Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Catheter Ablation (CA) is an effective therapeutic option in treating atrial fibrillation (AF). Persistent AF represents the advanced stage during the progression of AF. “AF begets AF” is recognized as a main mechanism for the persistence of AF: a complex situation involving triggers and substrate (i.e., structural, electrical, and autonomic remodeling). Previous meta-analysis of RCTs including 809 persistent AF patients (mean age 60 years, mean LAD 46 mm) has already shown that PVI based CA is superior to AADs in preventing recurrence of atrial tachyarrhythmia among patients with persistent AF.
- atrial fibrillation
- ablation
- rhythm control
1. CA in Treating Persistent AF and Longstanding Persistent AF
The recent PRECEPT trial employed contact force-sensing RF catheter guided by 3-D mapping system and lesion formation surrogates for PVI based ablation of persistent AF (N = 333, mean age 65 years, history of AF 1.3 years, mean LAD 42 mm, mean LVEF 56%). Linear ablation was only performed in cases with documented macro-re-entry atrial tachycardia (AT) or typical atrial flutter (AFL). Using standard electrocardiogram (ECG)/Holter monitoring, the PRECEPT study demonstrated a single procedure success rate around 70% at one year [1]. Randomized trials using different technologies for PVI in treating relatively healthy patients with persistent AF (mean age 66 years, history of AF 2 years, mean LAD 43 mm, mean LVEF 61%) reported similar ablation success rate around 70% at one year [2][3].
The randomized STAR AF II trial compared PVI vs. PVI plus (linear ablation vs. complex fractionated electrograms ablation) among patients with “late” persistent AF (N = 589, mean age 60 years, history of AF 4 years, mean LAD 45 mm, mean LVEF 56%). Using standard ECG/Holter monitoring, the STAR AF II study showed that 60% of the patients in the PVI group were free from recurrent AF during one year follow-up, and the study found no further reduction in AF recurrence when linear ablation or ablation of complex fractionated electrograms was performed in addition to PVI [4].
The ablation success rate appeared to be notably higher among patients with early persistent AF than those with late persistent AF, and this seemed to be consistent with the results from other recent studies [5][6][7][8].
2. Adjunctive Ablation Strategies beyond PVI in Treating Persistent AF
2.1. Ablation of Atrial Low Voltage Area
Structural remodeling characterized by atrial fibrosis and enlargement is often accompanied during the progression of AF, and it is known that dilated atrium is an independent risk factor of recurrent arrhythmia after rhythm control. The previous DECAAF Study demonstrated that AF patients who had early-stage atrial fibrosis carried relatively lower risk of recurrent atrial tachyarrhythmia (15.3%, 95% CI: 7.6–29.6%) as compared to those who had late-stage atrial fibrosis 51.1% (95% CI: 32.8–72.2%) [9]. Substrate formation has been recognized as an important mechanism for arrhythmia. Elimination of the arrhythmogenic ventricular substrate has been shown to suppress ventricular arrhythmias in patients with ischemic cardiomyopathy; however, whether or not additional ablation of the fibrotic atrial substrate further improves the success of CA in AF remains controversial.
The most recent DECAAF II trial tested the hypothesis that magnetic resonance imaging (MRI) guided atrial fibrosis area ablation in addition to PVI is superior to PVI alone in improving ablation success in patients with persistent AF [10]. A total of 843 patients (mean age 62.1 years) were randomized, patients were categorized in I (mild)-IV (severe) stages according to atrial fibrosis level. The study found that, consistent with the results of the initial DECAAF study, the extension of baseline atrial fibrosis level was correlated with atrial tachyarrhythmia recurrence after CA. Results after CA based on intention-to-treat (ITT) analysis showed no significant difference in atrial tachyarrhythmia (ATa) recurrence between groups in the overall study population during one year follow-up, Interestingly, per protocol analysis showed significantly less ATa recurrence of substrate ablation in patients with stage I or II (<20%) atrial fibrosis, whereas there was no benefit of fibrosis ablation on ATa recurrence in patients with stage III or IV atrial fibrosis [10].
2.2. Left Atrial Posterior Wall Isolation
The Left atrial posterior wall connecting the septal and lateral PVs has been identified as an arrhythmogenic region contributing to the initiation and maintenance of AF. Electrical isolation the left atrial posterior wall (PWI) has been shown to improve the ablation outcome.
The recent POBI-AF trial randomized 217 patients with persistent AF (73.3% longstanding persistent AF) to ablation with PVI alone or PVI + PWI. The freedom from ATa recurrence showed no significant difference between the PVI + PWI vs. PVI group (55.9% vs. 50.5%) after a mean follow-up of 16 months [11].
Cryoballoon (CB) has been established as a powerful tool for PVI and may create a more homogeneous and durable lesion [12]. A recent RCT investigated the effects of concomitant PVI + PWI using CB. One hundred and ten persistent AF (35% LS AF, mean LAD: 44 mm, mean LVEF 60%) were randomized into PVI or PVI + PWI. RF touch up was required in 7.3% patients to complete PVI and in 45% patients to complete PWI. One year follow-up demonstrated significantly higher freedom from ATa recurrence in the PVI + PWI group vs. PVI (74.5% vs. 54.5%) without compromising safety [13].
Recent large sized meta-analysis included 26 studies with 3287 patients with AF (age 61.7 ± 10.8 years) [14]. Procedural success to achieve PWI was 92.8%. The mean follow-up was 15.2 ± 8.4 months. For patients with paroxysmal AF, adjunctive PWI did not reduce the recurrence of all atrial arrhythmias or AF; whereas for patients with persistent AF, adjunctive PWI was associated with substantially lower recurrence of all atrial arrhythmias and AF, this finding remaining consistent when randomized data were included. Adjunctive PWI using either radiofrequency or a cryoballoon reduced AF recurrence, and primarily using cryoballoon seemed to be associated with lower recurrence rate of atrial tachycardias and/or atrial flutter. The incidence of procedural adverse events between PVI + PWI (3.2%) and PVI (2.8%) groups was low and similar. This meta-analysis indicated that patients with persistent AF appear to benefit from adjunctive PWI, and the ablation technology and/or approach may affect the clinical outcome of PWI [14].
2.3. Ablation Vein of Marshall
The vein (ligament) of Marshall (VOM) contains innervation and electrical triggers to initiate AF. VOM ethanol infusion has been shown as a feasible treatment for atrial tachyarrhythmia by facilitating the block of mitral isthmus [15]. Repeat procedure data also showed that VOM ethanol infusion was associated with greater lesion durability and higher rate of sustained mitral isthmus block as compared with radiofrequency catheter ablation [16]. The recent VENUS trial randomized 343 persistent AF patients (53% LS AF, mean LAD 46, LVEF 53%) to CA or CA + VOM Ethanol Infusion. VOM Ethanol Infusion was successful in 84% of patients. One year follow-up showed that CA + VOM ethanol infusion was associated with significantly higher freedom from ATa recurrence as compared with CA (49.2% vs. 38%) without compromising the safety [17]. The post hoc analysis showed that adjunctive VOM ethanol infusion improved the ablation outcomes (59% vs. 39.1%) only when associated with effective mitral isthmus block [18].
2.4. Left Atrial Appendage Isolation/Ablation
Left atrial appendage (LAA) has been recognized as a trigger source of AF/AT, and left atrial appendage isolation (LAAI) may suppress AF/AT recurrence. The previous BELIEF Trial randomized 173 long-standing persistent AF into LAAI plus standard ablation or standard ablation [19]. In this study, standard ablation was defined as PVI, PWI, left atrial (LA) lines, and non-PV triggers ablation. The mean age was 64 years, mean LAD 48 mm, mean LVEF 54%. During a 12-month follow-up, adjunctive LAAI was associated with significantly higher freedom from ATa as compared with standard ablation (56% vs. 28%). Notably, trigger from the LAA was identified in about one third of the patients during isoproterenol challenge [19].
A recent meta-analysis included nine studies with a total of 2336 patients. The majority of the patients were persistent AF or long-standing persistent AF, with a mean age of 65 years, mean LAD 45 mm, mean LVEF 56%. During a mean follow-up of 41 months, patients who underwent LAAI had significantly higher freedom from ATa recurrence than patients who underwent standard ablation (69.3% vs. 46.4%), and there was no significant difference in the procedural complications between the two groups [20].
Either RF or cryoballoon can be used for LAAI. When using RF ablation, LAAI can be achieved by wide-area linear ablation (including left atrial anterior line, left atrial roof line and left atrial mitral isthmus line). When using cryoballoon, similarly to PVI, LAAI can be achieved by directly occluding and freezing the LAA ostia. Recent non-randomized study found that LAAI can be more readily achieved by using cryoballoon, whereas the 1-year ATa recurrence-free rate was significantly higher in patients with LAAI following RF-guided wide area LAAI (RF:76.3% vs. CB:56.7%, p = 0.0017) [21].
Evidence has shown that electrical LAAI can be associated with increased risk of LAA thrombosis even under sinus rhythm because of loss of the LAA contractibility [22][23].
The limited efficacy of endocardial CA for persistent and long-standing persistent AF led to the development of a minimally invasive hybrid convergent (epicardial/endocardial) ablation approach in order to achieve more comprehensive, durable, transmural lesions. The recent CONVERGE trial randomized 153 patients with persistent and long-standing persistent AF to undergo Hybrid Convergent ablation or endocardial CA [24]. During the 1-year follow-up, the rate of freedom from AF/AT was significantly higher in the Hybrid Convergent group than that in the endocardial CA group (67.7% vs. 50.0%) [24]. At 1.5 years assessed by 7-day Holter, 74% in the Hybrid Convergent group and 55% in the endocardial CA patients experienced ≥90% AF burden reduction [24]. However, patients in the Hybrid Convergent group had more major adverse events (2.9% within one week post-procedure, and 4.9% between one week and 1month post-procedure) compared to endocardial CA group (0%) [24].
For patients with persistent AF, PVI remains the foundation ablation strategy. As above discussed, there have been studies showing improved outcome when PVI combined with different ablation strategies in selected patient group; besides, other ablation concepts, such as rotor ablation, and cardioneuroablation, have also been proposed. The additional merit of such ablation strategies in persistent AF still needs to be warranted. Questions with respect to proper patient selection, optimal timing to perform adjunctive ablation, choosing of pertinent ablation strategy, and selection of efficacious and safe ablation technology, remain to be answered (Figure 1).
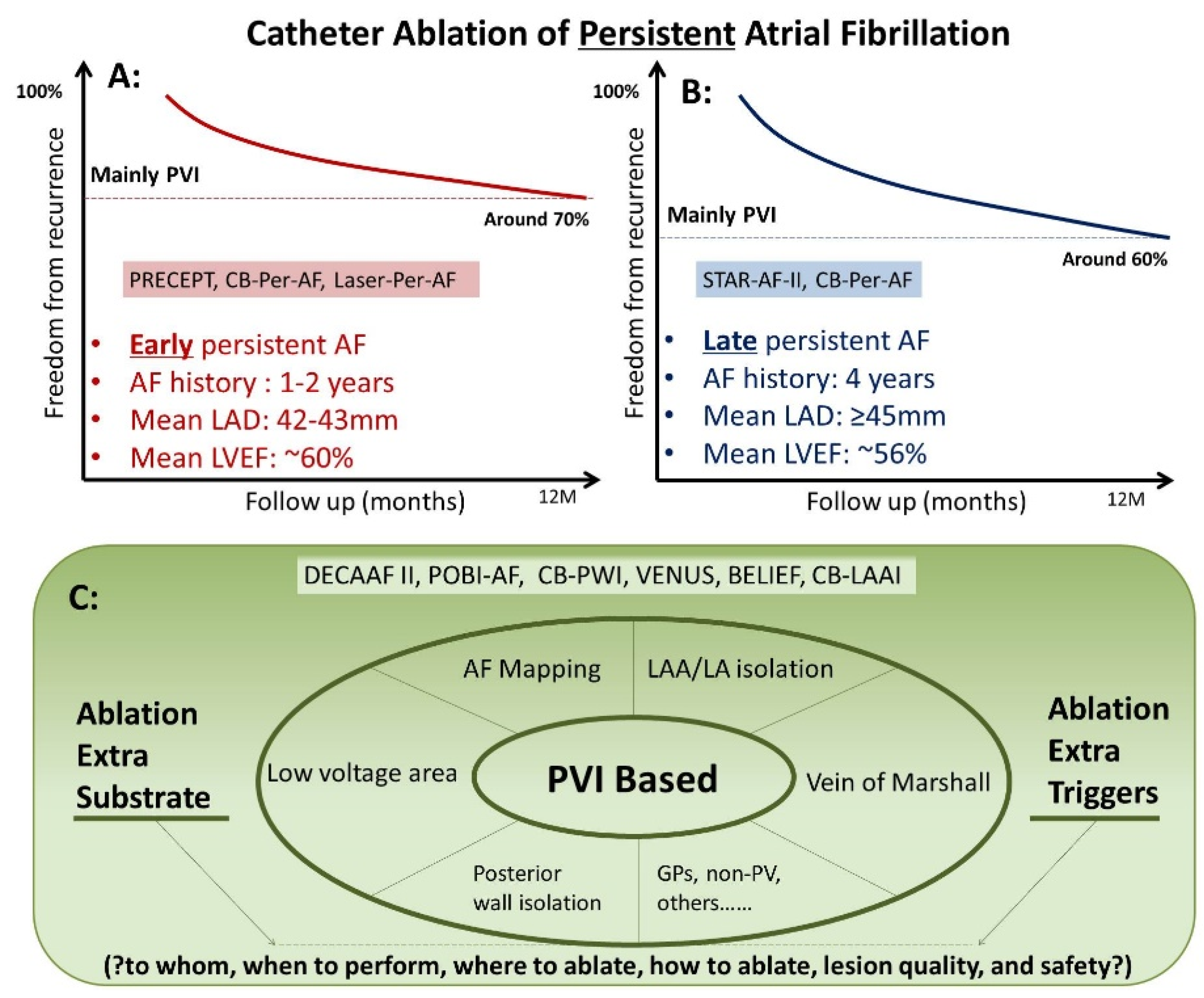
Figure 1. Catheter Ablation of Persistent Atrial Fibrillation. (A) Catheter ablation in “early” persistent AF. (B) Catheter ablation in “late” persistent AF. (C) Catheter ablation in non-PV sites.
This entry is adapted from the peer-reviewed paper 10.3390/jcm11226871
References
- Mansour, M.; Calkins, H.; Osorio, J.; Pollak, S.J.; Melby, D.; Marchlinski, F.E.; Athill, C.A.; Delaughter, C.; Patel, A.M.; Gentlesk, P.J.; et al. Persistent Atrial Fibrillation Ablation With Contact Force-Sensing Catheter: The Prospective Multicenter PRECEPT Trial. JACC Clin. Electrophysiol. 2020, 6, 958–969.
- Schmidt, B.; Neuzil, P.; Luik, A.; Osca Asensi, J.; Schrickel, J.W.; Deneke, T.; Bordignon, S.; Petru, J.; Merkel, M.; Sediva, L.; et al. Laser Balloon or Wide-Area Circumferential Irrigated Radiofrequency Ablation for Persistent Atrial Fibrillation: A Multicenter Prospective Randomized Study. Circ. Arrhythmia Electrophysiol. 2017, 10, e005767.
- Chun, J.K.R.; Bordignon, S.; Last, J.; Mayer, L.; Tohoku, S.; Zanchi, S.; Bianchini, L.; Bologna, F.; Nagase, T.; Urbanek, L.; et al. Cryoballoon Versus Laserballoon: Insights From the First Prospective Randomized Balloon Trial in Catheter Ablation of Atrial Fibrillation. Circ. Arrhythmia Electrophysiol. 2021, 14, e009294.
- Verma, A.; Jiang, C.Y.; Betts, T.R.; Chen, J.; Deisenhofer, I.; Mantovan, R.; Macle, L.; Morillo, C.A.; Haverkamp, W.; Weerasooriya, R.; et al. Approaches to catheter ablation for persistent atrial fibrillation. New Engl. J. Med. 2015, 372, 1812–1822.
- Hussein, A.; Das, M.; Riva, S.; Morgan, M.; Ronayne, C.; Sahni, A.; Shaw, M.; Todd, D.; Hall, M.; Modi, S.; et al. Use of Ablation Index-Guided Ablation Results in High Rates of Durable Pulmonary Vein Isolation and Freedom From Arrhythmia in Persistent Atrial Fibrillation Patients: The PRAISE Study Results. Circ. Arrhythmia Electrophysiol. 2018, 11, e006576.
- Ciconte, G.; Baltogiannis, G.; de Asmundis, C.; Sieira, J.; Conte, G.; Di Giovanni, G.; Saitoh, Y.; Irfan, G.; Mugnai, G.; Hunuk, B.; et al. Circumferential pulmonary vein isolation as index procedure for persistent atrial fibrillation: A comparison between radiofrequency catheter ablation and second-generation cryoballoon ablation. Europace 2015, 17, 559–565.
- Omran, H.; Gutleben, K.J.; Molatta, S.; Fischbach, T.; Wellmann, B.; Horstkotte, D.; Körber, B.; Nölker, G. Second generation cryoballoon ablation for persistent atrial fibrillation: An updated meta-analysis. Clin. Res. Cardiol. 2018, 107, 182–192.
- Liu, X.H.; Gao, X.F.; Jin, C.L.; Chen, C.F.; Chen, B.; Xu, Y.Z. Cryoballoon versus radiofrequency ablation for persistent atrial fibrillation: A systematic review and meta-analysis. Kardiol. Pol. 2020, 78, 20–29.
- Marrouche, N.F.; Wilber, D.; Hindricks, G.; Jais, P.; Akoum, N.; Marchlinski, F.; Kholmovski, E.; Burgon, N.; Hu, N.; Mont, L.; et al. Association of atrial tissue fibrosis identified by delayed enhancement MRI and atrial fibrillation catheter ablation: The DECAAF study. JAMA 2014, 311, 498–506.
- Marrouche, N.F.; Greene, T.; Dean, J.M.; Kholmovski, E.G.; Boer, L.M.; Mansour, M.; Calkins, H.; Marchlinski, F.; Wilber, D.; Hindricks, G.; et al. Efficacy of LGE-MRI-guided fibrosis ablation versus conventional catheter ablation of atrial fibrillation: The DECAAF II trial: Study design. J. Cardiovasc. Electrophysiol. 2021, 32, 916–924.
- Lee, J.M.; Shim, J.; Park, J.; Yu, H.T.; Kim, T.H.; Park, J.K.; Uhm, J.S.; Kim, J.B.; Joung, B.; Lee, M.H.; et al. The Electrical Isolation of the Left Atrial Posterior Wall in Catheter Ablation of Persistent Atrial Fibrillation. JACC Clin. Electrophysiol. 2019, 5, 1253–1261.
- Kuck, K.H.; Albenque, J.P.; Chun, K.J.; Fürnkranz, A.; Busch, M.; Elvan, A.; Schlüter, M.; Braegelmann, K.M.; Kueffer, F.J.; Hemingway, L.; et al. Repeat Ablation for Atrial Fibrillation Recurrence Post Cryoballoon or Radiofrequency Ablation in the FIRE AND ICE Trial. Circ. Arrhythmia Electrophysiol. 2019, 12, e007247.
- Aryana, A.; Allen, S.L.; Pujara, D.K.; Bowers, M.R.; O’Neill, P.G.; Yamauchi, Y.; Shigeta, T.; Vierra, E.C.; Okishige, K.; Natale, A. Concomitant Pulmonary Vein and Posterior Wall Isolation Using Cryoballoon With Adjunct Radiofrequency in Persistent Atrial Fibrillation. JACC Clin. Electrophysiol. 2021, 7, 187–196.
- Jiang, X.; Liao, J.; Ling, Z.; Meyer, C.; Sommer, P.; Futyma, P.; Martinek, M.; Schratter, A.; Acou, W.J.; Wang, J.; et al. Adjunctive Left Atrial Posterior Wall Isolation in Treating Atrial Fibrillation: Insight From a Large Secondary Analysis. JACC Clin. Electrophysiol. 2022, 8, 605–618.
- Kamakura, T.; Derval, N.; Duchateau, J.; Denis, A.; Nakashima, T.; Takagi, T.; Ramirez, F.D.; André, C.; Krisai, P.; Nakatani, Y.; et al. Vein of Marshall Ethanol Infusion: Feasibility, Pitfalls, and Complications in Over 700 Patients. Circ. Arrhythmia Electrophysiol. 2021, 14, e010001.
- Nakashima, T.; Pambrun, T.; Vlachos, K.; Goujeau, C.; André, C.; Krisai, P.; Ramirez, F.D.; Kamakura, T.; Takagi, T.; Nakatani, Y.; et al. Impact of Vein of Marshall Ethanol Infusion on Mitral Isthmus Block: Efficacy and Durability. Circ. Arrhythmia Electrophysiol. 2020, 13, e008884.
- Valderrábano, M.; Peterson, L.E.; Swarup, V.; Schurmann, P.A.; Makkar, A.; Doshi, R.N.; DeLurgio, D.; Athill, C.A.; Ellenbogen, K.A.; Natale, A.; et al. Effect of Catheter Ablation With Vein of Marshall Ethanol Infusion vs Catheter Ablation Alone on Persistent Atrial Fibrillation: The VENUS Randomized Clinical Trial. JAMA 2020, 324, 1620–1628.
- Lador, A.; Peterson, L.E.; Swarup, V.; Schurmann, P.A.; Makkar, A.; Doshi, R.N.; DeLurgio, D.; Athill, C.A.; Ellenbogen, K.A.; Natale, A.; et al. Determinants of outcome impact of vein of Marshall ethanol infusion when added to catheter ablation of persistent atrial fibrillation: A secondary analysis of the VENUS randomized clinical trial. Heart Rhythm 2021, 18, 1045–1054.
- Di Biase, L.; Burkhardt, J.D.; Mohanty, P.; Mohanty, S.; Sanchez, J.E.; Trivedi, C.; Güneş, M.; Gökoğlan, Y.; Gianni, C.; Horton, R.P.; et al. Left Atrial Appendage Isolation in Patients With Longstanding Persistent AF Undergoing Catheter Ablation: BELIEF Trial. J. Am. Coll. Cardiol. 2016, 68, 1929–1940.
- Romero, J.; Gabr, M.; Patel, K.; Briceno, D.; Diaz, J.C.; Alviz, I.; Trivedi, C.; Mohanty, S.; Polanco, D.; Della Rocca, D.G.; et al. Efficacy and safety of left atrial appendage electrical isolation during catheter ablation of atrial fibrillation: An updated meta-analysis. Europace 2021, 23, 226–237.
- Tohoku, S.; Chen, S.; Bordignon, S.; Chun, J.K.; Schmidt, B. Hot or cold? Feasibility, safety, and outcome after radiofrequency-guided versus cryoballoon-guided left atrial appendage isolation. J. Arrhythmia 2022, 38, 316–326.
- Chen, S.; Schmidt, B.; Bordignon, S.; Bologna, F.; Lindhoff-Last, E.; Chun, K.R.J. Thrombus Formation in Isolated Left Atrial Appendage After Multiple Atrial Fibrillation Ablations Despite Oral Anticoagulation Followed by Percutaneous Appendage Closure. JACC Clin. Electrophysiol. 2019, 5, 398–400.
- Chen, S.; Schmidt, B.; Tohoku, S.; Trolese, L.; Bordignon, S.; Chun, K.R.J. Transesophageal echocardiography-guided closure of electrically isolated left atrial appendage to constrain a rapidly growing thrombus despite anticoagulation and sinus rhythm. J. Cardiovasc. Electrophysiol. 2020, 31, 247–249.
- DeLurgio, D.B.; Crossen, K.J.; Gill, J.; Blauth, C.; Oza, S.R.; Magnano, A.R.; Mostovych, M.A.; Halkos, M.E.; Tschopp, D.R.; Kerendi, F.; et al. Hybrid Convergent Procedure for the Treatment of Persistent and Long-Standing Persistent Atrial Fibrillation: Results of CONVERGE Clinical Trial. Circ. Arrhythmia Electrophysiol. 2020, 13, e009288.
This entry is offline, you can click here to edit this entry!