Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Subjects:
Pharmacology & Pharmacy
Drug carriers are used to penetrate the biological barriers and deliver the requisite active pharmaceutical ingredients (API). This has greater significance for medication in arthritis therapies because the inflammatory progression of rheumatoid arthritis (RA) and osteoarthritis (OA) is complex, intertwined, and influenced by one another. For this purpose, the drug delivery systems (DDS) of this carrier are currently being investigated with exogenous triggers and endogenous stimuli. This flexible-release invention will solve the problems of multiple implantations and local toxic accumulation at the lesion sites.
- exogenous triggers
- endogenous stimuli
- drug delivery systems
1. Introduction
Programmable arthritis therapy [1] is in high demand now because the current therapy still lacks efficacy [2] and no recovery therapy has been discovered. Arthritis therapy is complex, intertwined, and progressively influenced by rheumatoid arthritis (RA) and osteoarthritis (OA) [3]. The most difficult part is the progression of pathological inflammation from OA to RA, which involves mediators, such as synovial hyperplasia and pannus synovitis [4]. Generally, RA and OA are chronic and joint-degenerative diseases, respectively, that are classified as inflammatory arthritis (IA) [5] and non-IA [6], respectively. Commonly, OA and RA are specified for large joints of the hip and knee, and small joints of the hands and wrists, such as metatarsophalangeal and interphalangeal toe joints, respectively [7]. The symptoms of OA begin with joint pain, cartilage degeneration, and osseous overgrowth, whereas RA inherits the OA characteristics and then progresses to cartilage destruction and function loss [7]. These severely restrict the patients’ mobility and activities, resulting in disability and living quality deterioration, respectively.
Although many approaches, such as drug administration routes [8], intra-articular therapies [9], resections [10], reconstruction surgeries [11], and articular cartilage scaffolds [12] [1], have been undertaken, the problems of drug delivery systems (DDS), such as mediate infiltration, pharmacokinetics, pharmacodynamics, efficacy, systemic toxicity, and navigation control, still remain unsatisfactory. Moreover, arthritis therapy involves multiple inflammatory factors, resulting in difficult medication [13]. Therefore, the current therapy is limited to alleviating these disease symptoms [14] or pathological alterations. Nonetheless, they have the same pathological microenvironmental changes that could be used as alterations to design biosensors in DDS [15]. These unique alteration features could be characterised as biosensors [16] in scaffold structures [17] [2], which act as detectors to be sensitively cleaved by the selective endogenous stimuli for active pharmaceutical ingredient (API) releases [18]. As a result, an alternative tissue engineering approach with a better sustained-release feature in DDS holds tremendous promise in target-specified delivery, on-demand stimulation, on-program triggering, and great flexibility [19]. This should be urgently developed towards achieving therapy efficacy and patient compliance in clinical translations [20].
2. Status Quo of Drug Carriers for Arthritis Therapy
The drug carrier for arthritis therapy is progressing from traditional to systemic drug administration routes [8]. The traditional drugs are non-steroidal anti-inflammatory drugs (NSAID) and glucocorticoids, which are commonly used in traditional drug administration routes, such as oral, topical, transdermal, and injection [22]. The systemic drug administration routes, such as intra-articular, surgery, and drug carriers, use API such as disease-modifying anti-rheumatic drugs (DMARD), disease-modifying OA drugs (DMOAD), and biological response regulators [23]. However, the traditional intra-articular therapies, resection, and reconstruction surgeries are still unsatisfactory due to the infiltration, efficacy, drug clearance, and target localisation ability. In particular are the radio-, chemo-, immune-, and hormone therapies after osteosarcoma and tumour surgeries, which may result in systemic side effects [24] such as secondary injury, increased risk of recurrence, and immunological rejection [25,26]. Over a long period of therapy, these may increase the detoxification burdens of the liver, kidney, and bone marrow system, resulting from the toxic doses accumulated [27]. Due to these numerous potential systemic side-effects, it is a complication of therapeutic efficacy that limits their clinical applications. Therefore, a new class of drug carriers with better DDS is continuously being created.
2.1. Historical Development
The historical development of DDS is highlighted with a timeline of their significant discoveries and advancements, as shown in Figure 1. The first drug carrier as hydrogel, mostly used in DDS, was invented by Wichterle and Lím in 1960 via a 3D cross-linked polymer, as shown in the green background in Figure 1 [28]. This hydrogel has become one of the most popular drug carriers because of its nanosize particles, API affinity-based nature, bioactive release control, and injectable designs. The first injectable hydrogel using hyaluronic acid (HA) was invented by Rydell and Balazs in 1971 [29]. Later, HA was most commonly used in pain relief for OA therapy. Until 1980, the hydrogel was used as DDS, becoming popular after a drug-release device with rate-controlling was invented by Lee et al. [30]. Even though many thermal therapies were used before 1986, the thermal stimulus was first introduced by Helme et al., which was used to release immune-reactive substance P for inflammation therapies, as shown in the orange background in Figure 1 [31]. In 1987, the enzymatic stimulus using antigen-induced arthritis was first introduced by Bonanomi et al. to investigate the pharmacokinetics and therapeutic effects [32]. In 1998, the pH stimulus using pH-sensitive P2X receptors [33] was first introduced by Dowd et al. to study peripheral nociceptive afferents in the rat knee joint [34]. P2X receptors are the membrane ion channels that open in response to the binding of extracellular adenosine 5′-triphosphate (ATP). In 2000, the redox stimulus using Cu/Zn-superoxide dismutase (SOD) loaded with Fc receptor was first introduced by Vouldoukis et al. to study apoptosis [35]. In 2014, the electro-ion stimulus using electrostatic interaction between negatively charged proteoglycans and highly positively charged Avidin was first introduced by Bajpayee et al. to investigate its pharmacodynamics effects [36].
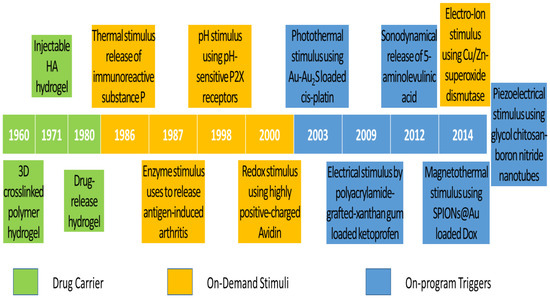
Figure 1. Timeline of significant discoveries and advancements in drug delivery systems with drug carriers, on-demand stimuli, and on-program triggers.
The existing DDS still does not meet the demands of scientists and researchers. Therefore, more flexible drug release systems or those composed of the existing trigger systems are being developed. Ren and Chow (2003) used a photothermal trigger with Au-Au2S-loaded cis-platin for near infra-red (NIR) DDS, as shown in the blue background in Figure 1 [37]. This DDS was a composed stimulation of photo and thermal, where gold linkages were leaked by NIR to free cis-platin for thermal stimulation. In 2009, Kulkarni and Sa used an electrical trigger with polyacrylamide-grafted xanthan-gum-loaded ketoprofen for transdermal DDS [38]. It was a simple study of in vitro drug release influenced by an electrical trigger. In addition, in 2012, Lv et al. used a sonodynamical trigger of 5-aminolevulinic acid therapy to investigate anti-carcinoma efficiency [39]. In these in vivo and in vitro studies using low-intensity US vibration, they found efficacy for SAS cell line proliferation and apoptosis. However, it is regretful that the increment of ROS in the therapy process was not further investigated. In 2014, Mohammad and Yusof developed a magnetothermal trigger using gold-coated superparamagnetic iron oxide nanoparticles (SPIONs@Au) loaded with doxorubicin (Dox) as an anthracycline-type chemotherapy drug for cancer therapy [40]. This in vitro DDS found that the cell viability and proliferation were more efficacious under low frequency oscillatory magnetic stimulation, but there was no effect under thermal stimulation. In the same year, Ricotti et al. used a piezoelectrical trigger of glycol chitosan-boron nitride nanotubes with US transducer stimulation for modulation of F/G-actin [41]. This simulation used a US transducer to convert mechanical stress into electrical signals to investigate actin expression in human dermal fibroblasts. From these highlights of the timeline figure, the on-program trigger began to synergistically correspond to the variations of on-demand stimuli to improve therapeutic efficacy. As a result of this work in the past 10 years, these multiple-stimulus trigger DDS strategies have received dramatic progression due to rapid advanced bio-fabrication technologies.
2.2. Clinical Advancement
In the last 10 years, many novel drug carriers have been developed, but there has not been much completed clinical testing. Thus, there are 10 drug carriers for arthritis-related therapies that have completed the recruitment status of the United States Federal Government clinical trials identifiers (GCTI) [42]. There are four, two, two, one, and one drug carriers successfully invented for knee OA [43], RA [44], osteosarcoma [45], joint infections [46], and peri-implant bone therapies [47], respectively. For the primary tests, we observed that there were 5 pharmacokinetics tests out of 10 [48]. Moreover, the Western Ontario and McMaster Universities OA Index (WOMAC) is used as a self-administered health status for non-IA patients, such as knee OA patients, for pain management [49]. These dominant pharmacokinetics tests mean that the target concentration, distribution volume, and elimination clearance of API are the main considerations of clinical trials [50]. As a result, drug carriers with efficacy, programming release, and patient compliance features are the most preferable choices for scientists.
As shown in Table 1, drug carriers are generally classified into targeted biological-disease-modifying products and products resulting from the conjugation of hydrophilic and hydrophobic functional groups. The microRNA (miR)-146a [51] drug carrier is the targeted biological-disease-modifying product used to release tocilizumab [52,53]. MiR exhibits neurological disease dysfunction in the different stages of the central nervous system, which is not related to this topic and not further elaborated in this review. The other nine drug carriers are created from both functional group conjugations, such as multi-layer lipid in lyophilised formulation (TLC599), diclofenac etalhyaluronate (SI-613), corticosteroid fluticasone propionate with polyvinyl alcohol (PVA) coating (EP-104IAR), HA polynucleotides (PN) [54], tumour necrosis factor (TNF) inhibitor (adalimumab) [55,56], albumin-bound inhibitor with mammalian target of rapamycin (mTOR) (ABI-009) [57], sirolimus derivatives with mTOR inhibitor kinase (temsirolimus), active Ted compound in phosphate ester prodrug (tedizolid phosphate) [58], and platelet-rich fibrin (PRF) [59]. The hydrophilic functional groups are designed to carry API, such as dexamethasone (Dex) sodium phosphate [60], diclofenac [61,62], fluticasone propionate [63], PN [64,65], methotrexate (Mtx) [66,67], nivolumab [68,69], liposomal Dox [70,71], tedizolid (Ted) [72,73], and simvastatin [74,75], which cleave autonomously with endogenous stimuli. However, these inventions still have not solved the systemic toxicity problem due to their long-term uses. Therefore, more advanced inventions with on-program triggers are moving into clinical trials. As a result, this review elaborates on the inventions resulting from the composition of on-demand stimuli and on-program triggers.
Table 1. Drug carriers for arthritis therapy, API, GCTI and year completed, and primary tests.
| Drug Carrier | Arthritis Therapy | API | GCT I, Year | Primary Test | Refs. |
|---|---|---|---|---|---|
| TLC599 (BioSeizer®) | Knee OA | Dex sodium phosphate | NCT03754049, 2022 | Pharmacokinetics | [76,77] |
| SI-613 | Knee OA | Diclofenac (Voltaren®) | NCT03209362, 2021 | WOMAC | [78,79] |
| EP-104IAR | Knee OA | Fluticasone propionate | NCT02609126, 2021 | Pharmacokinetics | [80,81] |
| HA-PN (Condrotide® Plus) | Knee OA | PN | NCT02417610, 2017 | WOMAC | [82,83] |
| miR-146a | RA | Tocilizumab (Actemra®) | NCT03149796, 2017 | miR expressions | [84,85] |
| Adalimumab (Humira®) | RA | Mtx | NCT01185288, 2014 | Pharmacokinetics | [86,87] |
| ABI-009 | Osteosarcoma | Nivolumab (Opdivo®) | NCT03190174, 2021 | Pharmacokinetics | [88,89] |
| Temsirolimus (Torisel®) | Osteosarcoma | Liposomal Dox (Doxil®) | NCT00949325, 2019 | Pharmacokinetics | [90,91] |
| Ted phosphate (Sivextro®) | Joint infections | Ted | NCT03378427, 2021 | Immuno-compromised | [92,93] |
| PRF | Peri-implant bone | Simvastatin (Zocor®) | NCT05008068, 2021 | Bone regeneration | [94,95] |
This entry is adapted from the peer-reviewed paper 10.3390/ph15111330
References
- Yan Yik Lim; Azizi Miskon; Ahmad Mujahid Ahmad Zaidi; CuZn Complex Used in Electrical Biosensors for Drug Delivery Systems. Materials 2022, 15, 7672, 10.3390/ma15217672.
- Yan Yik Lim; Azizi Miskon; Ahmad Mujahid Ahmad Zaidi; Megat Mohamad Hamdan Megat Ahmad; Muhamad Abu Bakar; Numerical Simulation Study on Relationship between the Fracture Mechanisms and Residual Membrane Stresses of Metallic Material. Journal of Functional Biomaterials 2022, 13, 20, 10.3390/jfb13010020.
This entry is offline, you can click here to edit this entry!