 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Alessandra Durazzo | + 694 word(s) | 694 | 2020-01-17 09:10:03 | | | |
| 2 | Nicole Yin | + 2 word(s) | 696 | 2020-10-20 11:46:52 | | | | |
| 3 | Nicole Yin | Meta information modification | 696 | 2020-11-02 05:05:11 | | |
Video Upload Options
The most recent advances on the use of nanoparticles in wound dressing formulations and in tissue engineering for the treatment of burn wound infections.
1. Introduction
An injured skin derived from a burn wound can be classified according to the depth of the thermal damage (classified into four degrees) and the estimation of percentage of total body surface area (TBSA) that has been affected (determined by the rule of nines). The susceptibility to infection is highly influenced by the severity of the damage and may cause, in some more advanced cases, severe lesions to the underlying tissues of the skin. The depth of thermal skin damage is represented in Figure 1.
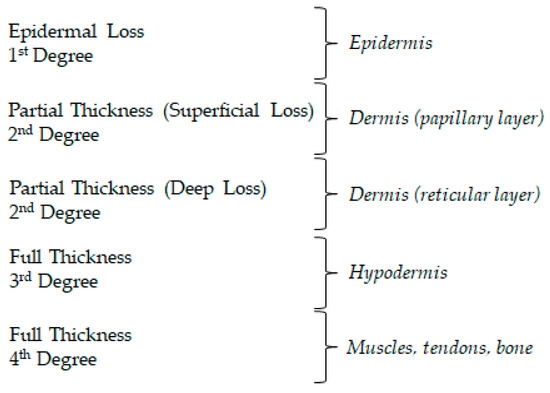
Figure 1. Different degrees of burn wounds and affected skin layers.
2. Pathophysiology
The skin is composed by three primary layers, videlicet epidermis, dermis, and hypodermis. The epidermis is the most external layer that serves as a skin protective barrier against external aggressions and maintains skin hydration and regeneration. Corneocytes, keratinocytes, melanocytes, Langerhans cells, Merkel cells, CD8+ T cells and stem cells are present in epidermis, among which Langerhans cells stand out by its function of antigen presenting cell within the adaptive immune system. The dermis is an irrigated fibrous matrix of collagen, elastin, nerve structures, cutaneous appendages and connective tissue, providing structural support, glandular function and irrigation. Adipocytes, macrophages, fibroblasts, vascular, and nerve systems form the hypodermis and support the above-mentioned layers of tissue.
When skin integrity is compromised by wound injury, a restorative response for cutaneous repair takes place, involving four stages of repair: haemostasis, inflammation, proliferation, and remodelling. In the first stage, vasoconstriction, platelet aggregation and immunity, and complement system activation occur, ceasing the bleeding and activating the coagulation cascade. The clot formation aims to prevent the microorganism invasion. Simultaneously, the inflammation is installed, as the fibrin clot secrets cytokines and growth factors that induce the migration of neutrophils followed by macrophages (differentiated lymphocytes and monocytes) to the wound resulting in the production of reactive oxygen species (ROS) and proteinases, thereby protecting the organism against exogenous microorganisms. The secretion of cytokines will promote a third stage, which upholds cells proliferation, angiogenesis, tissue granulation and ultimately promotes the formation of a temporary extracellular matrix. This mass is then replaced by a mature scar at the remodelling stage of the skin.
This regenerative process is potentially hampered by infection, which can be of fungal or bacterial origin, with the most prevalent microorganisms being Staphylococcus aureus (gram-positive bacteria), Pseudomonas aeruginosa (gram-negative bacteria) and Candida spp. (fungi). Infection constitutes a major concern, as the production of a biofilm in the extracellular matrix protects the microorganisms against conventional antibiotics and is highly associated with hypertrophic scar. After a burn injury, with the thermal destruction of the skin and the haemostasis phase, the burn wound surface takes the form of an a vascular necrotic tissue with high protein content, which results in impaired immune cells migration and provides a favourable environment to microbial invasion and colonization. Gram-positive bacteria of endogenous origin that survive thermal stress, namely Staphylococci, are the first to colonize the burn wound within the first 48 h, followed by other pathogens. The bacteria then initiate several mechanisms of virulent factors production, including host cell adhesion, immune system evasion, nutrient acquisition, which can lead to tissue destruction and systemic invasion if not rapidly intervened. The adhesion and proliferation will later promote the aggregate of microorganisms that secrete an extracellular matrix (slime) rich in proteins and polysaccharides, protecting the complex community from harsh environments in a biofilm.
Antibiotherapy, both topical and systemic, plays an important role in the prevention and treatment of wound infections. However, systemic antibiotics are highly associated with mechanisms of resistance, which compromise the treatment process. For local wound treatment, the deeper extension of the burn and increasing eschar thickness, the less reliable is the administration of systemic antibiotics to the eschar. Therefore, topical antibiotics emerge as an alternative treatment, as these contribute to a “high and sustained concentration of the antimicrobial at the site of the infection”. Despite their potential benefits, the results obtained with topical antibiotherapy are still “suboptimal”, which reinforces the need of innovation in topical antibiotic delivery systems.


