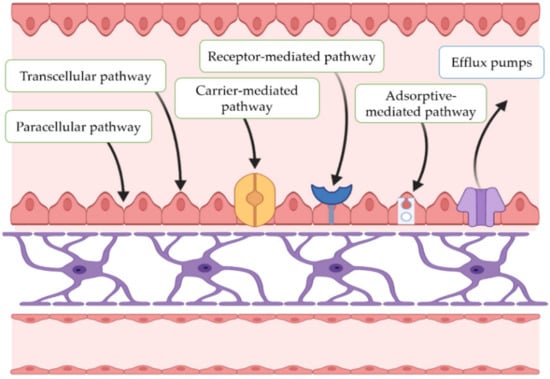
Today, levodopa-based therapies continue to be the standard care for PD, as they are effective in treating the disease’s motor symptoms and tend to be of relatively low cost. However, although these medications offer valuable symptomatic relief, as neurodegeneration advances, their use is often associated with significant and sometimes intolerable side effects. In addition to new therapeutic options, there is a need for improved efficiency of the existing ones, as many agents have difficulties in crossing the blood–brain barrier (BBB) to achieve therapeutic levels in the CNS or exhibit inappropriate pharmacokinetic profiles, thereby limiting their clinical benefits (Figure 2).
2. Investigational Polymeric Microparticles for the Treatment of Parkinson’s Disease
In recent years, different multiparticulate systems, such as polymeric MPs, have been designed as potential therapeutic approaches for PD. MPs are structures with sizes ranging from 1 to 1000 µm [
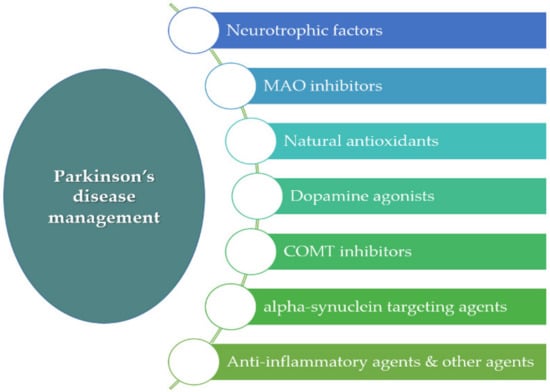
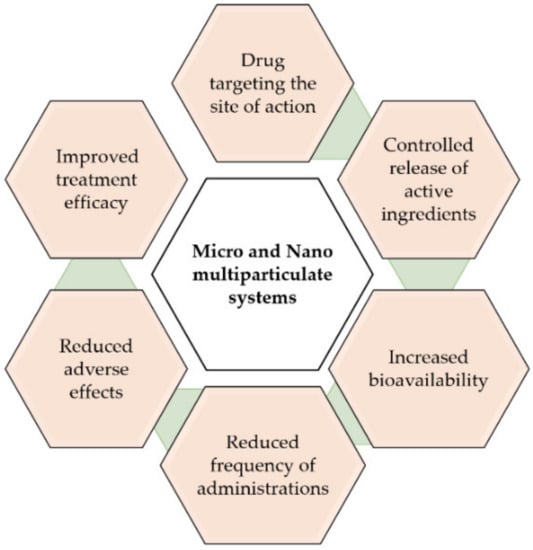
26]. Among the advantages of MPs is the possibility of achieving the controlled release of the active ingredients at the target site. This is of great interest for drugs that have limited access to the CNS. In addition, reduced adverse systemic effects and less frequent dosing intervals can be also achieved by MPs. Under investigation are different antiparkinsonian agents encapsulated within polymeric MPs, including neurotrophic factors such as glial-cell-derived neurotrophic factor (GDNF) and vascular endothelial growth factor (VEGF), antioxidant agents, inhibitors of different enzymes such as monoamine oxidase (MAO) and catechol-O-methyltransferase (COMT), anti-inflammatory compounds, as well as α-synuclein-targeting agents.
2.1. Neurotrophic Factors
Neurotrophic factors (NTFs) are biological molecules that influence several neuronal functions, including cell survival and axonal growth [
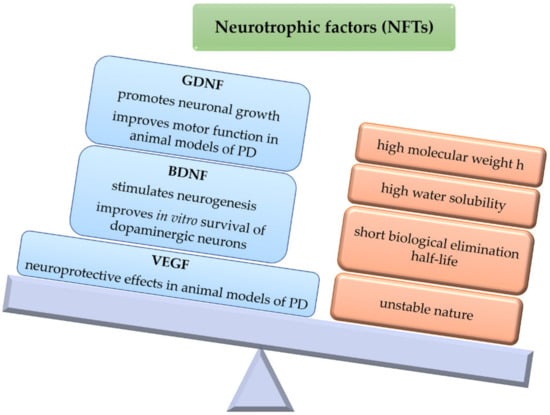
27]. For instance, GDNF has demonstrated to be able to protect and promote neuronal growth, also improving motor functions in animal models of PD [
27]. However, as the BBB is a major entry restriction, its high molecular weight and water solubility hinders the access of GDNF to the brain parenchyma. Thus, one viable route of administration is by means of viral vectors integrating the GDNF gene, or by implanting cells, semipermeable structures, or grafts that secrete the neurotrophic factor [
28]. In addition, GDNF exhibits a short biological elimination half-life due to its unstable nature. For these reasons, encapsulating this neurotrophic factor within polymeric microparticulate systems may be an interesting approach for brain delivery, as these systems can protect GDNF against external factors, also providing sustained release [
29].
The use of GDNF has been Investigated in combination with cell transplants, although this strategy does not lead to direct cell growth, which is necessary for full functional recovery. Furthermore, GDNF must be released transiently at low doses rather than in a constant manner over several months, since continuous release may affect synaptic integration of the transplanted and host tissues. Therefore, given the complex mechanism associated with PD, an interesting strategy may be the design of devices able to release GDNF in the nigral region to improve immediate transplant survival, and in addition, possibly release another factor, such as BDNF, to stimulate neurite outgrowth in the striatal region [
30].
Brain-derived neurotrophic factor (BDNF) stimulates and controls growth of new neurons from neural stem cells (neurogenesis) [
31,
32,
33]. In vitro studies have also provided evidence that BDNF can improve DA production, axonal extension, and survival in cultured dopaminergic neurons [
34]. Abnormally low levels of this factor have been associated with neurodegenerative diseases such as PD [
35]. BDNF could be used to reduce neurodegeneration and enhance the success of cell transplants required for long-term therapy and potential reversal of disease by promoting reinnervation [
36]. However, clinical efficacy has been severely limited by its limited access to the CNS [
28].
In human traumatic brain injury (TBI), day-of-injury serum BDNF has been associated with TBI diagnosis also providing 6-month prognostic information regarding recovery from the injury [
37].
Vascular endothelial growth factor (VEGF) is an angiogenic factor with specificity for endothelial cells that has demonstrated neuroprotective effects in animal models of PD [
38]. However, the use of VEGF as a neuroprotective factor is complicated, as its effect is dose-dependent, with high levels of VEGF inducing brain edema [
39]. As with other NFs, clinical use is limited by its rapid degradation and difficulty in crossing the BBB [
40]. To obtain a continuous and direct release of VEGF to the CNS, different intracranial administration strategies, such as MP administration, have been tested in animal models of PD [
41] (
Figure 4).
Figure 4. Neurotrophic factors. Potential mechanisms of action in Parkinson’s disease (PD). Physicochemical and biological characteristics. GDNF (Glial-Cell-Derived Neurotrophic Factor), BDNF (Brain-Derived Neurotrophic Factor), VEGF (Vascular Endothelial Growth Factor).
Therefore, NFs (GDNF, BDNF, VEGF) are of interest as potential therapeutic strategies for PD. Different polymeric systems have been developed that include GDNF or VEGF alone [
40,
42], GDNF and BDNF together [
43], or VEGF [
40].
For instance, Gujral et al. [
44] developed polymeric PLGA/collagen MPs by a water-in-oil-in-water (W/O/W) double emulsion method in which GDNF was fused with collagen-binding peptide (CBP) and immobilized to the inner collagen phase. The controlled release of GDNF-CBP was obtained when compared with standard MPs, with the system being non-cytotoxic up to concentrations of 300 μg/2 × 10
5 cells in neural stem/progenitor cells (NSPCs). In addition, culture of MPs with NSPCs cells induced differentiation into mature neurons, with the bioactivity of released GDNF being like that of recombinant human GDFN (rhGDNF). For this, GDNF-CBP MPs could be useful for the management of PD and other neurodegenerative diseases.
Jollivet et al. [
42] prepared GDNF MPs that released in vivo the neurotrophic factor for 2 months. rhGDNF-loaded MPs were elaborated using PLGA as a biodegradable polymer and were implanted into the brains of parkinsonian rats treated with 6-hydroxydopamine (6-OHDA) to induce a partial progressive and retrograde lesion of the nigrostriatal system. In this study, the MPs were well tolerated and induced sprouting of the preserved dopaminergic fibers with synaptogenesis. Other authors [
45] have also demonstrated that GDNF-releasing MPs were able to protect dopaminergic neurons for 6 weeks when concomitantly injected with 6-OHDA by stereotaxic procedure.
Garbayo et al. [
46] prepared N-glycosylated recombinant GDNF-loaded PLGA MPs. This delivery system was tested in an animal model of PD in which a unilateral lesion was induced in the nigrostriatal area by stereotaxic administration of 6-OHDA every 2 weeks. The amphetamine-induced rotational asymmetry test was conducted in the animals. The formulation developed was able to release the active ingredient for 5 weeks, improving the rotational behavior induced by amphetamine in the animals treated with GDNF as well as increasing the density of TH-positive fibers at the striatal level, without causing toxicity. The same authors [
47] also prepared GDNF-loaded PLGA MPs, which were evaluated in macaques (
Macaca fascicularis) after inducing PD-like symptoms with 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP). The MPTP model has some advantages over 6-OHDA as it does not require stereotaxic surgery for its administration [
48,
49]. The MPs were administered unilaterally into the putamen of parkinsonian monkeys with severe nigrostriatal degeneration. After 9 months, administration of microencapsulated GDNF (single dose, 25 mg of GDNF) led to sustained GDNF levels in the brain, resulting in motor enhancement and restoration of dopaminergic function. This was reflected by a bilateral increase in the density of striatal dopaminergic neurons. In addition, GDNF was retrogradely transported to the substantia nigra, bilaterally increasing the number of dopaminergic and total neurons, regardless of the degeneration produced. In addition, the administration of GDNF-loaded PLGA MPs was found to be safe, not causing immunogenicity, cerebellar degeneration, or weight loss. Therefore, the safety and efficacy shown by this new therapeutic system may represent an important basis for the clinical development of GDNF MPs [
47].
Lampe et al. [
43] developed a new delivery system consisting of PLGA MPs entrapped within degradable PEG-based hydrogel devices to locally release GDNF and BDNF with two different release profiles. The authors aimed for locally deliver GDNF or BDNF to brain areas associated with PD. GDNF was included to improve immediate transplant cell survival [
30] and BDNF to stimulate neurite outgrowth in the striatal region. In the experiments carried out in Sprague Dawley rats, stereotaxic implantation of the hydrogels was conducted with the BDNF end oriented to the striatum and the GDNF end to the substantia nigra, using minimally invasive single penetration for implantation. Doses of NTFs encapsulated within each hydrogel were 1 ng for BDNF and 10 ng for GDNF. The device delivered the NTFs in a region localized within 100 µm of the bridge, but not exactly to the targeted rostral or caudal ends. BDNF was slowly delivered over a period of 56 days, while a bolus of GDNF was released at around 28 days. The timed delivery of NTFs from the implanted devices using a multifaceted PEG hydrogel/PLGA microparticle strategy markedly reduced the microglial response relative to sham surgeries, which may constitute an interesting approach for the potential treatment of neurodegenerative diseases, such as PD.
The effect of VEGF, GDNF, and their combination was evaluated by Herrán et al. [
40]. These authors developed PLGA MPs loaded with GDNF and/or VEGF (GDNF-MPs and VEGF-MPs, respectively) which were administered to a 6-OHDA PD model induced in Sprague Dawley rats. Animals treated with at least one of the NTFs showed regenerative improvement in the amphetamine-induced turnover tests with respect to control animals, with the most effective intervention being achieved by GDNF-loaded MPs. In addition, recovery of the neuronal tissue was quantified at the end of the treatment by means of optical densitometry and immunohistochemical tests. Non-statistically significant differences were found, although animals treated with GDNF-loaded MPs or VEGF/GDNF-loaded MPs showed greater recovery in the injured area than those treated with VEGF-MPs or blank MPs. Both GDNF individually and the combination of GDNF and VEGF encapsulated within polymeric MPs exhibited regenerative effects in this experimental model of PD.
MPs prepared with biodegradable and biocompatible polymers represent a potential approach for the delivery of NFTs to the CNS; however, in most of the experiments carried out with NFT-loaded MPs, either the PD animal model assayed was that of 6-OHDA, which involves stereotaxic administration, thereby facilitating penetration of the MPs, or MPs were surgically implanted. As MPs cannot cross the BBB, less invasive administration techniques should be investigated to adequately establish the therapeutic potential of polymeric NFT-loaded MPs in neurodegenerative diseases.
2.2. MAO Inhibitors/Antioxidants
Oxidative stress is a result of various metabolic activities which are essential for life and usually leads to the formation of reactive oxygen species (ROS) and reactive nitrogen species (RNS). It has been associated with the development of PD [
50], as increased oxidative stress has been related to the overexpression of α-syn aggregates [
51].
The mechanisms involved in neuronal degeneration occurring in PD are complex and remain to be fully elucidated, although it is known that the loss of dopaminergic neurons in the substantia nigra pars compacta (SNpc) is responsible for the characteristic motor symptoms present in the disease [
1,
2]. Accumulating evidence suggests that oxidative damage and mitochondrial dysfunction contribute to the cascade of events leading to degeneration of dopaminergic neurons [
52,
53,
54]. This is supported by post-mortem brain analyses showing increased levels of 4-hydroxyl-2-nonenal (HNE), a by-product of lipid peroxidation [
55], the formation of DNA and RNA oxidation products (8-hydroxy-deoxyguanosine and 8-hydroxy-guanosine) [
56,
57], and carbonyl modifications of soluble proteins [
58]. The link between oxidative stress and dopaminergic neuronal degeneration is further supported by modelling the motor aspects of PD in animal models using toxins that cause oxidative stress, including MPTP, rotenone (RT), 6-OHDA, and 1,1′-dimethyl-4,4′-bipyridinium dichloride (paraquat) [
59,
60,
61]. For this reason and given that oxidative imbalance in PD has a multifactorial origin, the use of antioxidant agents could be a viable therapeutic strategy [
62]. In this regard, multiple alternatives have been proposed based on the use of iron chelators, ROS scavengers (vitamins, polyphenols, glutathione, etc.), and other substances (vegetable extracts, melatonin, nicotine, etc.) [
62,
63].
In addition, it seems that MAO-B (monoamine oxidase-B) plays an important role in the production of reactive oxygen intermediates (ROI) in activated astrocytes. MAO-B metabolizes the MPTP toxin to 1-methyl-4-phenylpyridium (MPP+), leading to the production of ROI and eventually to cell death [
64].
Rasagiline (RG) is a therapeutic agent belonging to the group of MAO-B inhibitors (MAOIs) which has demonstrated neuroprotective activity against MPTP and 6-OHDA animal models of PD [
65,
66]. Rasagiline is used for the symptomatic treatment of PD. A recent study conducted in PD patients by Im et al. [
67], when investigating the effects of RG on regional cerebral blood flow (rCBF) by single-photon-emission-computed tomography (SPECT), showed that adjunctive RG therapy has beneficial effects on perfusion in the precuneus of PD patients due to its neuroprotective effects.
The low oral bioavailability of RG (around 36%) and its short elimination half-life (0.6–2 h) [
68] make it a suitable candidate for the design of controlled-release systems. For this, Fernández et al. [
69] developed PLGA MPs loaded with RG mesylate (RM). The efficacy of this system was evaluated in male Wistar rats in an RT-induced model of PD. Daily intraperitoneal (i.p.) administration of RT at a dose of 2 mg/kg/day resulted in neuronal degeneration and behavioral deficits resembling those occurring in PD. Treated animals received the same daily dose of RT for 45 days and RM in saline (1 mg/kg/day) or RM-loaded PLGA MPs, which were assayed at two dose levels: high dose (amount of MPs equivalent to 15 mg/kg RM injected every 15 days) and low dose (amount of MPs equivalent to 7.5 mg/kg RM injected every 15 days). The results demonstrated a robust effect of high-dose RM-loaded MPs on all behavioral tests (catalepsy, akinesia, swim test) which resulted in better outcomes than RM given in solution (1 mg/kg/day). Furthermore, Nissl staining of brain sections showed selective degeneration of the substantia nigra (SN) dopaminergic neurons in animals treated with RT, which was markedly reverted by the administration of high-dose RM-loaded PLGA MPs. Interestingly, PET/CT analysis (positron emission tomography/computed tomography) using 18F-DG (fluorodeoxyglucose F18) resulted in mean increases in the radiotracer in striatum and SN of around 40% when RM-loaded PLGA MPs were given to the animals, thereby indicating the efficacy of the microparticulate drug delivery system developed for RM.
This study continued in 2012 [
70]. In this case, an advanced stage of neurodegeneration was achieved by daily i.p. injections of RT (2 mg/kg). On day 15, animals received RM in saline (1 mg/kg/day) or encapsulated within PLGA microspheres (amount of microspheres equivalent to 15 mg/kg RM given on days 15 and 30). After 45 days RM showed a robust effect on all outcomes evaluated (behavioral tests, Nissl staining, and PCR or Polymerase Chain Reaction), with non-statistically significant differences found between its administration in solution or encapsulated within MPs; however, with the new delivery system, administration of RM could be performed every two weeks instead of daily.
Kanwar et al. [
22] evaluated the efficacy of RM-loaded polycaprolactone (PCL) MPs in Sprague Dawley rats. For the development of PD-like symptoms, stereotaxic infusion of RT (6 μg/2 μL vehicle) was conducted in the animals. After recovery from surgery, animals received RM in solution (1 mg/kg/day), blank PCL MPs, or RM-loaded PCL MPs (equivalent to 30 mg/kg RM given once a month by subcutaneous (s.c.) injection). Significant differences in behavioral tests (locomotor activity, grip strength) and biochemical markers of oxidative stress (lipid peroxidation, reduced glutathione, etc.) were observed between the RM-treated groups and control animals. Non-statistically significant differences were found when RM was given in solution or encapsulated within PCL MPs, but administration of the microparticulate formulation could reduce the need for frequent dosing intervals, thereby resulting in better patient compliance in the treatment of PD.
A few polymeric microparticulate systems have been developed for the encapsulation of MAO-B inhibitors. From the formulation developed, satisfactory results were obtained in animal models of PD, although several issues should be addressed, such as pharmacokinetics and toxicity, as long-term systemic medication commonly leads to deleterious side effects.
2.3. Dopamine Agonists
DA receptor agonists may be able to prevent the nigrostriatal dopaminergic cell loss occurring in PD due to their antioxidant and levodopa-sparing effects. For this, pramipexole [
71,
72,
73], apomorphine [
74], and ropinirole [
75] have been studied in different neurodegenerative animal models, with the outcomes of these studies demonstrating that, in general, these DA agonists are able to prevent the loss of dopaminergic neurons.
Furthermore, recent therapeutical approaches for PD are exploring the use of radical scavenging materials, as polymers as catechol structures have demonstrated antioxidant activities due to their physicochemical properties. In this regard, Newland et al. [
76] synthesized photocrosslinkable DA-containing poly(β-amino ester) (DPAE) from poly(ethylene glycol) diacrylate (PEGDA) and dopamine hydrochloride using Michael-type addition. The authors developed a water-in-oil emulsion technique to photocrosslink the polymer into spherical MPs. The ability of the microparticulate formulation to capture ROS was analyzed by the 2,2-diphenyl-1-picrylhydrazyl (DPPH) method. DPAE MPs at concentrations of 5250 spheres/mL and 7000 spheres/mL reduced the formation of DPPH radicals up to 47 ± 9% and 56 ± 5%, respectively. In contrast, PEG MPs at a concentration of 7000 spheres/mL led to a reduction of only 5 ± 1%. The free radical activity of DPAE MPs increased in a dose-dependent manner up to 56%, with this level of antioxidant activity being slightly higher than that produced by ascorbic acid (10 μM), a well-known antioxidant. Furthermore, tests conducted in dopaminergic SH-SY5Y cells, primary astrocytes, and primary embryonic rat ventral midbrain cultures showed that the concentrations required for radical scavenging were non-toxic, as reduction in metabolic cell activity or morphological alterations did not occur.
Negro et al. [
77] developed ropinirole (RP)-loaded PLGA MPs as a controlled delivery system for this DA agonist. The formulation exhibited sustained in vitro release of the drug (78.23 µg/day/10 mg MPs) for 19 days. The efficacy of the new delivery system was evaluated in an RT model of PD induced in male Wistar rats. For this, animals received daily i.p. doses of RT (2 mg/kg). Once PD-like symptoms appeared (day 15), animals were given either RP in saline (1 mg/kg/day for 45 days) or RP-loaded PLGA MPs at two dose levels (amounts of MPs equivalent to 7.5 mg/kg or 15 mg/kg RP given on days 15 and 30, respectively). Behavioral outcomes (akinesia, catalepsy, rotarod, swim test) and brain analyses (Nissl staining, glial fibrillary acidic protein (GFAP), TH immunohistochemistry) showed that animals receiving RP either in solution or encapsulated within the MPs reverted PD-like symptoms, with the best results obtained with the MPs at the highest dose assayed.
2.4. COMT Inhibitors
Catechol-O-methyltransferase (COMT) is a selective and widely distributed enzyme involved in the catabolism of levodopa, with tolcapone (TC) being a potent COMT inhibitor both in the brain and peripheral tissues, that can slow down levodopa metabolism, thereby leading to a prolongation of its effect in the treatment of PD. Casanova et al. [
78] developed TC-loaded PLGA MPs which exhibited zero-order in vitro release of the drug for 30 days. The new delivery system prepared with 120 mg of TC and 400 mg of PLGA 502 was tested in an RT model of PD induced in male Wistar rats. Daily i.p. injections of the neurotoxin (2 mg/kg) were given to induce neurodegeneration. Once established, animals received TC in saline (3 mg/kg/day) or encapsulated within the MPs (amount of MPs equivalent to 3 mg/kg/day TC every 14 days). Brain analyses of Nissl staining, GFAP, and TH as well as behavioral testing (akinesia, catalepsy, swim test) showed that the new delivery system developed for TC was able to efficiently revert PD-like symptoms in the animal model assayed.
2.5. α-Synuclein-Targeting Agents
Alpha-synuclein (α-syn) is a key protein involved in the pathogenesis of PD. The exact function of α-syn remains still largely unknown, although mounting evidence supports the fact that α-syn is involved in synaptic plasticity and neurotransmitter release [
79,
80]. Under normal conditions, native α-syn exists in a dynamic equilibrium between unfolded monomers and α-helically folded tetramers, with a low tendency for aggregation [
81]. The reduction in the tetramer:monomer ratio and the consequent increase in the level of α-syn unfolded monomers favor its aggregation [
82], which involves a conformational change where the protein adopts a β-sheet-rich structure that facilitates its aggregation into oligomers, protofibrils, and insoluble fibrils that finally accumulate in the form of Lewy bodies [
83]. Lewy bodies are a characteristic feature of PD, being closely related to its progression [
84], as the appearance of Lewy bodies induces alterations in synapses, mitochondrial dysfunction, and deterioration of the endoplasmic reticulum functionality. These circumstances lead to increased metabolic activity, oxidative stress, and protein accumulation, which may explain the subsequent cell death occurring in the disease. Furthermore, misfolded α-syn can spread between different cells and tissues, inducing misfolding of other units of the protein [
83].
The most common α-syn-targeting strategies used in the treatment of PD are decreasing the expression of α-syn with antisense oligonucleotides or miRNA, inhibiting its aggregation with small molecules, favoring its clearance via autophagy, and preventing the seeding and prion-like spreading of α-syn [
81,
85,
86]. In this regard, immunotherapy is gaining increased attention for the management of PD, with active immunization being of particular interest, as it allows for prolonged treatments without the need for frequent dosing intervals [
87]. Immunotherapeutic approaches targeting α-syn have the advantage of addressing several of these mechanisms, with active and passive vaccination being able to prevent neurodegeneration and reduce α-syn accumulation by promoting clearance via autophagy and microglial cells [
88,
89,
90,
91].
The ability of the combined delivery of antigen plus rapamycin (RAP) in the form of nanoparticles in inducing antigen-specific regulatory T cells (Tregs) has been already demonstrated [
92]. Rockenstein et al. [
87] adapted this approach to α-syn by developing an antigen-presenting cell-targeting glucan microparticle (GP) vaccine delivery system. This active immunization system with immunomodulatory activity was composed of GP-MPs loaded with RAP and α-syn as antigen to produce the active humoral immunization (GP+RAP/α-syn). The immunity produced was compared to that of GP-alone, GP-α-syn, and GP+RAP in transgenic (tg) PDGFβ α-syn Line D male and female mice. The effect was analyzed using neuropathological and biochemical markers. Mice treated with GP-RAP and GP-RAP/α-syn showed an increase in the number of Treg lymphocytes in the CNS, decreased levels of proinflammatory cytokines (IL-6 and TNF-α), and increased levels of TGF-β1 (transforming growth factor-beta 1). Animals treated with GP-α-syn and GP-RAP/α-syn presented significant increases in anti-α-syn antibody titers, decreased α-syn aggregates and neurodegeneration, and increased functional recovery markers of neurodegeneration (Arc protein and TH). Therefore, combined therapy (RAP and the antigen) led to better responses than monotherapies, possibly due to the combination of the immunomodulatory activity of RAP and immunization by α-syn. The authors concluded that this new vaccine delivery system, which induced both regulatory Tregs and anti-α-synuclein antibody titers, demonstrated a satisfactory effect in reducing α-syn accumulation, neurodegeneration, and inflammation. Authors claimed that this combined vaccine may be more potent than conventional immunization, which is only based on cellular or humoral immunization, with the potential to be further investigated in synucleinopathies, such as PD and dementia with Lewy bodies, among others.
From the promising results obtained, further research should be conducted to determine if combining humoral and cellular immunization might synergistically reduce inflammation and improve microglial-mediated α-syn clearance.
Table 1 summarizes the polymeric microparticulate systems under investigation as potential new therapeutic approaches for PD.
Table 1. Polymeric microparticulate systems under investigation for the treatment of PD.
| Category |
Active Compound |
Polymer |
Research Model |
Ref. |
| Neurotrophic factors |
GDNF |
PLGA shell/Collagen core |
Cell culture: neural stem/progenitor cells. |
[44] |
| GDNF/BDNF |
PLGA/PEG |
Cell cultures: brain/glial
cells, microglia, and astrocytes.
Animal study: female Sprague Dawley rats. |
[43] |
| GDNF |
PLGA |
Animal study: partial
and progressive 6-OHDA-induced model of PD. Female Sprague Dawley rats. |
[42] |
| GDNF |
PLGA |
Animal study: 6-OHDA-induced model of PD. Female Sprague Dawley rats. |
[46] |
| GDNF |
PLGA |
Animal study: MPTP-induced model of PD. Macaca fascicularis. |
[47] |
| GDNF/VEGF |
PLGA |
Animal study: 6-OHDA-induced model of PD. Female albino Sprague Dawley rats. |
[40] |
MAO
inhibitors/Antioxidants |
Rasagiline |
PLGA |
SKN-AS cell culture, H2O2 neurotoxin.
Animal study: RT-induced model of PD. Male Wistar rats. |
[69] |
| Rasagiline |
PLGA |
SKN-AS cell culture, H2O2 neurotoxin.
Animal study: advanced RT model of PD. Male Wistar rats. |
[70] |
| Rasagiline |
Polycaprolactone |
Animal study: RT-induced model of PD. Male Sprague Dawley rats. |
[22] |
Dopamine
agonists |
Dopamine |
Poly(β-aminoester) |
Cell cultures: SH-SY5Y cells, rat primary astrocytes, embryonic midbrain cultures. |
[76] |
| Ropinirole |
PLGA |
SKN-AS cell culture, H2O2 neurotoxin.
Animal study: RT-induced model of PD. Male Wistar rats. |
[77] |
| COMT inhibitors |
Tolcapone |
PLGA |
Animal study: RT-induced model of PD. Male Wistar rats. |
[78] |
| Alpha-synuclein-targeting agents |
α-syn + Rapamycin |
Glucan |
Animal study: transgenic PDGFβ α-syn. Male and female Line D mice. |
[87] |