardot, P.; et al. Coupling between Myogenesis and Angiogenesis during Skeletal Muscle Regeneration is Stimulated by Restorative Macrophages. Stem Cell Rep. 2017, 9, 2018–2033.
- Sarrafian, T.L.; Bodine, S.C.; Murphy, B.; Grayson, J.K.; Stover, S.M. Extracellular matrix scaffolds for treatment of large volume muscle injuries: A review. Veter. Surg. 2018, 47, 524–535.
- Anderson, S.E.; Han, W.M.; Srinivasa, V.; Mohiuddin, M.; Ruehle, M.A.; Moon, J.Y.; Shin, E.; Emeterio, C.L.S.; Ogle, M.E.; Botchwey, E.A.; et al. Determination of a Critical Size Threshold for Volumetric Muscle Loss in the Mouse Quadriceps. Tissue Eng. Part C Methods 2019, 25, 59–70.
- Skuk, D.; Caron, N.J.; Goulet, M.; Roy, B.; Tremblay, J.P. Resetting the Problem of Cell Death Following Muscle-Derived Cell Transplantation: Detection, Dynamics and Mechanisms. J. Neuropathol. Exp. Neurol. 2003, 62, 951–967.
- Wolf, M.T.; Dearth, C.L.; Sonnenberg, S.B.; Loboa, E.G.; Badylak, S.F. Naturally derived and synthetic scaffolds for skeletal muscle reconstruction. Adv. Drug Deliv. Rev. 2015, 84, 208–221.
- Corona, B.T.; Ward, C.L.; Baker, H.B.; Walters, J.T.R.; Christ, G.J. Implantation ofIn VitroTissue Engineered Muscle Repair Constructs and Bladder Acellular Matrices Partially RestoreIn VivoSkeletal Muscle Function in a Rat Model of Volumetric Muscle Loss Injury. Tissue Eng. Part A 2013, 20, 705–715.
- Nakayama, K.H.; Quarta, M.; Paine, P.; Alcazar, C.; Karakikes, I.; Garcia, V.; Abilez, O.; Calvo, N.S.; Simmons, C.S.; Rando, T.A.; et al. Treatment of volumetric muscle loss in mice using nanofibrillar scaffolds enhances vascular organization and integration. Commun. Biol. 2019, 2, 170.
- Borselli, C.; Cezar, C.A.; Shvartsman, D.; VanDenburgh, H.H.; Mooney, D.J. The role of multifunctional delivery scaffold in the ability of cultured myoblasts to promote muscle regeneration. Biomaterials 2011, 32, 8905–8914.
- Grasman, J.; Zayas, M.J.; Page, R.L.; Pins, G.D. Biomimetic scaffolds for regeneration of volumetric muscle loss in skeletal muscle injuries. Acta Biomater. 2015, 25, 2–15.
- Matthias, N.; Hunt, S.D.; Wu, J.; Lo, J.; Callahan, L.A.S.; Li, Y.; Huard, J.; Darabi, R. Volumetric muscle loss injury repair using in situ fibrin gel cast seeded with muscle-derived stem cells (MDSCs). Stem Cell Res. 2018, 27, 65–73.
- Kesireddy, V. Evaluation of adipose-derived stem cells for tissue-engineered muscle repair construct-mediated repair of a murine model of volumetric muscle loss injury. Int. J. Nanomed. 2016, 11, 1461–1473.
- Qiu, X.; Liu, S.; Zhang, H.; Zhu, B.; Su, Y.; Zheng, C.; Tian, R.; Wang, M.; Kuang, H.; Zhao, X.; et al. Mesenchymal stem cells and extracellular matrix scaffold promote muscle regeneration by synergistically regulating macrophage polarization toward the M2 phenotype. Stem Cell Res. Ther. 2018, 9, 88.
- Lalegül-Ülker, Ö.; Şeker, Ş.; Elçin, A.E.; Elçin, Y.M. Encapsulation of bone marrow-MSCs in PRP-derived fibrin microbeads and preliminary evaluation in a volumetric muscle loss injury rat model: Modular muscle tissue engineering. Artif. Cells Nanomed. Biotechnol. 2018, 47, 10–21.

