 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Tadashi Nishimura | + 2107 word(s) | 2107 | 2021-06-08 12:16:35 | | | |
| 2 | Lily Guo | Meta information modification | 2107 | 2021-06-09 02:50:46 | | | | |
| 3 | Lily Guo | Meta information modification | 2107 | 2021-06-09 02:53:28 | | |
Video Upload Options
Cartilage conduction (CC) is a form of conduction that allows a relatively loud sound to be audible when a transducer is placed on the aural cartilage. The CC transmission mechanism has gradually been elucidated, allowing for the development of CC hearing aids (CC-HAs), which are clinically available in Japan. However, CC is still not fully understood.
1. Introduction
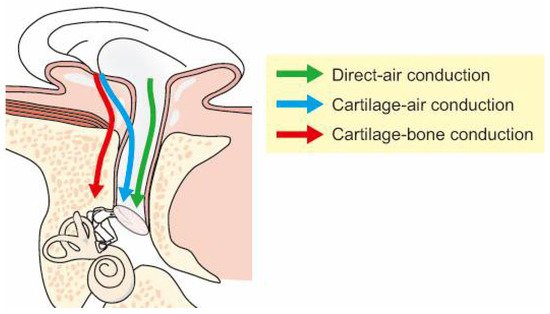
The sound transmission pathway to the cochlea is generally classified into air and bone conduction (AC and BC). For AC, sound generated outside the ear travels to the eardrum through the ear canal and is transduced into vibrations of the ossicles to reach the cochlea. For BC, skull bone vibrations induced by a transducer are transmitted to the cochlea, involving at least five components [1,2,3]. Sound can also be perceived by body part vibrations other than the skull bone [4,5,6], and the transmission mechanisms are unique from one another. When the transducer is placed on the aural cartilage, particularly on the tragus, a relatively loud sound is audible [7]. This form of conduction is referred to as cartilage conduction (CC) [8]. Generally, hearing through non-osseous soft tissue conduction is not as clear as conventional BC. However, a clear sound is audible in CC, and it is perceived louder than when a transducer is placed on the mastoid or forehead [9].
2. The Theoretical CC Transmission Pathway
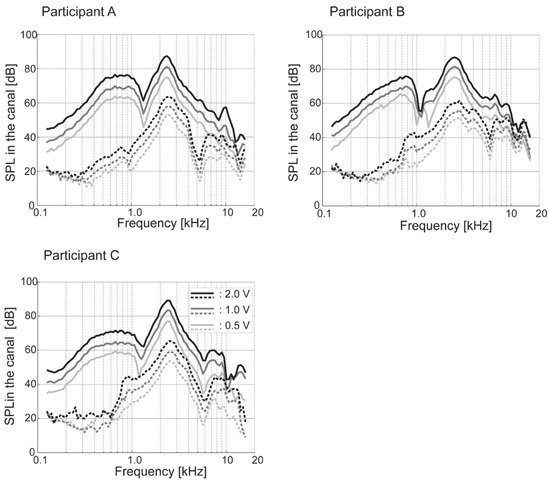
3. Sound Pressure Level in the Ear Canal via CC
The measurement of the sound level in the ear canal similar to real-ear measurements [3] contributes towards understanding the phenomenon. objectively demonstrated the loudness increase by measuring the sound pressure level in the ear canal using a probe microphone (Figure 2) [4]. Conversely, to reproduce the difference in the sound pressure level in the ear canal between the attached and unattached conditions, not only the bony portion of the ear canal but also the cartilaginous portion was necessary to consider [5]. The airborne sound generated by a simulated cartilaginous portion (movable plate) played an important role in the reproduction of the sound pressure level in a simulated ear canal.
4. Hearing Threshold Measurements via CC
4.1. Threshold Shift with an Earplug
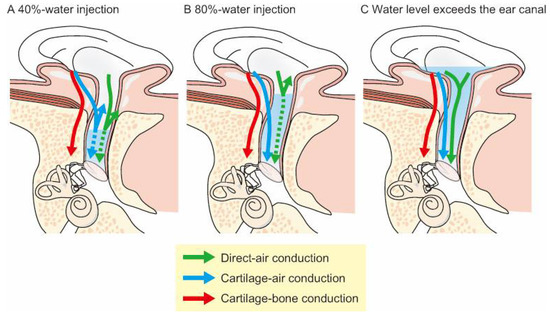
4.2. Threshold Shift with Water Injected into the Ear Canal
5. CC in Pathological Ears
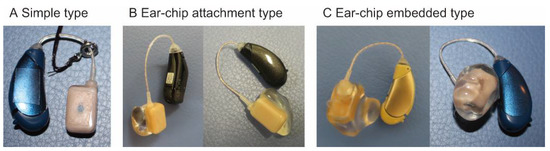
6. CC Applications
References
- Stenfelt, S.; Goode, R.L. Bone-conducted sound: Physiological and clinical aspects. Otol. Neurotol. 2005, 26, 1245–1261.
- Stenfelt, S. Acoustic and physiologic aspects of bone conduction hearing. Adv. Otorhinolaryngol. 2011, 71, 10–21.
- Stenfelt, S. Model predictions for bone conduction perception in the human. Hear. Res. 2016, 340, 135–143.
- Sohmer, H.; Freeman, S.; Geal-Dor, M.; Adelman, C.; Savion, I. Bone conduction experiments in humans—A fluid pathway from bone to ear. Hear. Res. 2000, 146, 81–88.
- Watanabe, T.; Bertoli, S.; Probst, R. Transmission pathways of vibratory stimulation as measured by subjective thresholds and distortion-product otoacoustic emissions. Ear Hear. 2008, 29, 667–673.
- Ito, T.; Röösli, C.; Kim, C.J.; Sim, J.H.; Huber, A.M.; Probst, R. Bone conduction thresholds and skull vibration measured on the teeth during stimulation at different sites on the human head. Audiol. Neurootol. 2011, 16, 12–22.
- Blondé-Weinmann, C.; Joubaud, T.; Zimpfer, V.; Hamery, P.; Roth, S. Characterization of cartilage implication in protected hearing perception during direct vibro-acoustic stimulation at various locations. Appl. Acoust. 2021, 179, 108074.
- Hosoi, H. Approach in the Use of Cartilage Conduction Speaker. Japanese Patent 4541111, 17 November 2004.
- Hosoi, H.; Nishimura, T.; Shimokura, R.; Kitahara, T. Cartilage conduction as the third pathway for sound transmission. Auris Nasus Larynx 2019, 46, 151–159.
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Matsui, T.; Yamanaka, T.; Levitt, H. Is cartilage conduction classified into air or bone conduction? Laryngoscope 2014, 124, 1214–1219.
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Yamanaka, T.; Kitahara, T.; Levitt, H. Cartilage conduction is characterized by vibrations of the cartilaginous portion of the ear canal. PLoS ONE 2015, 10, e0120135.
- Gazia, F.; Galletti, B.; Portelli, D.; Alberti, G.; Freni, F.; Bruno, R.; Galletti, F. Real ear measurement (REM) and auditory performances with open, tulip and double closed dome in patients using hearing aids. Eur. Arch. Otorhinolaryngol. 2020, 277, 1289–1295.
- Shimokura, R.; Hosoi, H.; Nishimura, T.; Yamanaka, T.; Levitt, H. Cartilage conduction hearing. J. Acoust. Soc. Am. 2014, 135, 1959–1966.
- Shimokura, R.; Hosoi, H.; Nishimura, T.; Iwakura, T.; Yamanaka, T. Simulating cartilage conduction sound to estimate the sound pressure level in the external auditory canal. J. Sound Vib. 2015, 20, 261–268.
- Levitt, H. Transformed up-down methods in psychoacoustics. J. Acoust. Soc. Am. 1971, 49, 467–477.
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Matsui, T.; Yamanaka, T.; Kitahara, T.; Levitt, H. Cartilage conduction efficiently generates airborne sound in the ear canal. Auris Nasus Larynx 2015, 42, 15–19.
- Miyamae, R.; Nishimura, T.; Hosoi, H.; Saito, O.; Shimokura, R.; Yamanaka, T.; Kitahara, T. Perception of speech in cartilage conduction. Auris Nasus Larynx 2017, 44, 26–32.
- Nishimura, T.; Miyamae, R.; Hosoi, H.; Saito, O.; Shimokura, R.; Yamanaka, T.; Kitahara, T. Frequency characteristics and speech recognition in cartilage conduction. Auris Nasus Larynx 2019, 46, 709–715.
- Nishimura, T.; Hosoi, H.; Saito, O.; Akasaka, S.; Shimokura, R.; Yamanaka, T.; Kitahara, T. Effect of fixation place on airborne sound in cartilage conduction. J. Acoust. Soc. Am. 2020, 148, 469.
- Morimoto, C.; Nishimura, T.; Hosoi, H.; Saito, O.; Fukuda, F.; Shimokura, R.; Yamanaka, T. Sound transmission by cartilage conduction in ear with fibrotic aural atresia. J. Rehabil. Res. Dev. 2014, 51, 325–332.
- Hosoi, H.; Yanai, S.; Nishimura, T.; Sakaguchi, T.; Iwakura, T.; Yoshino, K. Development of cartilage conduction hearing aid. Arch. Mat. Sci. Eng. 2010, 42, 104–110.
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Matsui, T.; Iwakura, T. Benefit of a new hearing device utilizing cartilage conduction. Auris Nasus Larynx 2013, 40, 440–446.
- Shimokura, R.; Hosoi, H.; Iwakura, T.; Nishimura, T.; Matsui, T. Development of monaural and binaural behind-the-ear cartilage conduction hearing aids. Appl. Acoust. 2013, 74, 1234–1240.
- Nishimura, T.; Hosoi, H.; Morimoto, C.; Kitahara, T. Indications of hearing levels for cartilage conduction hearing aids: Evaluation using 2 cm3 coupler and an artificial mastoid. Pediatr. Otorhinolaryngol. Jpn. 2020, 41, 34–40.
- House, J.W.; Kutz, J.W., Jr.; Chung, J.; Fisher, L.M. Bone-anchored hearing aid subjective benefit for unilateral deafness. Laryngoscope 2010, 120, 601–607.
- Lo, J.F.W.; Tsang, W.S.S.; Yu, J.Y.K.; Ho, O.Y.M.; Ku, P.K.M.; Tong, M.C.F. Contemporary hearing rehabilitation options in patients with aural atresia. BioMed Res. Int. 2014, 2014, 761579.
- Riss, D.; Arnoldner, C.; Baumgartner, W.D.; Blineder, M.; Flak, S.; Bachner, A.; Gstoettner, W.; Hamzavi, J.S. Indication criteria and outcomes with the Bonebridge transcutaneous bone-conduction implant. Laryngoscope 2014, 124, 2802–2806.
- Ikeda, R.; Hidaka, H.; Murata, T.; Miyazaki, H.; Katori, Y.; Kobayashi, T. Vibrant Soundbridge implantation via a retrofacial approach in a patient with congenital aural atresia. Auris Nasus Larynx 2019, 46, 204–209.
- Oh, S.J.; Goh, E.K.; Choi, S.W.; Lee, S.; Lee, H.M.; Lee, I.W.; Kong, S.K. Audiologic, surgical and subjective outcomes of active transcutaneous bone conduction implant system (Bonebridge). Int. J. Audiol. 2019, 58, 956–963.
- Curca, I.A.; Parsa, V.; Macpherson, E.A.; Scollie, S.; Vansevenant, K.; Zimmerman, K.; Lewis-Teeter, J.; Allen, P.; Parnes, L.; Agrawal, S. Audiological outcome measures with the BONEBRIDGE transcutaneous bone conduction hearing implant: Impact of noise, reverberation and signal processing features. Int. J. Audiol. 2020, 59, 556–565.
- Kwak, S.H.; Moon, Y.M.; Nam, G.S.; Bae, S.H.; Kim, S.H.; Jung, J.; Choi, J.Y. Clinical Experience of Vibroplasty With Direct Coupling to the Oval Window Without Use of a Coupler. Laryngoscope 2020, 130, E926–E932.
- Vickers, D.; Canas, A.; Degun, A.; Briggs, J.; Bingham, M.; Toner, J.; Cooper, H.; Rogers, S.; Cooper, S.; Irving, R.; et al. Evaluating the effectiveness and reliability of the Vibrant Soundbridge and Bonebridge auditory implants in clinical practice: Study design and methods for a multi-centre longitudinal observational study. Contemp. Clin. Trials Commun. 2018, 10, 137–140.
- Kruyt, I.J.; Bakkum, K.H.E.; Caspers, C.J.I.; Hol, M.K.S. The efficacy of bone-anchored hearing implant surgery in children: A systematic review. Int. J. Pediatr. Otorhinolaryngol. 2020, 132, 109906.
- Zawawi, F.; Kabbach, G.; Lallemand, M.; Daniel, S.J. Bone-anchored hearing aid: Why do some patients refuse it? Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 232–234.


