Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 2 | Rita Xu | + 2704 word(s) | 2704 | 2021-08-05 10:08:57 | | | |
| 3 | Conner Chen | Meta information modification | 2704 | 2021-10-11 09:55:50 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Martínez, V. Urinary Tract Infections. Encyclopedia. Available online: https://encyclopedia.pub/entry/12723 (accessed on 07 February 2026).
Martínez V. Urinary Tract Infections. Encyclopedia. Available at: https://encyclopedia.pub/entry/12723. Accessed February 07, 2026.
Martínez, Vicente. "Urinary Tract Infections" Encyclopedia, https://encyclopedia.pub/entry/12723 (accessed February 07, 2026).
Martínez, V. (2021, August 03). Urinary Tract Infections. In Encyclopedia. https://encyclopedia.pub/entry/12723
Martínez, Vicente. "Urinary Tract Infections." Encyclopedia. Web. 03 August, 2021.
Copy Citation
Urinary tract infections (UTIs) affect any part of the urinary tract and may spread through the urinary tract towards the urethra, bladder and even the kidneys and they are associated with an increase in morbidity and mortality. UTIs may be resolved spontaneously or treated with antibiotics. However, regular use of antibiotics is related to nephrotoxicity and produces changes in the intestinal flora, alter immunity and metabolism, and finally, gut bacteria become a reservoir of genes for resistance to antibiotics. Regarding this concern, a new group of molecules called drug conjugates have been proposed as an alternative or a complement to de use of just antibiotics such as a new adjuvant in UTIs therapy called Itxasol©.
urinary tract infections
arbutin
umbelliferon
N-acetyl l-cysteine
1. Introduction
Urinary tract infections (UTIs) affect any part of the urinary tract and may spread through the urinary tract towards the urethra, bladder and even the kidneys [1]. It has been estimated that around 150 million people suffer from UTIs annually [2], and they are associated with an increase in morbidity and mortality [3]. UTIs are more prevalent in women than in men, which is related to the short length of the urethra favoring bacteria colonization [4][5][6], and it has been estimated that 50–70% of women will suffer at least one urinary infection in their life [6]. Of women suffering from UTIs, 20–30% might suffer from a recurrent UTI, which is defined as recurrences of uncomplicated and/or complicated UTIs, with a frequency of at least three UTIs/year or two UTIs in the last six months [7]. UTIs in women are often associated with sexual intercourse [8], poor social conditions that limit access to female hygiene products for menstruation [9] and use of contraceptive devices such as diaphragms [10][11]. In the case of postmenopausal women, recurrent UTIs are related to the low levels of estrogens that produce changes in the vaginal microbiota [12]. In the case of men, UTIs are often related to prostatitis, prostate benign hyperplasia or any kind of urinary obstructive tract pathology [13][14]. In addition, UTIs are related to smoking, which is also associated with the development of bladder cancer, and it has been reported to increase the risk of suffering from UTIs by up to 50% [15].
The main bacteria isolated from cases of UTIs (80%) is E. coli, although other pathogens have been cultured, such as Klebsiella pneumoniae and Pseudomonas aeruginosa [16]. These infections represent a major number of hospital- and community-acquired infections, acute pyelonephritis being one of the major causes of hospitalization [6][17].
Causes of UTIs are related to sexual intercourse [18], and the incidence increases with age [19]. Other manifestations of UTIs are cystitis and pyelonephritis [20]. UTIs are often associated with the use of catheters [20][21], this being a major risk factor in hospital-acquired UTIs. UTIs are also related with radical cystectomy that is used for the treatment of different kinds of bladder cancer [22]. It has been estimated that around 35% of the patients after radical cystectomy surgery suffer from UTIs [23][24]. Of note, there are multiples cases of asymptomatic bacteriuria that do not require treatment, and they are not considered UTIs [6].
UTIs may be resolved spontaneously or treated with antibiotics [25]. Antibiotic resistance is a major problem nowadays [26]; in the European Union alone, it has been reported that annually, there are around 670,000 cases of infections related to multi-drug-resistant bacteria with 37,000 associated deaths, representing an enormous socioeconomic burden [27]. Regular use of antibiotics is related to nephrotoxicity due to interstitial nephritis, acute tubular necrosis and intratubular crystal deposition, which leads to an impaired kidney function [28]. Antibiotics also produce changes in the intestinal flora that trigger pathological processes, such as diarrhea, and alter immunity and metabolism; furthermore, gut bacteria have become a reservoir of genes for resistance to antibiotics [25].
As in other cases, UTI reinfections are recurrent, which leads to antibiotic resistance and, therefore, complications in treatment [29][30]. The recurrence of UTIs varies among different populations [16]. Children and young adult women usually suffer from having UTIs after a brief period following initial diagnosis [31][32].
Treatment of UTIs depends on various factors, such as the severity of the illness and the sex and age of the patient. The main first-line treatments are nitrofurantoin, fosfomycin trometamol, pivmecillinam and trimethoprim/sulfamethoxazole (TMP-SMX), with beta-lactams and fluoroquinolones being alternative therapies [33][34]. However, antibiotic usage produces nephrotoxicity in the case of gentamicin [35]. In addition, the occurrence of antibiotic resistance in UTIs is common [36][37], and this resistance is related to an increase in mortality due to microbial infections [38][39][40]. Moreover, regarding the use of antibiotics in patients with urothelial carcinoma, it has also been reported that patients under antibiotic treatment show a worse survival rate than that those who do not receive antibiotics [38].
One of the major problems related to the efficacy of antibiotics is the creation of biofilm by bacteria and fungus [41][42]. Biofilm promotes the propagation of these organisms and helps them to be more resistant to pharmacological treatments [43][44]. It has also been demonstrated that the formation of the biofilm plays a key role in catheter-associated infection [45]. This situation combined with the lack of new antibiotics requires effort to identify alternatives that might be used to combat recurrent infections. Regarding this concern, a new group of molecules called drug conjugates have been proposed as an alternative or a complement to the use of antibiotics alone [46]. These drug conjugates combine a sustained release, different kinds of antibiotics, and antibacterial activities as well as carrier composition [47].
It is important to underline that antibiotics come from natural sources and have been used to treat infections since ancient times. A milestone was reached with the discovery of penicillin by Sir Alexander Fleming in 1928 [48][49][50]. In this regard, Itxasol© is a new drug with a biomimetic origin that has recently been authorized by the Spanish Drugs Agency that belongs to Health Ministry (Agencia Española del Medicamento, authorization number C.N. 203621.5) to be used to treat UTIs as an adjuvant. Biomimetic might be defined as the science that studies nature as a source of inspiration for innovative technologies to solve human problems through models of systems (mechanics), processes (chemistry) or elements that imitate or are inspired by nature [51].
Itxasol© is composed of β-arbutin, umbelliferon (UMB) and N-acetyl l-cysteine (NAC). The three components of Itxasol© act as a natural antibiotic and potentially reduce inflammation, biofilm formation and the number of pathogenic microorganisms in the urinary tract.
2. β-arbutin
Arbutin is a glycoside derived from extracts of leaves of Arctostaphylos uva-ursi, plants from genus Bergenia or other plants that belong to genus Ainsliaea and Calluna. These plants have been traditionally used for the treatment of urinary tract infections in Europe, America and Asiatic countries [52]. After its administration, arbutin is transformed into hydroquinone and glucose (Figure 1). The mechanism of action of hydroquinone (HQ) is related to the destruction of the bacteria wall, which leads to leakage of intracellular content and bacteria death [53]. One of the major advantages of β-arbutin treatment is that the amount of derived HQ that might reach the urinary tract after HQ excretion in urine is around 65% of the β-arbutin administrated [54].
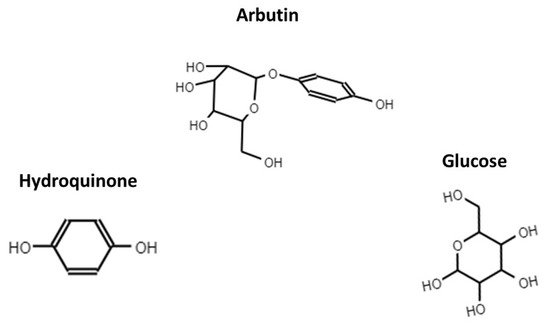
Figure 1. Chemical structure of arbutin, hydoquinone and D-Glucose.
The antibacterial activity of β-arbutin has been tested in several studies that demonstrated that it can destroy both Gram-negative and positive bacteria as well as fungi. In this list, we can find Pseudomonas aeruginosa, Staphylococcus aureus, S. aureus MRSA K31 (clinical, antibiotic-resistant strain), Enterococcus faecalis, Escherichia coli, Escherichia coli ESBL R194 (clinical, antibiotic-resistant strain), Enterococcus faecalis HLAR (clinical, antibiotic-resistant strain), Bacillus subtilis and Candida albicans [53][55][56]. In Table 2, we show the minimum inhibitory concentration of HQ against different pathogens.
Table 2. Main MIC values for HQ.
| Pathogen | MIC (μg/mL) | Gram | Reference |
|---|---|---|---|
| Escherichia coli | 256 | Negative | [57] |
| Pseudomonas aeruginosa | 7.8 | Negative | [58] |
| Staphylococcus aureus | 15.6 | Positive | [58] |
| Staphylococcus aureus | 103 | Positive | [59] |
| Salmonella typhimurium | 512 | Negative | [57] |
| Bacillus cereus | 512 | Positive | [57] |
| Mycobacterium tuberculosis | 12.5 | Positive | [60] |
In fact, in vivo, it has been reported in a randomized controlled trial that β-arbutin in combination with other plant extracts, such as berberine and birch, significantly reduced the incidence of recurrent cystitis [61]. The use of β-arbutin as a substitute for antibiotic treatment for UTIs is under study in a double-blind, randomized and controlled clinical trial on women aged 15 to 75 years old, but the results are yet to be published [62].
One concern regarding the safety of arbutin is that hydroquinone might be nephrotoxic [63][64]. Extract of strawberry tree Arbutus unedo, which contains arbutin, has been proven to be safe for the kidney in rats [65]. These extracts did not show any side effects in kidney function or affect the integrity of the DNA in the kidney cells. It has also been demonstrated that the administration of arbutin to humans was not toxic for lymphocytes, and it did not induce damage to the DNA of these cells [66].
Inflammation is an important consequence of UTIs. Regarding this effect, it has been demonstrated that β-arbutin reduces the kidney inflammation produced by the administration of lipopolysaccharide to rats. It was concluded that the anti-inflammatory effects of β-arbutin were mediated by inhibition of the Akt signaling pathway [67]. These results were dependent on the activity of arbutin, because when a specific arbutin activity inhibitor was administered, the beneficial effects of arbutin were abolished. Of note, arbutin, in a polyherbal mixture administered to diabetic rats, resulted in a decrease in blood sugar and level of cholesterol as well as cardiovascular risk, while it restored several histopathological changes produced by diabetes in the liver, pancreas and kidney [68]. The main actions of β-arbutin are summarized in Table 3.
Table 3. Main actions of β-arbutin.
| Action | Main Findings/Use | Reference |
|---|---|---|
| Antibacterial action | Inhibits Pseudomonas aeruginosa growth at 128 mg/mL | [56] |
| Demonstration of antibacterial activity | [55] | |
| Arbutin destroys bacteria through wall cellular disruption (Gram + and Gram −) | [53] | |
| Reduction in bacterial load in prevention of UTI recurrence | [61] | |
| Clinical trial to reduce the use of antibiotics administering b-arbutin (results not yet published) | [62] | |
| Anti-inflammatory | Attenuated damage induced by lipopolysaccharide in rat | [67] |
| Anti-diabetic | Ameliorates hyperglycemia, hyperlipidemia and histopathological changes in pancreas, kidney and liver in a diabetes rat model | [68] |
3. Umbelliferon (UMB)
UMB (Figure 2) is a coumarin (7-hydroxycoumarin) that can be extracted from fruits [2] and plants and has demonstrated multiple activities, such as antitumoral, antioxidant (with the ability to quench free radicals), antihyperglycemic, anti-arthritic and anti-inflammatory activities, as well as hepatic and cerebral protective functions [17][69][70][71][72][73][74][75].
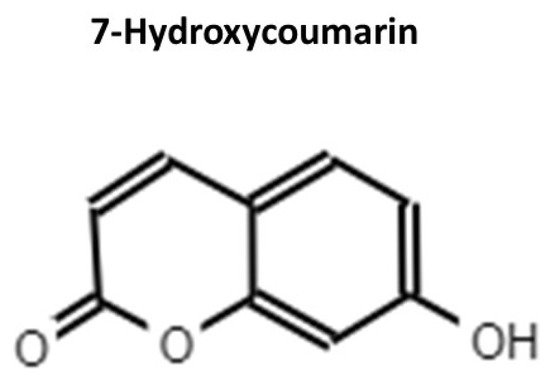
Figure 2. Chemical structure of UMB.
UMB activity as an antibiotic was described as earlier as 1978. However, it has not been used due to a lack of knowledge about its mechanism of action and its actions in the kidney [46]. Although knowledge of the antibiotic action of UMB is scarce, it has recently been demonstrated that derivates of UMB from plants of genus Ferula are useful against periodontal bacteria, inhibiting bacteria growth and biofilm formation [76]. In agreement with these data, it has been described that UMB can inhibit the formation of the biofilm created by Staphylococcus epidermidis, impairing intracellular adhesion by downregulation in the expressions of genes related to adherence function [77]. The MIC of UMB against different pathogens is shown in Table 4.
Table 4. Main MIC values for UMB.
Coumarins are useful against fungus such as C. albicans [80][81]. Thus, this efficacy might lie in the fact that UMB can produce internal changes, such as an increase in ROS, DNA fragmentation and externalization of phosphatidyl serine, all of them being related to an increase in apoptosis [82]. The use of UMB to stop biofilm production in a model of C. elegans showed downregulation of the expression of genes related to the formation of filaments and adhesion as well as reducing the formation of biofilm in this nematode in general [83]. Besides fungi, it has also been reported that coumarins reduce the virulence and biofilm formation of E. coli O157:H7. Coumarins downregulate the expression of curli and motility genes, which results in fewer fimbriae and the production of biofilm [84]. In the same sense, UMB prevents the formation of biofilm by the methicillin-resistant Staphylococcus epidermidis strain at a dose of 500 mg/mL but without affecting the growth of this bacteria [77].
UMB has also been reported as a good nephron protector when it is used in combination with cisplatin, which is one of the chemotherapeutic agents used against different cancers but with limited use given its nephrotoxicity [85]. In a mouse model of cisplatin-induced acute kidney injury (AKI), it was demonstrated that UMB reduced the nephrotoxicity associated with cisplatin use. These effects were achieved by increased cell tubular proliferation upon enhanced expression of sox9 transcription factor. Another kidney-protective effect of UMB was the reduction of necrosis in kidney cells produced by the inhibition of the RIPK1/RIPK3/MLKL pathway. In a model of methotrexate-induced kidney injury, the administration of UMB reduced the expression of inflammation mediators P38MAPK and NF-κB and the pro-apoptotic molecules BAS and caspase3 while increasing anti-apoptotic levels of the BLC-2 molecule [86].
On the other hand, UMB has proven useful in treating the nephropathy produced in diabetic rat models induced with streptozotocin. In this model, UMB reduced the creatinine level in plasma, renal oxidative stress levels and levels of tissue and circulating TGF-β1 [1]. In another similar rat model study, in addition to the reduction of glucose blood levels, the beneficial effects of UMB were related to a decrease in inflammatory mediators, such as TNF-α, IL-6 and IL-1β; a reduction in the levels of mesenchymal–epithelial markers, such as podocin and CD2AP; and the reversal of some of the histopathological changes mediated by a diabetic status in the kidney [87]. In fact, this inhibition of the TGF-β1 pathway has also been reported in carbon tetrachloride-induced liver fibrosis in rats. After treatment with UMB, liver cells reduced the activation of the Smad/TGF-β1 pathway; downregulated the expression of NF-κB, collagen I and III and α-Smad; increased the levels of glutathione; and upregulated the expression of PPARγ. The histology result was a decrease in liver fibrosis [88]. The principal actions of UMB are summarized in Table 5.
Table 5. Main actions of coumarins and their derivates.
| Action | Main Findings/Use | References |
|---|---|---|
| Antifungicidal/antibiotic | Antifungicidal activity | [74][82][83] |
| Decreases virulence and biofilm formation of E.coli O157:H7 | [84] | |
| Impedes biofilm formation of methicillin-resistant Staphylococcus epidermidis | [77] | |
| Destroys periodontal bacteria and inhibits biofilm formation | [76] | |
| Antibiofilm properties (Staphylococcus epidermidis) | [77] | |
| Antitumoral | Inhibits cell growth in lung carcinoma cell lines | [73] |
| Induces cell cycle arrest in G0/G1 in human cell carcinoma | [75] | |
| Anti-inflammatory | Reduction in inflammation in a model of brain damage in rats | [17] |
| Antihyperglycemic | Anti-diabetic effect in a diabetic mouse model induced with streptozotocin | [89] |
| Nephron protection | Reduction in the nephrotoxicity associated to cisplatin use | [85] |
| UMB attenuates renal toxicity induced by gentamicin | [1][86] | |
| Enhances renal function in diabetic mouse model | [87] | |
| Antifibrotic | Ameliorates the liver fibrosis signs induced by carbon tetrachloride (CCl4) in rats | [88] |
4. N-Acetyl L-Cysteine (NAC)
The NAC molecule (Figure 3) is well known for its antioxidant, anti-inflammatory and mucolytic actions [90][91]. Its mechanism of action is related to its ability to reduce the levels of reactive oxygen species (ROS), such as •OH, NO2 and CO3−, given that it is a precursor of glutathione, a renowned natural ROS scavenger [92]. Moreover, there is compelling evidence regarding NAC as a molecule that destroys biofilms and also reduces their formation via bacteria and fungus [93][94]. Although the mechanism by which NAC reduces biofilm formation is still not clear, a recent report by Li and co-workers demonstrated that NAC can penetrate the bacteria wall, stopping protein synthesis and leading to bacteria death [95]. Table 6 summarizes the recent reports demonstrating the ability of NAC to both inhibit biofilm formation and destroy already formed ones. Besides being useful against UTIs, several pieces of evidence point out NAC as a kidney protector [96]. Moreover, a recent study demonstrated that the administration of NAC protected Wistar rats with a kidney injury against long warm renal ischemia. In particular, NAC administration resulted in an improvement in biochemical parameters and renal function when compared to the placebo group [97].
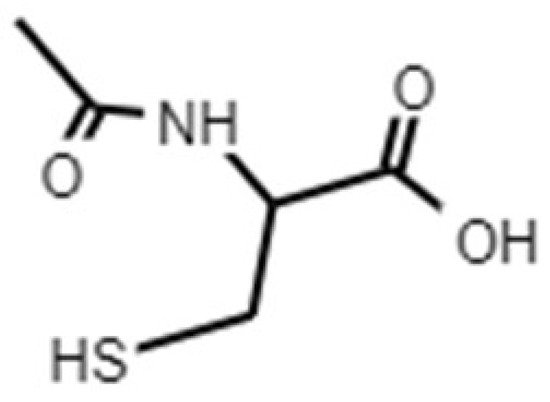
Figure 3. Chemical structure of NAC.
Table 6. Recent reported studies on antibiofilm activities of NAC.
| Organism | NAC Concentration | Reference |
|---|---|---|
| C. albicans C. parapsilosis C. guilliermondii C. tropicalis C. glabrata |
10–50 mg/mL | [96] |
| Pseudomonas aeruginosa | 0.15–0.23 mg/mL | [98] |
| P. aeruginosa | 3–10 mg/mL | [99] |
| P. aeruginosa | 32 mg/mL | [100] |
| Candida albicans | 25 mg/mL | [101] |
| Staphylococcus aureus | 0.5 mg/mL | [102] |
| Stenotrophomonas maltophilia | 16–32 mg/mL | [103] |
| Acinetobacter baumannii | 16–128 mg/mL | [104] |
| Candida tropicalis | 1000 mg/mL | [105] |
| Actinomyces naeslundii, Lactobacillus salivarius, Streptococcus mutans, Enterococcus faecalis | 25–100 mg/mL | [106] |
| Pseudomonas aeruginosa | 10 mg/mL | [107] |
| Staphylococcus pseudintermedius Pseudomonas aeruginosa Corynebacterium spp. and β-hemolytic Streptococcus spp. | 0.115–80 mg/mL | [108] |
| Actinomyces naeslundii, Lactobacillus salivarius, Streptococcus mutans, Enterococcus faecalis | 0.78–1.56 mg/mL | [109] |
References
- Garud, M.S.; Kulkarni, Y.A. Attenuation of renal damage in type I diabetic rats by umbelliferone—A coumarin derivative. Pharmacol. Rep. 2017, 69, 1263–1269.
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284.
- Gandaglia, G.; Varda, B.; Sood, A.; Pucheril, D.; Konijeti, R.; Sammon, J.D.; Sukumar, S.; Menon, M.; Sun, M.; Chang, S.L.; et al. Short-term perioperative outcomes of patients treated with radical cystectomy for bladder cancer included in the National Surgical Quality Improvement Program (NSQIP) database. J. Can. Urol. Assoc. 2014, 8, E681–E687.
- Foxman, B. The epidemiology of urinary tract infection. Nat. Rev. Urol. 2010, 7, 653–660.
- Czajkowski, K.; Broś-Konopielko, M.; Teliga-Czajkowska, J. Urinary tract infection in women. Prz. Menopauzalny 2021, 20, 40–47.
- Geerlings, S.E. Clinical Presentations and Epidemiology of Urinary Tract Infections. Microbiol. Spectr. 2016, 4, 4–5.
- Albert, X.; Huertas, I.; Pereiro, I.; Sanfélix, J.; Gosalbes, V.; Perrotta, C. Antibiotics for preventing recurrent urinary tract infection in non-pregnant women. Cochrane Database Syst. Rev. 2004, 2004, CD001209.
- Scholes, D. Risk factors for recurrent urinary tract infection in young women. J. Infect. Dis. 2000, 182, 1177–1182.
- Mathiyalagen, P.; Peramasamy, B.; Vasudevan, K.; Basu, M.; Cherian, J.; Sundar, B. A descriptive cross-sectional study on menstrual hygiene and perceived reproductive morbidity among adolescent girls in a union territory, India. J. Fam. Med. Prim. Care 2017, 6, 360.
- Lindh, I.; Othman, J.; Hansson, M.; Ekelund, A.C.; Svanberg, T.; Strandell, A. New types of diaphragms and cervical caps versus older types of diaphragms and different gels for contraception: A systematic review. BMJ Sex. Reprod. Health 2020, 47, e12.
- Behzadi, P.; Behzadi, E.; Pawlak-Adamska, E.A. Urinary tract infections (UTIs) or genital tract infections (GTIs)? It’s the diagnostics that count. GMS Hyg. Infect. Control 2019, 14, Doc14.
- Jung, C.; Brubaker, L. The etiology and management of recurrent urinary tract infections in postmenopausal women. Climacteric 2019, 22, 242–249.
- Hooton, T.M.; Scholes, D.; Hughes, J.P.; Winter, C.; Roberts, P.L.; Stapleton, A.E.; Stergachis, A.; Stamm, W.E. A Prospective Study of Risk Factors for Symptomatic Urinary Tract Infection in Young Women. N. Engl. J. Med. 1996, 335, 468–474.
- Etienne, M.; Galperine, T.; Caron, F. Urinary Tract Infections in Older Men. N. Engl. J. Med. 2016, 374, 2191–2192.
- Lenis, A.T.; Lec, P.M.; Chamie, K. Bladder cancer a review. JAMA J. Am. Med. Assoc. 2020, 324, 1980–1991.
- Foxman, B. Urinary tract infection syndromes. Occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect. Dis. Clin. N. Am. 2014, 28, 1–13.
- Germoush, M.O.; Othman, S.I.; Al-Qaraawi, M.A.; Al-Harbi, H.M.; Hussein, O.E.; Al-Basher, G.; Alotaibi, M.F.; Elgebaly, H.A.; Sandhu, M.A.; Allam, A.A.; et al. Umbelliferone prevents oxidative stress, inflammation and hematological alterations, and modulates glutamate-nitric oxide-cGMP signaling in hyperammonemic rats. Biomed. Pharmacother. 2018, 102, 392–402.
- Nicolle, L.E.; Harding, G.K.M.; Preiksaitis, J.; Ronald, A.R. The association of urinary tract infection with sexual intercourse. J. Infect. Dis. 1982, 146, 579–583.
- Detweiler, K.; Mayers, D.; Fletcher, S.G. Bacteruria and Urinary Tract Infections in the Elderly. Urol. Clin. N. Am. 2015, 42, 561–568.
- Anger, J.T.; Saigal, C.S.; Wang, M.M.; Yano, E.M. Urologic Disease Burden in the United States: Veteran Users of Department of Veterans Affairs Healthcare. Urology 2008, 72, 37–41.
- Linsenmeyer, T.A. Catheter-associated urinary tract infections in persons with neurogenic bladders. J. Spinal Cord Med. 2018, 41, 132–141.
- Ghoreifi, A.; Van Horn, C.M.; Xu, W.; Cai, J.; Miranda, G.; Bhanvadia, S.; Schuckman, A.K.; Daneshmand, S.; Djaladat, H. Urinary tract infections following radical cystectomy with enhanced recovery protocol: A prospective study. Urol. Oncol. Semin. Orig. Investig. 2020, 38, 75.e9–75.e14.
- Clark, P.E.; Agarwal, N.; Biagioli, M.C.; Eisenberger, M.A.; Greenberg, R.E.; Herr, H.W.; Inman, B.A.; Kuban, D.A.; Kuzel, T.M.; Lele, S.M.; et al. Bladder cancer: Clinical practice guidelines in oncology. JNCCN J. Natl. Compr. Cancer Netw. 2013, 11, 446–475.
- Shigemura, K.; Tanaka, K.; Matsumoto, M.; Nakano, Y.; Shirakawa, T.; Miyata, M.; Yamashita, M.; Arakawa, S.; Fujisawa, M. Post-operative infection and prophylactic antibiotic administration after radical cystectomy with orthotopic neobladderurinary diversion. J. Infect. Chemother. 2012, 18, 479–484.
- Griebling, T.L. Urologic diseases in America project: Trends in resource use for urinary tract infections in women. J. Urol. 2005, 173, 1281–1287.
- Ventola, C.L. The antibiotic resistance crisis: Causes and threats. Pharm. Ther. J. 2015, 40, 277–283.
- Kakoullis, L.; Papachristodoulou, E.; Chra, P.; Panos, G. Mechanisms of antibiotic resistance in important gram-positive and gram-negative pathogens and novel antibiotic solutions. Antibiotics 2021, 10, 415.
- Morales-Alvarez, M.C. Nephrotoxicity of Antimicrobials and Antibiotics. Adv. Chronic Kidney Dis. 2020, 27, 31–37.
- Barber, A.E.; Norton, J.P.; Spivak, A.M.; Mulvey, M.A. Urinary tract infections: Current and emerging management strategies. Clin. Infect. Dis. 2013, 57, 719–724.
- Waller, T.A.; Pantin, S.A.L.; Yenior, A.L.; Pujalte, G.G.A. Urinary Tract Infection Antibiotic Resistance in the United States. Prim. Care Clin. Off. Pract. 2018, 45, 455–466.
- Foxman, B.; Gillespie, B.; Koopman, J.; Zhang, L.; Palin, K.; Tallman, P.; Marsh, J.V.; Spear, S.; Sobel, J.D.; Marty, M.J.; et al. Risk factors for second urinary tract infection among college women. Am. J. Epidemiol. 2000, 151, 1194–1205.
- Salo, J.; Uhari, M.; Helminen, M.; Korppi, M.; Nieminen, T.; Pokka, T.; Kontiokari, T. Cranberry juice for the prevention of recurrences of urinary tract infections in children: A randomized placebo-controlled trial. Clin. Infect. Dis. 2012, 54, 340–346.
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, e103–e120.
- Pietrucha-Dilanchian, P.; Hooton, T.M. Diagnosis, Treatment, and Prevention of Urinary Tract Infection. Microbiol. Spectr. 2016, 4.
- Blunston, M.A.; Yonovitz, A.; Woodahl, E.L.; Smolensky, M.H. Gentamicin-induced ototoxicity and nephrotoxicity vary with circadian time of treatment and entail separate mechanisms. Chronobiol. Int. 2015, 32, 1223–1232.
- Pitout, J.D.D. Extraintestinal pathogenic Escherichia coli: A combination of virulence with antibiotic resistance. Front. Microbiol. 2012, 3, 9.
- Asadi Karam, M.R.; Habibi, M.; Bouzari, S. Urinary tract infection: Pathogenicity, antibiotic resistance and development of effective vaccines against Uropathogenic Escherichia coli. Mol. Immunol. 2019, 108, 56–67.
- Hopkins, A.M.; Kichenadasse, G.; Karapetis, C.S.; Rowland, A.; Sorich, M.J. Concomitant Antibiotic Use and Survival in Urothelial Carcinoma Treated with Atezolizumab. Eur. Urol. 2020, 78, 540–543.
- Zilberberg, M.D.; Shorr, A.F.; Micek, S.T.; Vazquez-Guillamet, C.; Kollef, M.H. Multi-drug resistance, inappropriate initial antibiotic therapy and mortality in Gram-negative severe sepsis and septic shock: A retrospective cohort study. Crit. Care 2014, 18, 596.
- Teillant, A.; Gandra, S.; Barter, D.; Morgan, D.J.; Laxminarayan, R. Potential burden of antibiotic resistance on surgery and cancer chemotherapy antibiotic prophylaxis in the USA: A literature review and modelling study. Lancet Infect. Dis. 2015, 15, 1429–1437.
- Rabin, N.; Zheng, Y.; Opoku-Temeng, C.; Du, Y.; Bonsu, E.; Sintim, H.O. Biofilm formation mechanisms and targets for developing antibiofilm agents. Future Med. Chem. 2015, 7, 493–512.
- Hall, C.W.; Mah, T.F. Molecular mechanisms of biofilm-based antibiotic resistance and tolerance in pathogenic bacteria. FEMS Microbiol. Rev. 2017, 41, 276–301.
- Goel, N.; Fatima, S.W.; Kumar, S.; Sinha, R.; Khare, S.K. Antimicrobial resistance in biofilms: Exploring marine actinobacteria as a potential source of antibiotics and biofilm inhibitors. Biotechnol. Rep. 2021, 30, e00613.
- Atriwal, T.; Azeem, K.; Husain, F.M.; Hussain, A.; Khan, M.N.; Alajmi, M.F.; Abid, M. Mechanistic Understanding of Candida albicans Biofilm Formation and Approaches for Its Inhibition. Front. Microbiol. 2021, 12, 932.
- Liu, L.; Shi, H.; Yu, H.; Yan, S.; Luan, S. The recent advances in surface antibacterial strategies for biomedical catheters. Biomater. Sci. 2020, 8, 4074–4087.
- Cal, P.M.S.D.; Matos, M.J.; Bernardes, G.J.L. Trends in therapeutic drug conjugates for bacterial diseases: A patent review. Expert Opin. Ther. Pat. 2017, 27, 179–189.
- Ibrahim, M.A.; Panda, S.S.; Birs, A.S.; Serrano, J.C.; Gonzalez, C.F.; Alamry, K.A.; Katritzky, A.R. Synthesis and antibacterial evaluation of amino acid-antibiotic conjugates. Bioorg. Med. Chem. Lett. 2014, 24, 1856–1861.
- Lima, L.M.; da Silva, B.N.M.; Barbosa, G.; Barreiro, E.J. β-lactam antibiotics: An overview from a medicinal chemistry perspective. Eur. J. Med. Chem. 2020, 208, 112829.
- Piddock, L.J.V. The crisis of no new antibiotics-what is the way forward? Lancet Infect. Dis. 2012, 12, 249–253.
- Sengupta, S.; Chattopadhyay, M.K.; Grossart, H.P. The multifaceted roles of antibiotics and antibiotic resistance in nature. Front. Microbiol. 2013, 4, 47.
- Vincent, J.F.V.; Bogatyreva, O.A.; Bogatyrev, N.R.; Bowyer, A.; Pahl, A.K. Biomimetics: Its practice and theory. J. R. Soc. Interface 2006, 3, 471–482.
- Sticher, O.; Soldati, F.; Lehmann, D. High-performance liquid chromatographic separation and quantitative determination of arbutin, methylarbutin, hydroquinone and hydroquinone-monomethylether in Arctostaphylos, Bergenia, Calluna and Vaccinium species (author’s transl). Planta Med. 1979, 35, 253–261.
- Ma, C.; He, N.; Zhao, Y.; Xia, D.; Wei, J.; Kang, W. Antimicrobial Mechanism of Hydroquinone. Appl. Biochem. Biotechnol. 2019, 189, 1291–1303.
- Schindler, G.; Patzak, U.; Brinkhaus, B.; Von Nieciecki, A.; Wittig, J.; Krähmer, N.; Glöckl, I.; Veit, M. Urinary excretion and metabolism of arbutin after oral administration of Arctostaphylos uvae ursi extract as film-coated tablets and aqueous solution in healthy humans. J. Clin. Pharmacol. 2002, 42, 920–927.
- Żbikowska, B.; Franiczek, R.; Sowa, A.; Połukord, G.; Krzyzanowska, B.; Sroka, Z. Antimicrobial and Antiradical Activity of Extracts Obtained from Leaves of Five Species of the Genus Bergenia: Identification of Antimicrobial Compounds. Microb. Drug Resist. 2017, 23, 771–780.
- Ng, T.B.; Ling, J.M.L.; Wang, Z.T.; Cai, J.N.; Xu, G.J. Examination of coumarins, flavonoids and polysaccharopeptide for antibacterial activity. Gen. Pharmacol. 1996, 27, 1237–1240.
- Kim, M.H.; Jo, S.H.; Ha, K.S.; Song, J.H.; Jang, H.D.; Kwon, Y.I. Antimicrobial activities of 1,4-benzoquinones and wheat germ extract. J. Microbiol. Biotechnol. 2010, 20, 1204–1209.
- Jeyanthi, V.; Velusamy, P.; Kumar, G.V.; Kiruba, K. Effect of naturally isolated hydroquinone in disturbing the cell membrane integrity of Pseudomonas aeruginosa MTCC 741 and Staphylococcus aureus MTCC 740. Heliyon 2021, 7, e07021.
- Rúa, J.; Fernández-Álvarez, L.; De Castro, C.; Del Valle, P.; De Arriaga, D.; García-Armesto, M.R. Antibacterial activity against foodborne Staphylococcus aureus and antioxidant capacity of various pure phenolic compounds. Foodborne Pathog. Dis. 2011, 8, 149–157.
- Jyoti, A.; Nam, K.-W.; Jang, W.S.; Kim, Y.-H.; Kim, S.-K.; Lee, B.-E.; Song, H.-Y. Antimycobacterial activity of methanolic plant extract of Artemisia capillaris containing ursolic acid and hydroquinone against Mycobacterium tuberculosis. J. Infect. Chemother. 2016, 22, 200–208.
- Genovese, C.; Davinelli, S.; Mangano, K.; Tempera, G.; Nicolosi, D.; Corsello, S.; Vergalito, F.; Tartaglia, E.; Scapagnini, G.; Di Marco, R. Effects of a new combination of plant extracts plus d-mannose for the management of uncomplicated recurrent urinary tract infections. J. Chemother. 2018, 30, 107–114.
- Afshar, K.; Fleischmann, N.; Schmiemann, G.; Bleidorn, J.; Hummers-Pradier, E.; Friede, T.; Wegscheider, K.; Moore, M.; Gágyor, I. Reducing antibiotic use for uncomplicated urinary tract infection in general practice by treatment with uva-ursi (REGATTA)—A double-blind, randomized, controlled comparative effectiveness trial. BMC Complement. Altern. Med. 2018, 18, 203.
- Adesunloye, B.A. Acute renal failure due to the herbal remedy CKLS. Am. J. Med. 2003, 115, 506–507.
- Nowak, A.K.; Shilkin, K.B.; Jeffrey, G.P. Darkroom hepatitis after exposure to hydroquinone. Lancet 1995, 345, 1187.
- Jurica, K.; Benković, V.; Sikirić, S.; Brčić Karačonji, I.; Kopjar, N. The effects of strawberry tree (Arbutus unedo L.) water leaf extract and arbutin upon kidney function and primary DNA damage in renal cells of rats. Nat. Prod. Res. 2020, 34, 2354–2357.
- Jurica, K.; Brčić Karačonji, I.; Mikolić, A.; Milojković-Opsenica, D.; Benković, V.; Kopjar, N. In vitro safety assessment of the strawberry tree (Arbutus unedo L.) water leaf extract and arbutin in human peripheral blood lymphocytes. Cytotechnology 2018, 70, 1261–1278.
- Zhang, B.; Zeng, M.; Li, B.; Kan, Y.; Wang, S.; Cao, B.; Huang, Y.; Zheng, X.; Feng, W. Arbutin attenuates LPS-induced acute kidney injury by inhibiting inflammation and apoptosis via the PI3K/Akt/Nrf2 pathway. Phytomedicine 2021, 82, 153466.
- Madić, V.; Petrović, A.; Jušković, M.; Jugović, D.; Djordjević, L.; Stojanović, G.; Vasiljević, P. Polyherbal mixture ameliorates hyperglycemia, hyperlipidemia and histopathological changes of pancreas, kidney and liver in a rat model of type 1 diabetes. J. Ethnopharmacol. 2021, 265, 113210.
- Hoult, J.R.S.; Payá, M. Pharmacological and biochemical actions of simple coumarins: Natural products with therapeutic potential. Gen. Pharmacol. 1996, 27, 713–722.
- Kumar, V.; Anwar, F.; Verma, A.; Mujeeb, M. Therapeutic effect of umbelliferon-α-D-glucopyranosyl-(2I→1II)-α-D-glucopyranoside on adjuvant-induced arthritic rats. J. Food Sci. Technol. 2015, 52, 3402–3411.
- Kumar, V.; Ahmed, D.; Verma, A.; Anwar, F.; Ali, M.; Mujeeb, M. Umbelliferone β-D-galactopyranoside from Aegle marmelos (L.) corr. An ethnomedicinal plant with antidiabetic, antihyperlipidemic and antioxidative activity. BMC Complement. Altern. Med. 2013, 13, 273.
- Li, H.; Yao, Y.; Li, L. Coumarins as potential antidiabetic agents. J. Pharm. Pharmacol. 2017, 69, 1253–1264.
- Lopez-Gonzalez, J.S.; Prado-Garcia, H.; Aguilar-Cazares, D.; Molina-Guarneros, J.A.; Morales-Fuentes, J.; Mandoki, J.J. Apoptosis and cell cycle disturbances induced by coumarin and 7-hydroxycoumarin on human lung carcinoma cell lines. Lung Cancer 2004, 43, 275–283.
- Navarro-García, V.M.; Rojas, G.; Avilés, M.; Fuentes, M.; Zepeda, G. In vitro antifungal activity of coumarin extracted from Loeselia mexicana Brand. Mycoses 2011, 54, e569–e571.
- Vijayalakshmi, A.; Sindhu, G. Umbelliferone arrest cell cycle at G0/G1 phase and induces apoptosis in human oral carcinoma (KB) cells possibly via oxidative DNA damage. Biomed. Pharmacother. 2017, 92, 661–671.
- Amin, A.; Hanif, M.; Abbas, K.; Ramzan, M.; Rasheed, A.; Zaman, A.; Pieters, L. Studies on effects of umbelliferon derivatives against periodontal bacteria; antibiofilm, inhibition of quorum sensing and molecular docking analysis. Microb. Pathog. 2020, 144, 104184.
- Swetha, T.K.; Pooranachithra, M.; Subramenium, G.A.; Divya, V.; Balamurugan, K.; Pandian, S.K. Umbelliferone Impedes Biofilm Formation and Virulence of Methicillin-Resistant Staphylococcus epidermidis via Impairment of Initial Attachment and Intercellular Adhesion. Front. Cell. Infect. Microbiol. 2019, 9, 357.
- Cruz, L.F.; de Figueiredo, G.F.; Pedro, L.P.; Amorin, Y.M.; Andrade, J.T.; Passos, T.F.; Rodrigues, F.F.; Souza, I.L.A.; Gonçalves, T.P.R.; Lima, L.A.R.D.S.; et al. Umbelliferone (7-hydroxycoumarin): A non-toxic antidiarrheal and antiulcerogenic coumarin. Biomed. Pharmacother. 2020, 129, 110432.
- Monte, J.; Abreu, A.C.; Borges, A.; Simões, L.C.; Simões, M. Antimicrobial Activity of Selected Phytochemicals against Escherichia coli and Staphylococcus aureus and Their Biofilms. Pathogens 2014, 3, 473–498.
- Hu, X.-L.; Xu, Z.; Liu, M.-L.; Feng, L.-S.; Zhang, G.-D. Recent Developments of Coumarin Hybrids as Anti-fungal Agents. Curr. Top. Med. Chem. 2017, 17, 3219–3231.
- Kumar, R.; Saha, A.; Saha, D. A new antifungal coumarin from Clausena excavata. Fitoterapia 2012, 83, 230–233.
- Jia, C.; Zhang, J.; Yu, L.; Wang, C.; Yang, Y.; Rong, X.; Xu, K.; Chu, M. Antifungal activity of coumarin against Candida albicans is related to apoptosis. Front. Cell. Infect. Microbiol. 2019, 9, 445.
- Xu, K.; Wang, J.L.; Chu, M.P.; Jia, C. Activity of coumarin against Candida albicans biofilms. J. Mycol. Med. 2019, 29, 28–34.
- Lee, J.H.; Kim, Y.G.; Cho, H.S.; Ryu, S.Y.; Cho, M.H.; Lee, J. Coumarins reduce biofilm formation and the virulence of Escherichia coli O157:H7. Phytomedicine 2014, 21, 1037–1042.
- McSweeney, K.R.; Gadanec, L.K.; Qaradakhi, T.; Ali, B.A.; Zulli, A.; Apostolopoulos, V. Mechanisms of cisplatin-induced acute kidney injury: Pathological mechanisms, pharmacological interventions, and genetic mitigations. Cancers 2021, 13, 1572.
- Hassanein, E.H.M.; Ali, F.E.M.; Kozman, M.R.; Abd El-Ghafar, O.A.M. Umbelliferone attenuates gentamicin-induced renal toxicity by suppression of TLR-4/NF-κB-p65/NLRP-3 and JAK1/STAT-3 signaling pathways. Environ. Sci. Pollut. Res. 2021, 28, 11558–11571.
- Wang, H.Q.; Wang, S.S.; Chiufai, K.; Wang, Q.; Cheng, X.L. Umbelliferone ameliorates renal function in diabetic nephropathy rats through regulating inflammation and TLR/NF-κB pathway. Chin. J. Nat. Med. 2019, 17, 346–354.
- Mahmoud, A.M.; Hozayen, W.G.; Hasan, I.H.; Shaban, E.; Bin-Jumah, M. Umbelliferone Ameliorates CCl4-Induced Liver Fibrosis in Rats by Upregulating PPARγ and Attenuating Oxidative Stress, Inflammation, and TGF-β1/Smad3 Signaling. Inflammation 2019, 42, 1103–1116.
- Kumar, V.; Ahmed, D.; Anwar, F.; Ali, M.; Mujeeb, M. Enhanced glycemic control, pancreas protective, antioxidant and hepatoprotective effects by umbelliferon-α-D-glucopyranosyl-(2I→1II)-α-Dglucopyranoside in streptozotocin induced diabetic rats. SpringerPlus 2013, 2, 1–20.
- Aldini, G.; Altomare, A.; Baron, G.; Vistoli, G.; Carini, M.; Borsani, L.; Sergio, F. N-Acetylcysteine as an antioxidant and disulphide breaking agent: The reasons why. Free Radic. Res. 2018, 52, 751–762.
- Tardiolo, G.; Bramanti, P.; Mazzon, E. Overview on the effects of N-acetylcysteine in neurodegenerative diseases. Molecules 2018, 23, 3305.
- Samuni, Y.; Goldstein, S.; Dean, O.M.; Berk, M. The chemistry and biological activities of N-acetylcysteine. Biochim. Biophys. Acta Gen. Subj. 2013, 1830, 4117–4129.
- Blasi, F.; Page, C.; Rossolini, G.M.; Pallecchi, L.; Matera, M.G.; Rogliani, P.; Cazzola, M. The effect of N-acetylcysteine on biofilms: Implications for the treatment of respiratory tract infections. Respir. Med. 2016, 117, 190–197.
- Dinicola, S.; De Grazia, S.; Carlomagno, C.; Pintucci, J.P. N-acetylcysteine as powerful molecule to destroy bacterial biofilms. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 2942–2948.
- Li, X.; Kim, J.; Wu, J.; Ahamed, A.I.; Wang, Y.; Martins-Green, M. N-Acetyl-cysteine and Mechanisms Involved in Resolution of Chronic Wound Biofilm. J. Diabetes Res. 2020, 2020, 9589507.
- Kelly, A.M.; Dwamena, B.; Cronin, P.; Bernstein, S.J.; Carlos, R.C. Meta-analysis: Effectiveness of drugs for preventing contrast-induced nephropathy. Ann. Intern. Med. 2008, 148, 284–294.
- Aydin, A.; Sunay, M.M.; Karakan, T.; Özcan, S.; Hasçiçek, A.M.; Yardimci, İ.; Surer, H.; Korkmaz, M.; Hücümenoğlu, S.; Huri, E. The examination of the nephroprotective effect of montelukast sodium and N-acetylcysteine ın renal ıschemia with dimercaptosuccinic acid imaging in a placebo-controlled rat model. Acta Cir. Bras. 2020, 35, 1–9.
- Guerini, M.; Grisoli, P.; Pane, C.; Perugini, P. Microstructured lipid carriers (MLC) based on N-acetylcysteine and chitosan preventing Pseudomonas Aeruginosa biofilm. Int. J. Mol. Sci. 2021, 22, 891.
- Kundukad, B.; Udayakumar, G.; Grela, E.; Kaur, D.; Rice, S.A.; Kjelleberg, S.; Doyle, P.S. Weak acids as an alternative anti-microbial therapy. Biofilm 2020, 2, 100019.
- Lababidi, N.; Montefusco-Pereira, C.V.; de Souza Carvalho-Wodarz, C.; Lehr, C.M.; Schneider, M. Spray-dried multidrug particles for pulmonary co-delivery of antibiotics with N-acetylcysteine and curcumin-loaded PLGA-nanoparticles. Eur. J. Pharm. Biopharm. 2020, 157, 200–210.
- Nunes, T.S.B.S.; Rosa, L.M.; Vega-Chacón, Y.; de Oliveira Mima, E.G. Fungistatic action of N-acetylcysteine on Candida albicans biofilms and its interaction with antifungal agents. Microorganisms 2020, 8, 980.
- Pijls, B.G.; Sanders, I.M.J.G.; Kuijper, E.J.; Nelissen, R.G.H.H. Synergy between induction heating, antibiotics, and N-acetylcysteine eradicates Staphylococcus aureus from biofilm. Int. J. Hyperth. 2020, 37, 130–136.
- Pollini, S.; Di Pilato, V.; Landini, G.; Di Maggi, T.; Cannatelli, A.; Sottotetti, S.; Cariani, L.; Aliberti, S.; Blasi, F.; Sergio, F.; et al. In vitro activity of N-acetylcysteine against Stenotrophomonas maltophilia and Burkholderia cepacia complex grown in planktonic phase and biofilm. PLoS ONE 2018, 13, e0203941.
- Feng, J.; Liu, B.; Xu, J.; Wang, Q.; Huang, L.; Ou, W.; Gu, J.; Wu, J.; Li, S.; Zhuo, C.; et al. In vitro effects of N-acetylcysteine alone and combined with tigecycline on planktonic cells and biofilms of Acinetobacter baumannii. J. Thorac. Dis. 2018, 10, 212–218.
- Fernández-Rivero, M.E.; Del Pozo, J.L.; Valentín, A.; de Diego, A.M.; Pemán, J.; Cantón, E. Activity of amphotericin B and anidulafungin combined with rifampicin, clarithromycin, ethylenediaminetetraacetic acid, N-acetylcysteine, and farnesol against Candida tropicalis biofilms. J. Fungi 2017, 3, 16.
- Choi, Y.S.; Kim, C.; Moon, J.H.; Lee, J.Y. Removal and killing of multispecies endodontic biofilms by N-acetylcysteine. Braz. J. Microbiol. 2018, 49, 184–188.
- Kundukad, B.; Schussman, M.; Yang, K.; Seviour, T.; Yang, L.; Rice, S.A.; Kjelleberg, S.; Doyle, P.S. Mechanistic action of weak acid drugs on biofilms. Sci. Rep. 2017, 7, 4783.
- May, E.R.; Conklin, K.A.; Bemis, D.A. Antibacterial effect of N-acetylcysteine on common canine otitis externa isolates. Vet. Dermatol. 2016, 27, 188-e47.
- Moon, J.H.; Choi, Y.S.; Lee, H.W.; Heo, J.S.; Chang, S.W.; Lee, J.Y. Antibacterial effects of N-acetylcysteine against endodontic pathogens. J. Microbiol. 2016, 54, 322–329.
More
Information
Subjects:
Urology & Nephrology
Contributor
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
3.2K
Revisions:
2 times
(View History)
Update Date:
11 Oct 2021
Table of Contents



Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No