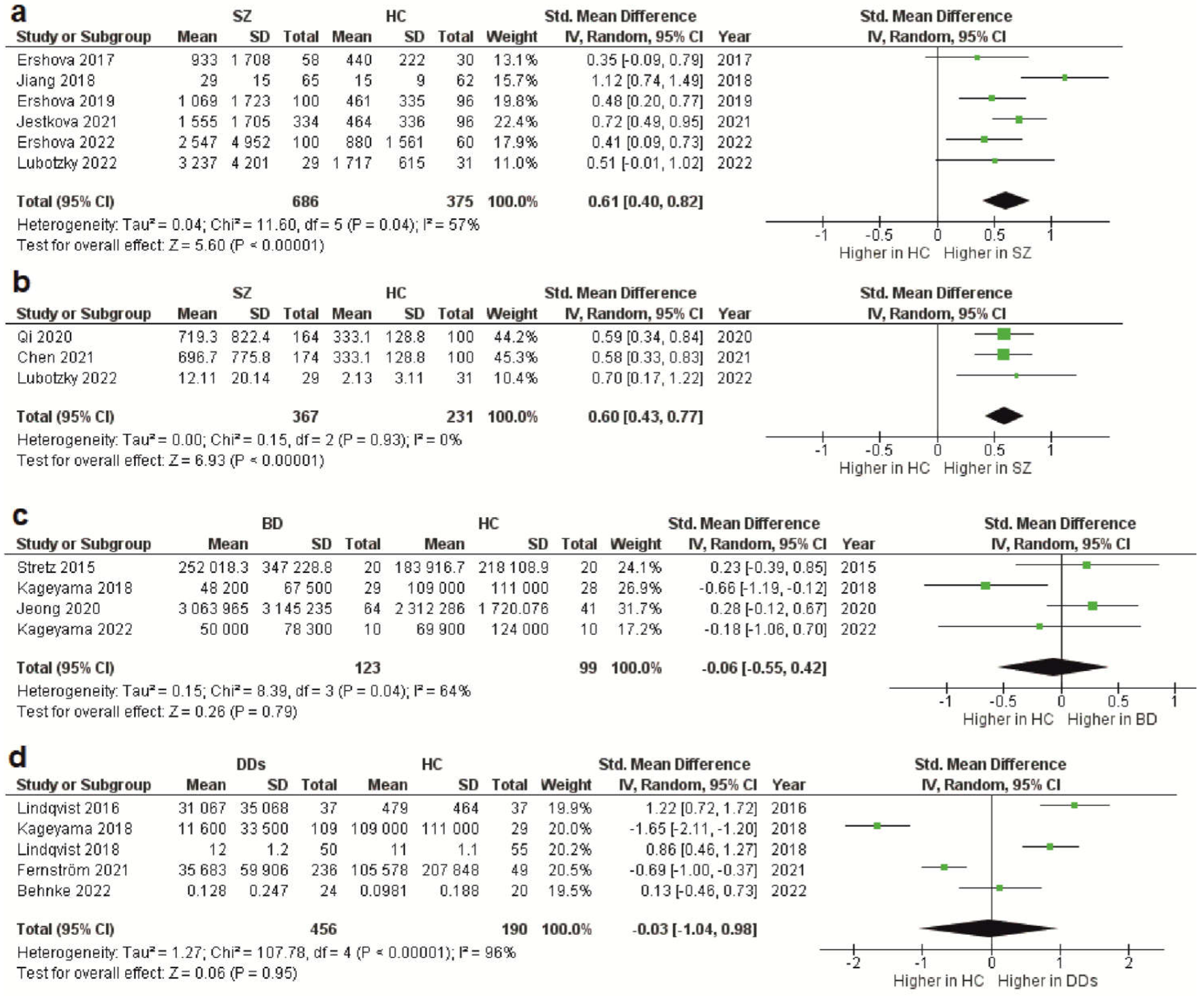
The cell-free DNA (cfDNA) levels are known to increase in biological fluids in various pathological conditions. However, the data on circulating cfDNA in severe psychiatric disorders, including schizophrenia, bipolar disorder (BD), and depressive disorders (DDs), is contradictory. The meta-analysis showed that the levels of total cfDNA and genomic cfDNA in patients with schizophrenia are significantly higher than in healthy donors (SMD values of 0.61 and 0.6, respectively; p < 0.00001). Data on mitochondrial cfDNA in schizophrenia were scarce. Meta-analysis in BD and DDs found no significant differences in the level of mitochondrial cfDNA. However, further research on mitochondrial and genomic cfDNA levels in psychiatric disorders is needed due to the data heterogeneity.
- cfDNA
- cf-mtDNA
- DAMPs
- schizophrenia
- bipolar disorder
- major depressive disorder
1. Introduction
2. Reports Characteristics
| Study | Year | DNA Type | Sample | Extraction Method | Detection Method | Population |
|---|---|---|---|---|---|---|
| Schizophrenia | ||||||
| Ershova et al. [22] | 2017 | Total CfDNA | Plasma | Solvent extraction method | FL, PicoGreen dye | SZ 58/HC 30 |
| Jiang et al. [21] | 2018 | Total CfDNA | Plasma | TIANamp Micro DNA Kit (spin-column) | FCS | SZ 65/HC 62 |
| Ershova et al. [20] | 2019 | Total CfDNA | Plasma | Solvent extraction method | FL, PicoGreen dye | SZ 100/HC 96 |
| Jestkova et al. [23] | 2021 | Total CfDNA | Plasma | Solvent extraction method | FL, PicoGreen dye | SZ 334/HC 95 |
| Ershova et al. [24] | 2022 | Total CfDNA | Plasma | Solvent extraction method | FL, PicoGreen dye | SZ 100/HC 60 |
| Lubotzky et al. [25] | 2022 | Total CfDNA and Cf-gDNA | Plasma | QIAsymphony DSP Circulating DNA Kit (magnetic particles) | FL, bisulfite DNA treatment, PCR amplification followed by NGS | FEP 29/HC 31 |
| Chen et al. [26] | 2021 | Cf-gDNA | Serum | TianLong DNA Kit (spin-column) | qPCR, target: Alu repeats | SZ 174/HC 100 |
| Qi et al. [27] | 2020 | Cf-gDNA | Serum | TianLong DNA Kit (spin-column) | qPCR, target: Alu repeats | SZ 164/HC 100 |
| Bipolar Disorder | ||||||
| Stertz et al. [30] | 2015 | Cf-mtDNA | Serum | QIAmp DNA Mini Kit (spin-column) | qPCR, target: MT-ATP8 gene | BD 20/HC 20 |
| Kageyama et al. [29] | 2018 | Cf-mtDNA | Plasma | QIAamp DNA Blood Mini Kit (spin-column) | qPCR, target: MT-ND1 and MT-ND4 genes | BD 28/HC 29 |
| Jeong et al. [31] | 2020 | Cf-mtDNA | Serum | QIAmp DNA Mini Kit (spin-column) | qPCR, target: MT-ND1 gene | BD 64/HC 41 |
| Kageyama et al. [32] | 2022 | Cf-mtDNA | Plasma | QIAamp DNA Blood Mini Kit (spin-column) | qPCR, target: MT-ND1 and MT-ND4 genes | BD 10/HC 10 |
| Depressive disorders | ||||||
| Lindqvist et al. [33] | 2016 | Cf-mtDNA | Plasma | QIAmp 96 DNA Blood Kit (spin-column) | qPCR, target: MT-ND2 gene | Suicide attempters 37/HC 37 |
| Kageyama et al. [29] | 2018 | Cf-mtDNA | Plasma | QIAamp DNA Blood Mini Kit (spin-column) | qPCR, target: MT-ND1 and MT-ND4 genes | MDD 109/HC 29 |
| Lindqvist et al. [34] | 2018 | Cf-mtDNA | Plasma | QIAmp 96 DNA Blood Kit (spin-column) | qPCR, target: MT-ND1 and MT-ND4 genes | MDD 50/HC 55 |
| Fernström et al. [35] | 2021 | Cf-mtDNA | Plasma | QIAmp DNA Blood Mini Kit (spin-column) | qPCR, target: MT-ND2 gene | Current depression 236/HC 49 |
| Behnke et al. [36] | 2022 | Cf-mtDNA | Serum | QIAamp DNA Micro Kit (spin-column) | qPCR with multiple target | MDD 24/HC 20 |
3. CfDNA Level in Schizophrenia
4. CfDNA Level in Bipolar Disorder
5. CfDNA Level in Depressive Disorders
6. Conclusion
This entry is adapted from the peer-reviewed paper 10.3390/ijms24043402
References
- Aucamp, J.; Abel, J.B.; Christoffel, P.S.B. The diverse origins of circulating cell-free DNA in the human body: A critical re-evaluation of the literature. Biol. Rev. Camb. Philos. Soc. 2018, 93, 1649–1683.
- Labbe, M.; Petresco, M.; Fabrykant, M.L. Taux du phosphore sanguin et de ses differentes formes dans les leucemies et les anemies. J. Soc. Biol. 1931, 107, T2.
- Mandel, P.; Metais, P. Nuclear acids in human blood plasma. Comptes Rendus Seances Soc. Biol. Fil. 1948, 142, 241–243.
- Bronkhorst, A.J.; Ungerer, V.; Diehl, F.; Anker, P.; Dor, Y.; Fleischhacker, M.; Gahan, P.B.; Hui, L.; Holdenrieder, S.; Thierry, A.R. Towards systematic nomenclature for cell-free DNA. Hum. Genet. 2021, 140, 565–578.
- Pös, O.; Biró, O.; Szemes, T.; Nagy, B. Circulating cell-free nucleic acids: Characteristics and applications. Eur. J. Hum. Genet. 2018, 26, 937–945.
- Grabuschnig, S.; Bronkhorst, A.J.; Holdenrieder, S.; Rosales, R.I.; Schliep, K.P.; Schwendenwein, D.; Ungerer, V.; Sensen, C.W. Putative origins of cell-free DNA in humans: A review of active and passive nucleic acid release mechanisms. Int. J. Mol. Sci. 2020, 21, 8062.
- Fernando, M.R.; Jiang, C.; Krzyzanowski, G.D.; Ryan, W.L. New evidence that a large proportion of human blood plasma cell-free DNA is localized in exosomes. PLoS ONE 2017, 12, e0183915.
- Heitzer, E.; Auinger, L.; Speicher, M.R. Cell-free DNA and apoptosis: How dead cells inform about the living. Trends Mol. Med. 2020, 26, 519–528.
- Yipp, B.G.; Kubes, P. NETosis: How vital is it? Blood 2013, 122, 2784–2794.
- Moss, J.; Magenheim, J.; Neiman, D.; Zemmour, H.; Loyfer, N.; Korach, A.; Samet, Y.; Maoz, M.; Druid, H.; Arner, P.; et al. Comprehensive human cell-type methylation atlas reveals origins of circulating cell-free DNA in health and disease. Nat. Commun. 2018, 9, 5068.
- Lo, Y.M.D.; Han, D.S.C.; Jiang, P.; Chiu, R.W.K. Epigenetics, fragmentomics, and topology of cell-free DNA in liquid biopsies. Science 2021, 372, eaaw3616.
- Van der Meij, K.R.M.; Sistermans, E.A.; Macville, M.V.E.; Stevens, S.J.C.; Bax, C.J.; Bekker, M.N.; Bilardo, C.M.; Boon, E.M.J.; Boter, M.; Diderich, K.E.M.; et al. TRIDENT-2: National implementation of genome-wide non-invasive prenatal testing as a first-tier screening test in the Netherlands. Am. J. Hum. Genet. 2019, 105, 1091–1101.
- Fettke, H.; Kwan, E.M.; Azad, A.A. Cell-free DNA in cancer: Current insights. Cell. Oncol. (Dordr.) 2019, 42, 13–28.
- De Vlaminck, I.; Valantine, H.A.; Snyder, T.M.; Strehl, C.; Cohen, G.; Luikart, H.; Neff, N.F.; Okamoto, J.; Bernstein, D.; Weisshaar, D.; et al. Circulating cell-free DNA enables noninvasive diagnosis of heart transplant rejection. Sci. Transl. Med. 2014, 6, 241ra77.
- Zindel, J.; Kubes, P. DAMPs, PAMPs, and LAMPs in immunity and sterile inflammation. Annu. Rev. Pathol. 2019, 15, 493–518.
- Gong, T.; Liu, L.; Jiang, W.; Zhou, R. DAMP-sensing receptors in sterile inflammation and inflammatory diseases. Nat. Rev. Immunol. 2020, 20, 95–112.
- Ermakov, E.A.; Melamud, M.M.; Buneva, V.N.; Ivanova, S.A. Immune System Abnormalities in Schizophrenia: An Integrative View and Translational Perspectives. Front. Psychiatry 2022, 13, 880568.
- Pereira, A.C.; Oliveira, J.; Silva, S.; Madeira, N.; Pereira, C.M.F.; Cruz, M.T. Inflammation in Bipolar Disorder (BD): Identification of new therapeutic targets. Pharmacol. Res. 2021, 163, 105325.
- Miller, A.H.; Raison, C.L. The role of inflammation in depression: From evolutionary imperative to modern treatment target. Nat. Rev. Immunol. 2016, 16, 22–34.
- Ershova, E.S.; Jestkova, E.M.; Martynov, A.V.; Shmarina, G.V.; Umriukhin, P.E.; Bravve, L.V.; Zakharova, N.V.; Kostyuk, G.P.; Saveliev, D.V.; Orlova, M.D.; et al. Accumulation of circulating cell-free CpG-enriched ribosomal DNA fragments on the background of high endonuclease activity of blood plasma in schizophrenic patients. Int. J. Genom. 2019, 2019, 8390585.
- Jiang, J.; Chen, X.; Sun, L.; Qing, Y.; Yang, X.; Hu, X.; Yang, C.; Xu, T.; Wang, J.; Wang, P.; et al. Analysis of the concentrations and size distributions of cell-free DNA in schizophrenia using fluorescence correlation spectroscopy. Transl. Psychiatry 2018, 8, 104.
- Ershova, E.S.; Jestkova, E.M.; Chestkov, I.V.; Porokhovnik, L.N.; Izevskaya, V.L.; Kutsev, S.I.; Veiko, N.N.; Shmarina, G.; Dolgikh, O.; Kostyuk, S.V. Quantification of cell-free DNA in blood plasma and DNA damage degree in lymphocytes to evaluate dysregulation of apoptosis in schizophrenia patients. J. Psychiatr. Res. 2017, 87, 15–22.
- Jestkova, E.M.; Ershova, E.S.; Martynov, A.V.; Zakharova, N.V.; Kostyuk, G.P.; Veiko, N.N.; Kostyuk, S.V. Concentration of Circulating Cell-Free DNA in the Peripheral Blood Plasma of Patients with Acute Endogenous and Exogenous Etiology Psychoses. Psikhiatria 2021, 19, 6–14.
- Ershova, E.S.; Shmarina, G.V.; Martynov, A.V.; Zakharova, N.V.; Veiko, R.V.; Umriukhin, P.E.; Kostyuk, G.P.; Kutsev, S.I.; Veiko, N.N.; Kostyuk, S.V. NADPH-oxidase 4 gene over-expression in peripheral blood lymphocytes of the schizophrenia patients. PLoS ONE 2022, 17, e0269130.
- Lubotzky, A.; Pelov, I.; Teplitz, R.; Neiman, D.; Smadja, A.; Zemmour, H.; Piyanzin, S.; Ochana, B.L.; Spalding, K.L.; Glaser, B.; et al. Elevated brain-derived cell-free DNA among patients with first psychotic episode—A proof-of-concept study. Elife 2022, 11, e76391.
- Chen, L.Y.; Qi, J.; Xu, H.L.; Lin, X.Y.; Sun, Y.J.; Ju, S.Q. The Value of Serum Cell-Free DNA Levels in Patients with Schizophrenia. Front. Psychiatry 2021, 12, 637789.
- Qi, J.; Chen, L.Y.; Shen, X.J.; Ju, S.Q. Analytical Value of Cell-Free DNA Based on Alu in Psychiatric Disorders. Front. Psychiatry 2020, 10, 992.
- Ouyang, H.; Huang, M.; Xu, Y.; Yao, Q.; Wu, X.; Zhou, D. Reduced Cell-Free Mitochondrial DNA Levels Were Induced by Antipsychotics Treatment in First-Episode Patients with Schizophrenia. Front. Psychiatry 2021, 12, 652314.
- Kageyama, Y.; Kasahara, T.; Kato, M.; Sakai, S.; Deguchi, Y.; Tani, M.; Kuroda, K.; Hattori, K.; Yoshida, S.; Goto, Y.; et al. The relationship between circulating mitochondrial DNA and inflammatory cytokines in patients with major depression. J. Affect. Disord. 2018, 233, 15–20.
- Stertz, L.; Fries, G.R.; Rosa, A.R.; Kauer-Sant’anna, M.; Ferrari, P.; Paz, A.V.; Green, C.; Cunha, Â.B.; Dal-Pizzol, F.; Gottfried, C.; et al. Damage-associated molecular patterns and immune activation in bipolar disorder. Acta Psychiatr. Scand. 2015, 132, 211–217.
- Jeong, H.; Dimick, M.K.; Sultan, A.; Duong, A.; Park, S.S.; El Soufi El Sabbagh, D.; Goldstein, B.I.; Andreazza, A.C. Peripheral biomarkers of mitochondrial dysfunction in adolescents with bipolar disorder. J. Psychiatr. Res. 2020, 123, 187–193.
- Kageyama, Y.; Deguchi, Y.; Kasahara, T.; Tani, M.; Kuroda, K.; Inoue, K.; Kato, T. Intra-individual state-dependent comparison of plasma mitochondrial DNA copy number and IL-6 levels in patients with bipolar disorder. J. Affect. Disord. 2022, 299, 644–651.
- Lindqvist, D.; Fernström, J.; Grudet, C.; Ljunggren, L.; Träskman-Bendz, L.; Ohlsson, L.; Westrin, Å. Increased plasma levels of circulating cell-free mitochondrial DNA in suicide attempters: Associations with HPA-axis hyperactivity. Transl. Psychiatry 2016, 6, e971.
- Lindqvist, D.; Wolkowitz, O.M.; Picard, M.; Ohlsson, L.; Bersani, F.S.; Fernström, J.; Westrin, Å.; Hough, C.M.; Lin, J.; Reus, V.I.; et al. Circulating cell-free mitochondrial DNA, but not leukocyte mitochondrial DNA copy number, is elevated in major depressive disorder. Neuropsychopharmacology 2018, 43, 1557–1564.
- Fernström, J.; Ohlsson, L.; Asp, M.; Lavant, E.; Holck, A.; Grudet, C.; Westrin, Å.; Lindqvist, D. Plasma circulating cell-free mitochondrial DNA in depressive disorders. PloS ONE 2021, 16, e0259591.
- Behnke, A.; Gumpp, A.M.; Rojas, R.; Sänger, T.; Lutz-Bonengel, S.; Moser, D.; Schelling, G.; Krumbholz, A.; Kolassa, I.T. Circulating inflammatory markers, cell-free mitochondrial DNA, cortisol, endocannabinoids, and N-acylethanolamines in female depressed outpatients. World J. Biol. Psychiatry 2023, 24, 58–69.
- Meddeb, R.; Pisareva, E.; Thierry, A.R. Guidelines for the preanalytical conditions for analyzing circulating cell-free DNA. Clin. Chem. 2019, 65, 623–633.