1000/1000
Hot
Most Recent
Glioblastoma (GBM) is the most popular primary central nervous system cancer and has an extremely expansive course. Aggressive tumor growth correlates with short median overall survival (OS) oscillating between 14 and 17 months. The survival rate of patients in a three-year follow up oscillates around 10%. The interaction of the proteins programmed death-1 (PD-1) and programmed cell death ligand (PD-L1) creates an immunoregulatory axis promoting invasion of glioblastoma multiforme cells in the brain tissue. The PD-1 pathway maintains immunological homeostasis and protects against autoimmunity. PD-L1 expression on glioblastoma surface promotes PD-1 receptor activation in microglia, resulting in the negative regulation of T cell responses. Glioblastoma multiforme cells induce PD-L1 secretion by activation of various receptors such as toll like receptor (TLR), epidermal growth factor receptor (EGFR), interferon alpha receptor (IFNAR), interferon-gamma receptor (IFNGR). Binding of the PD-1 ligand to the PD-1 receptor activates the protein tyrosine phosphatase SHP-2, which dephosphorylates Zap 70, and this inhibits T cell proliferation and downregulates lymphocyte cytotoxic activity. Relevant studies demonstrated that the expression of PD-L1 in glioma correlates with WHO grading and could be considered as a tumor biomarker. Studies in preclinical GBM mouse models confirmed the safety and efficiency of monoclonal antibodies targeting the PD-1/PD-L1 axis. Satisfactory results such as significant regression of tumor mass and longer animal survival time were observed. Monoclonal antibodies inhibiting PD-1 and PD-L1 are being tested in clinical trials concerning patients with recurrent glioblastoma multiforme.
Glioblastoma (GBM) is the most common primary cancer in the central nervous system and has an extremely expansive course[1]. The standard approach to glioma treatment consists in the most extensive as possible surgical resection and in adjuvant radiation strengthened by temozolomide (TMZ) administration[2]. The median overall survival (OS) oscillates between 14 and 17 months[3][4]. The survival rate of patients in a three-year follow up oscillates around 10%[5] . GBM resistance to typical therapies requires verification. Glioblastoma cells interact with the surrounding environment, creating forceful interactions among heterogenous cell groups, various chemokines with cytogenetic effects, and extracellular proteins stimulating tumorigenesis, uncontrolled multifocal expansion, and immunological evasion[6].
The proteins programmed death-1 (PD-1) and programmed cell death ligand (PD-L1) interplay, creating an immunoregulatory axis promoting invasion of glioblastoma multiforme cells in the brain tissue[7]. Physiologically, the main function of PD-1 is to restrain T-cell anti-tumor activity and amplify Tregs activation, which limit T-cell reaction and protect against hyper immunity. The PD-L1/PD-1 axis maintains immunological homeostasis and protects against autoimmunity[8].
The binding of PD-1 to the corresponding PD-1 receptor activates the protein tyrosine phosphatase SHP-2, which dephosphorylates Zap 70 (Figure 1). This process T cells proliferation and downregulates lymphocyte cytotoxic activity[9].
Studies revealed that glioma cells are the principal expressors of PD-1 ligands[10]. The presence of PD-L1 was revealed in glioblastoma lines and biopsies in 2003 by Wintterle et al.[11]. Relevant studies demonstrated that the presence of PD-1L in glioma cells correlates with WHO grading and could be considered as a biomarker for glioma cells[12].
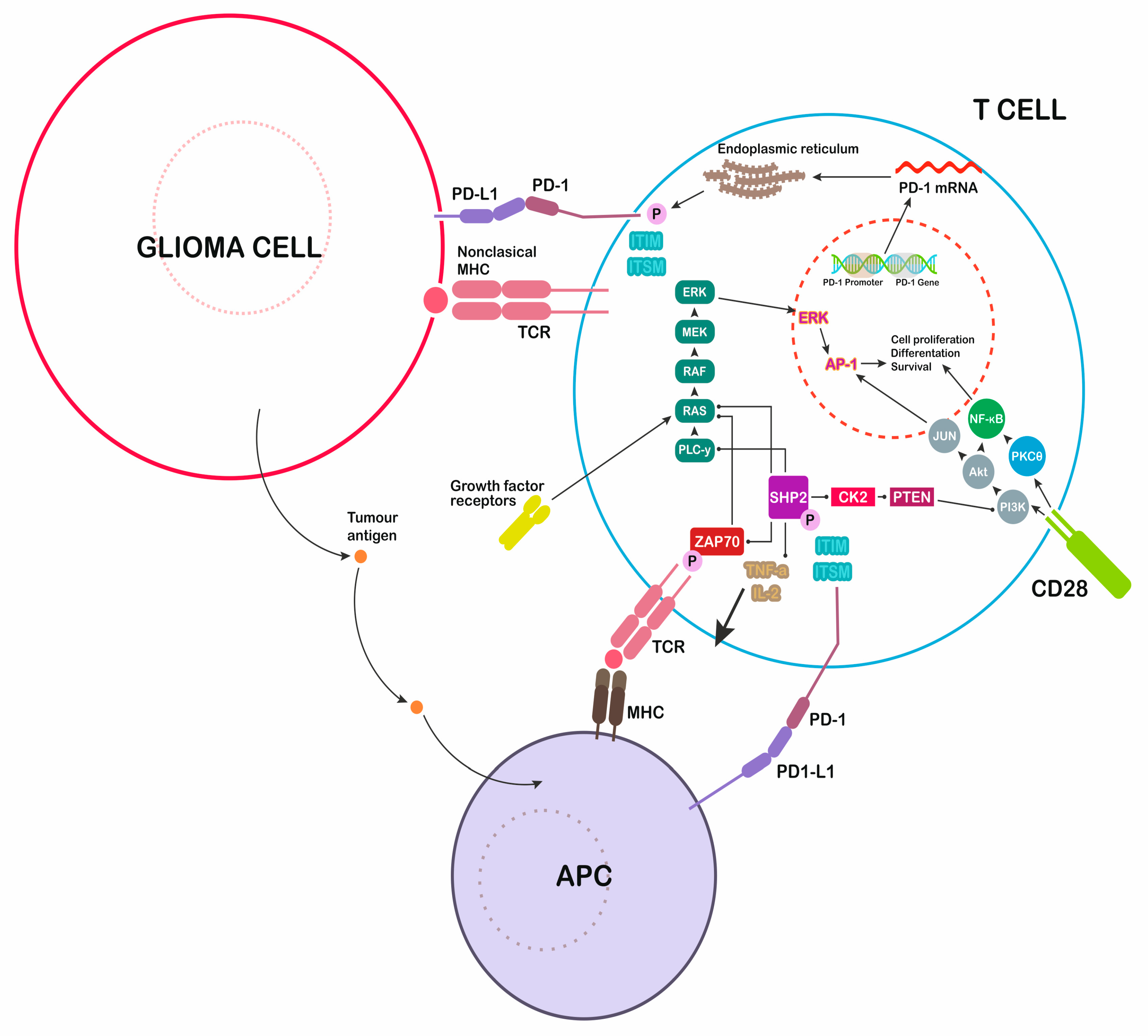
Figure 1. Immunological modulation induced by glioblastoma multiforme (GBM) cells. Secretion of programmed cell death ligand 1 (PD-L1) inhibits the immune attack, blocking T cells responses. PD-1: programmed death-1, major histocompatibility complex: MHC, T-cell receptor: TCR, antigen-presenting cell: APC.
GBM is highly resistant to standard therapies and thus is a challenging disease. Short OS and aggressive intercourse remain uncontrollable when using the typical therapeutic approach. The PD-1L/PD-1 immune check point axis is considered an interesting target for immunotherapy. Many pathways activating PD-L1/PD-1-dependent glioma cell immunoescape were clearly described. Blockade of the interaction between PD-1 and PD-L1 may re-establish proper immunity against GBM. Recent clinical studies on PD-1L/PD-1 inhibitors have presented effective responses. Although trials do not confirm critical extension of OS, these inhibitors may confer different benefits if combined with standard therapies. Further clinical observations are required to create the best therapeutic protocols that can bring a new hope for patients.