1. Introduction
Several genes present a potential target for studying breast cancer, The genes studied have been listed in Table 1, and the signaling pathways of these genes were mentioned in Figure 1.
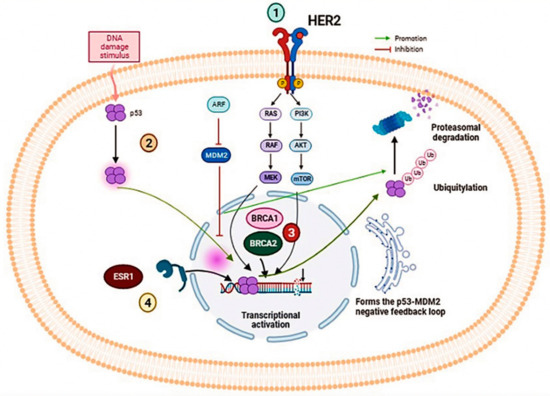
Figure 1. Illustration of several signaling pathways implicated in the oncogenesis of breast cancer. (1) ERBB2 associated protein HER2 signaling pathway, (2) p53 protein implicated in the apoptosis, (3) BRCA1/2 couple implicated in DNA repair mechanisms such as Homologous recombination, (4) ESR1 engaged as a transcription factor.
Table 1. Summary of molecular and clinical utility of ctDNA in breast cancer.
| Gene |
Patient Cohort |
Molecule Testing Technique |
Main Findings |
Clinical Significance |
References |
| ESR1 |
541 postmenopausal women with a diagnosis of MBC. |
Analyzed ESR1 mutations (Y537S and D538G) on cell-free DNA (cfDNA) using droplet digital polymerase chain reaction (ddPCR). |
D538G (21.1%)
Y537S (13.3%)
30 had both mutations. |
These mutations were associated with shorter overall survival:
- wild-type, 32.1 months
- D538G, 25.99 months
- Y537S, 19.98 months
- Both mutations, 15.15 months. |
[72] |
| |
86 estrogen receptor-positive BC patients.185 plasma samples (151 plasma samples from 69 MBC patients, and 34 plasma samples from 17 primary BC (PBC) patients). |
Multiplex droplet digital PCR assays in a snapshot and serially. |
cfDNA ESR1 and PIK3CA mutations were found in 28.9% and 24.6% of MBC patients, respectively. |
All patients with ESR1 mutations had resistance to prior AI (aromatase inhibitor) therapy.
85% of patients with ESR1 mutations had resistance to prior SERM (Selective estrogen receptor modulators) therapy. |
[73] |
| BRCA1/2 |
828 patients with advanced breast, ovarian, prostate, or pancreatic cancer.
(the study was conducted in accordance with the Declaration of Helsinki). |
Plasma-based NGS assay. |
Of 828 patients, 60 (7.2%) had at least one BRCA1/2 loss-of-function mutation, 42 patients with germline mutations and 18 (14 patients had breast cancer) with somatic mutations only. |
NGS analysis of cfDNA identified high rates of therapeutically relevant mutations, including deleterious BRCA1/2 somatic mutations missed by germline testing. |
[74] |
| |
24 patients with proven BRCA1/2 germline mutations (19 ovarian cancer patients and 5 patients with MBC who received prior treatment with platinum-based chemotherapy and/or PARP inhibitors). |
Targeted massively parallel sequencing of tumor DNA from ovarian cancer patients, cfDNA from ovarian and breast cancer patients, and their germline DNA. |
Identification of BRCA1 or BRCA2 reversion mutations in the cfDNA of 4 ovarian cancer patients (21%) and 2 breast cancer patients (40%). |
cfDNA sequencing can help identify putative BRCA1/2 reversion mutations which may facilitate patient selection for PARP inhibition therapy. |
[75] |
| PIK3CA |
Thirty patients with advanced BC (ABC); |
PIK3CA mutation analysis was performed using ddPCR. |
The presence of a PI3K mutation in liquid biopsy correlates with worse PFS in patients with ABC receiving CDK4/6i. |
Integration of PI3K status assessment with other molecular information could improve the management of patients with aggressive breast cancer and better suggest the best therapeutic strategy. |
[76] |
| TP53 |
46 patients with nonmetastatic triple-negative breast cancer; |
Characterization of TP53 gene mutations in tumor tissue through massively parallel sequencing (MPS). Monitoring of previously characterized mutations based on ctDNA analysis by ddPCR at four time points: pre-NCT, post-cycle, pre-surgery, and post-surgery. |
Results show a marked decrease in ctDNA levels and positivity rate during chemotherapy cycles. |
The high prevalence of TP53 mutations in TNBC is a potential biomarker for ctDNA monitoring during NCT, and therefore is a tool for TNBC management. |
[77] |
| |
113 lung and 18 breast cancer patients |
NGS analysis of ctDNA: Panel for hot spot regions in 11 genes for lung cancer and 10 genes for breast cancer. |
Variations in the TP53 gene were detected at a high frequency in both tumor types, followed by the PIK3CA gene in breast cancer. |
Based on NGS and ddPCR techniques, liquid biopsy could be a very effective method for managing terminal cancer cases and monitoring treatment responses. |
[78] |
| |
68 patients with metastatic breast cancer (MBC). |
cfDNA and gDNA (Genomic DNA) analysis by next-generation sequencing (NGS) |
TP53 mutations occurred in 10 (45.45%) TNBC patients, 9 (36.00%) HER2+ patients, and 7 (22.22%) HR+ patients.
TP53 represents the gene with the highest number of somatic mutations. |
Mutations in TP53 cDNA and PIK3CA genes likely limit survival and promote disease progression. |
[79] |
| ERBB2 |
636 women with HER2 nonamplified MBC. |
ctDNA analysis by NGS. |
Results of this study indicate the efficacy of neratinib for HER2-mutated nonamplified breast cancer. |
This study supports the potential use of ctDNA to identify patients with HER2-mutated breast cancer to establish a new standard of care. |
[80] |
| |
Multicohort, phase 2a, platform trial of ctDNA testing in 18 UK hospitals.1051 patients were registered in the study. |
ddPCR and NGS are used to detect ctDNA mutations.
Patients were recruited into four parallel treatment cohorts corresponding to the mutations identified in the ctDNA (ESR1; HER2; AKT1 and PTEN). |
The findings of this study demonstrate the clinically relevant activity of targeted therapies against rare HER2 and AKT1 mutations. |
The results of this research show that ctDNA analysis, with the technologies used in this study, is accurate enough to be routinely adopted into clinical practice. |
[81] |
2. BRCA1/2 Genes
Breast cancer with
BRCA mutations is characterized by its aggressiveness,
BRCA1 mutated breast cancer is frequently high grade and triple negative,
BRCA2 related breast cancer is on average of a higher histological grade than sporadic cases [
82]. Somatic mutations in
BRCA1/2 occur in approximately 3% of all sporadic breast cancers [
83].
The
BRCA1 gene encodes a nuclear phosphoprotein that acts as a tumor suppressor gene by maintaining genomic stability [
84]. The encoded protein combines with other tumor suppressors, DNA damage sensors, and signal transducers to form a large multi-unit protein complex known as the
BRCA1 genome-associated surveillance complex [
85].
The
BRCA2 gene is involved in the maintenance of genomic stability and more specifically the homologous recombination (HR) pathway that repairs double-stranded DNA breaks.
BRCA2 is located on chromosome 13q12.13, it is a large gene comprising 27 exons coding for 3418 amino acids [
86].
In The Cancer Genome Atlas breast cancer study, which performed exome sequencing of tumor and normal samples from a selected cohort of breast cancer patients, a 1/3 somatic to 2/3 germline ratio was found [
87] and a similar ratio of somatic to germline mutations has been found in other studies [
88].
In a large-scale study in the United States, Vidula et al. analyzed cDNA by NGS and demonstrated that this approach can identify three classes of clinically relevant BRCA1/2 mutations: germline mutations, somatic loss of function, and reversions. This study supports the notion that systematic analysis of cfDNA in patients with advanced cancer can help identify potential candidates for appropriate genotype-based therapy [
74].
In line with this, another study conducted in 2017 to analyze cfDNA by massively parallel sequencing, this study targeted all exons of 141 genes and all exons and introns of
BRCA1 and
BRCA2, as well as functional studies to assess the impact of putative
BRCA1/2 reversion mutations on
BRCA1/2 function, the findings of this study support the utility of cfDNA sequencing to identify putative
BRCA1/2 reversion mutations and facilitate patient selection for PARP inhibition therapy [
75].
3. ESR1 Gene
Over 75% of primary breast cancers are ER-positive, for which hormone therapy is the gold standard in the treatment armamentarium [
58,
89]. The estrogen receptor (ER) is a transcription factor involved in cell proliferation and activation [
90]. Estrogen receptor alpha is encoded by the
ESR1 gene. The acquisition of alterations in this gene has been identified as an important resistance mechanism to endocrine therapy [
91].
ESR1 mutations rarely occur in primary tumors (~1%) but are relatively common (10–50%) in metastatic cancers presenting resistance to endocrine therapy, this is explained by the therapeutic pressure that stimulates the emergence of activating mutations of
ESR1 in the metastatic tissue. These gene mutations are associated with shorter progression-free survival [
90]. Therefore, it is important to test for
ESR1 somatic mutations in ctDNA in order to detect the onset of this molecular resistance even before clinical progression. To predict treatment outcomes, because this may dictate patient management, including monitoring and modifications of the treatment plan, eventually this approach can be used to guide sequential treatment options in patients [
68,
71]. The potential value of screening for
ESR1 mutations in metastatic cancer has increased.
In a Japanese study in 2017, involving 86 ER+ breast cancer patients, including 69 patients diagnosed with metastatic breast cancer (MBC) and 17 patients with primary breast cancer (PBC), the results showed the absence of
ESR1 mutations in the PBC group, whereas in the MBC group
ESR1 cfDNA mutations were detected in 28.9%. The clinical impact of these mutations was significantly important: all
ESR1 mutation-positive patients had resistance to previous treatments with aromatase inhibitors (AIs) compared to 71.4% of
ESR1 WT patients; 85% of ESR1 mutation-positive patients had resistance to previous treatment with selective estrogen receptor modulators (SERMs) compared to 51% of
ESR1 WT patients. Otherwise, cfDNA monitoring in a subgroup of 52 patients showed that loss of
ESR1 mutations was associated with a longer response time [
73].
In January 2020, a Chinese comparative study was conducted comparing 297 tumor samples of primary breast cancer patients and 43 blood samples of metastatic breast cancer (MBC) patients. Next-generation sequencing (NGS) was used by targeting the whole exon of the
ESR1 gene, and the result’s findings are consistent with previous studies:
ESR1 mutations were more frequently detected in circulating tumor DNA of MBC patients than in PBC patients, and the
ESR1 mutation frequency in patients using aromatase inhibitors (AIs) was significantly higher than those who were not using AIs [
92].
A French large study targeting twelve genes by whole exome sequencing has identified
ESR1 as a pilot gene specific to MBC, they confirmed that the
ESR1 gene mutation is the most frequent “metastasis-specific” mutation observed in MBC, by identifying that 100% of
ESR1 mutation-positive cases are ER + and present resistance to endocrine therapy [
93]. In 2020, a confirmative study by Shibayama and Al reported that
ESR1 mutations were found to be a prognostic predictor of acquired resistance to endocrine therapy [
94].
Collectively, these studies demonstrate how the genetic profile of MBC is different from that of primary breast tumors. Hence, metastatic cancer profiling must become a primary step in the definition of optimal treatments for patients; thus, monitoring and surveillance studies will be critical to confirm the effectiveness after treatment. A final point regarding these findings was how easily and feasibly this biomarker could be obtained, plasma samples can be easily collected for ctDNA analysis, allowing for dynamic testing that will increase our understanding of the disease progression and the design of strategies to improve outcomes.
4. PIK3CA Gene
The
PIK3CA gene encodes the A isoform of the catalytic subunit (p110a) of the phosphatidylinositol 3-kinases class IA. Phosphatidylinositol 3-kinases (PI3K) are involved in the conversion of phosphatidylinositol 4,5-biphosphate (PIP2) to phosphatidylinositol 3,4,5-triphosphate (PIP3). This PI3K class has a critical role in the control of various cellular processes such as cell growth and proliferation, metabolism, and migration via the PI3K/AKT/mTOR pathway [
95].
In approximately 40% of HR + breast cancer cases, the most common molecular alterations are the activating mutations of the PI3K subunit in the
PIK3CA gene, these mutations induce hyperactivation of the p110α catalytic subunit, leading to constitutive phosphorylation of the AKT and its forward effectors [
96,
97].
Several preclinical studies indicate that the PIK3/AKT/mTOR pathway alterations may correlate with resistance to CDK4/6 inhibitors (CDK4/6i). Cyclin-dependent kinase 4 and 6 (CDK4/6i) inhibitors have shown clinical efficacy in ER-positive MBC, although their cytostatic effects are limited by primary and acquired resistance, putative mechanisms of resistance to CDK4/6i have been identified [
76,
98].
An Italian study completed in January 2021 showed that patients with a
PIK3CA mutation in the blood at the start of CDK4/6i treatment had a significantly shorter Progression Free Survival (PFS) compared to patients without a mutation. Therefore, PI3K status should be considered as a potential predictive biomarker of CDK4/6i resistance. The integration of PI3K status assessment with other molecular information in a surveillance system can improve the accuracy of predicting Overall Survival (OS) and PFS of patients with metastatic breast cancer and may suggest the best treatment strategy. On the other hand, it should be noted that PI3K status as such cannot be the only responsible for CDK4/6i resistance, and thus, special attention should be given to all mutations that also promote the activation of the PI3K/AKT/mTOR signaling pathway [
76].
In the same sense, targeted therapy drugs in the final phase of clinical trials, specifically targeting PI3K, are designed to be administered to patients whose tumor has a PIK3CA gene alteration, which makes their detection particularly important in tumor genetics.
5. TP53 Gene
Tumor suppressor
TP53 is considered the genome gatekeeper. Several studies indicate that
TP53 mutations increase the risk of cancer and, once cancer occurs, these mutations promote invasion, metastasis, and chemoresistance [
103]. In invasive breast cancer,
TP53 (p. 53) is the most frequently mutated gene, which is mutated in approximately 80% of triple-negative breast cancer (TNBC) [
104].
The presence or absence of
TP53 mutations is routinely investigated in clinical practice on tumor tissues, using immunohistochemistry or sequencing techniques. However, these methods have various limitations, such as invasiveness and inability to identify tumor heterogeneity and progression, which underline the need for a more robust and sophisticated technology [
105]. Currently,
TP53 gene mutations can be detected by cfDNA analysis given the ability of this biomarker to detect tumor heterogeneity, which is a limitation of tumor biopsies [
106,
107].
In 2017, a French study was realized including 47 patients with non-metastatic triple-negative breast cancer (TNBC) treated with neoadjuvant chemotherapy (NCT), and the study targeted the
TP53 gene at several time points: before NCT; after 1 cycle; before surgery, and after surgery. The results indicated a decrease in ctDNA levels during NCT; however, a small decrease in ctDNA levels during NCT was significantly associated with shorter survival. This research confirmed that the high prevalence of
TP53 mutations in TNBC is a potential biomarker for ctDNA monitoring during NCT, and that ctDNA may become a clinically useful prognostic tool for managing TNBC patients treated with NCT [
77].
In July 2019, Savli and colleagues showed that variations in the
TP53 gene are strongly observed in breast cancer samples, this study demonstrated that
TP53 pathogenic variants detection and monitoring by ctDNA analysis is recommended as a useful biomarker for predictive studies, for tumor growth monitoring and personalized treatment strategy planning [
78].
Screening for
TP53 mutations in ctDNA can provide monitoring for early detection of genetic events underlying drug resistance and can also inform therapy approaches [
79], FEI MA et al.,
(ClinicalTrials.gov NCT01937689) have exploited ctDNA profiling before and after treatment with an oral anti-HER1/HER2 tyrosine kinase inhibitor for 18 HER2-positive metastatic breast cancer patients, and they identified that mutations in
TP53 and PI3K/Akt/mTOR pathway genes were strongly implicated in resistance to HER1/HER2 blocking [
108].
The overall clinical trials confirm that p53 is both a potential prognostic and predictive biomarker and a therapeutic target for breast cancer patients, particularly for TN subtype patients.
6. ERBB2 Gene
The human epidermal growth factor receptor 2 (
HER2) is overexpressed in 20–30% of breast cancer patients [
109], this amplification is “acquired” in approximately 2–5% of metastatic breast cancers that originally had primary cancers that were not HER2 amplified [
110]. Blocking HER2 activity through trastuzumab provides a better outcome for HER2-positive patients. However, resistance in women with metastatic breast cancer (MBC) is usually observed [
111].
As targeted anti-HER2 therapies are developed, the assessment of
HER2 status will be more important to stratify patients to the most appropriate treatment regimens [
110], and this requires repetitive tumor sampling to identify whether the cancer’s genetic profile has changed after previous treatment [
112]. The analysis of circulating DNA has the potential to screen for
HER2 (ERBB2) amplification acquisition in a non-invasive manner.
In 2017, a phase II study
(Clinicaltrials.gov, NCT01670877) was conducted to evaluate the clinical benefit rate (CBR) of NERATINIB as monotherapy through determining
HER2 mutations based on circulating DNA analysis, whereby the results indicated the efficacy of NERATINIB in HER2 mutated non-amplified breast cancer and justify that cfDNA sequencing may offer a non-invasive strategy to identify patients with HER2 mutated cancers [
80]. In a similar direction, and at a larger scale, a multicenter, open-label, multicohort, phase 2a clinical trial
(ClinicalTrials.gov, NCT03182634) in 18 UK hospitals was conducted, the results confirm the clinically relevant activity of targeted therapies against rare activating mutations in breast cancer, in HER2 mutant breast cancer
(ERBB2) identified by cfDNA tests, NERATINIB had comparable activity to that observed when guided by tissue tests [
81].
In October 2020, Kleftogiannis et al. developed a new error-correcting cfDNA sequencing approach using bioinformatics strategies to identify tumor-associated genomic alterations. This assay was also performed effectively on the detection of copy number variations (CNVs) in the
ERBB2 oncogene. This result creates opportunities for better tumor characterization, in which sequential plasma samples can be collected to represent CNVs and variants more precisely over time [
113].
This entry is adapted from the peer-reviewed paper 10.3390/diagnostics13030470