Ventricular arrhythmias (VA) are a major cause of sudden cardiac death (SCD). Echocardiography is the first widely available imaging tool which guides VA management strategies. Along with other invasive and noninvasive imaging techniques, it provides essential information for identification of VA substrate such as differentiation between ischemic and non-ischemic etiology and identification of structural heart disease. Both classic as well as novel echocardiographic techniques such as left ventricular strain measurement and mechanical dispersion assessment provide prognostic information and assist in risk stratification. Furthermore, intracardiac echocardiography may have an adjunctive role for the VA ablation by providing real-time visualization of cardiac structures, continuous monitoring of catheter location and early recognition of procedural complications.
1. Introduction
Ventricular arrhythmias (VA) consist of a large spectrum of ventricular rhythm disturbances ranging from premature ventricular complexes to ventricular tachycardia and fibrillation. VA are a major cause of sudden cardiac death (SCD) and a significant burden on the patient’s quality of life. In the majority of cases, VA are associated with structural heart disease.
Cardiac imaging plays an essential role in revealing the underlying etiology of VA and for SCD risk stratification. Echocardiography is the first readily available, inexpensive and accurate imaging tool used to identify the structural changes associated with VA. It is usually followed by multimodality imaging techniques such as cardiac magnetic resonance (CMR), cardiac computed tomography (CT) and nuclear imaging which bring additional information about the VA substrate. Basic echocardiography measurements such as left ventricle ejection fraction (LVEF) have long been used to assess the risk of SCD and current guidelines still rely on it for the indication of a implantable cardiac defibrillator (ICD) [
1].
Substrate ablation is an efficient interventional treatment for VA. For a safe and successful ablation there is a need to understand anatomical VA substrate along with the electric substrate defined by the electroanatomic mapping (EAM). This review will focus on the necessary information provided by the echocardiography prior to the VA ablation procedure.
2. Role of Echocardiography in Identification of VA Substrate
2.1. VA in Structural Heart Disease
Echocardiography is useful in the diagnosis of structural heart disease [
2]. Transthoracic echocardiography (TTE) is a widely available imaging technique which offers valuable information about VA substrate. The main objectives of TTE evaluation are assessment of left ventricle (LV) systolic function with estimation of LVEF, differential diagnosis between ischemic versus nonischemic etiology, assessment of valve function [
3], identification of congenital heart disease [
3] and different cardiomyopathies [
3].
For the evaluation of LV systolic function, LVEF is the main parameter used in VA management. The ESC guidelines recommend performing echocardiography in all patients with suspected or known VA for assessment of LV function and identification of structural substrate [
1]. In patients with structural heart disease, a LVEF < 35% estimated by echocardiography is associated with increased risk of VA and SCD [
1]. Furthermore, indications for ICDs in primary prevention of SCD rely on LVEF [
1]. The LVEF may be estimated using 2D or 3D LV volumes [
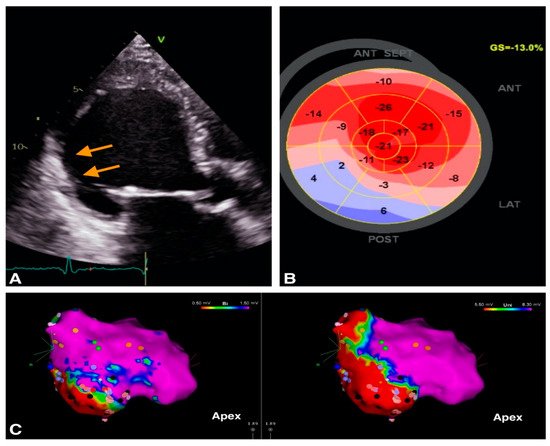
1]. Furthermore, TTE can identify segmental LV contraction abnormalities and describe myocardial scars which may represent VA substrate (
Figure 1).
Figure 1. Example of image integration from a patient with VT and old myocardial infarction; (A). 2D apical 3 chambers view showing the thin, hyperechogenic inferolateral wall (orange arrows). (B). Bull’s eye representation of peak longitudinal strain showing positive values in inferior wall providing a description of the myocardial scar (C) Electroanatomic bipolar (left) and unipolar (right) voltage maps in septal view, with an inferior area of low voltage corresponding to the scar identified by echocardiography.
Transthoracic and transesophageal echocardiography are the routine tools for the diagnosis and severity assessment of underlying valvular heart disease which may contribute to VA occurrence.
Echocardiography plays a significant role in the diagnosis and in management of patients with congenital heart disease and VA. Several studies have shown that right ventricle (RV) and LV dysfunction are risk factors for VA in congenital heart disease patients [
2]. It is mandatory to establish the current status of the congenital heart disease and the need of correcting residual complications in order to limit the risk of VA recurrence. A frequent clinical scenario is the operated patient with tetralogy of Fallot with severe residual pulmonary regurgitation and severe dilatation of RV who develops ventricular tachycardia (VT). The treatment of pulmonary stenosis/regurgitation is discussed to promote RV reverse remodeling and maybe decrease the risk of malignant polymorphic VA [
4].
A multicenter study performed by Koyak et al. showed that moderate to severe systemic or subpulmonary ventricular dysfunction were associated with a high risk of SCD, especially in adults with transposition of great arteries, Eisenmenger physiology and surgically repaired tetralogy of Fallot [
5].
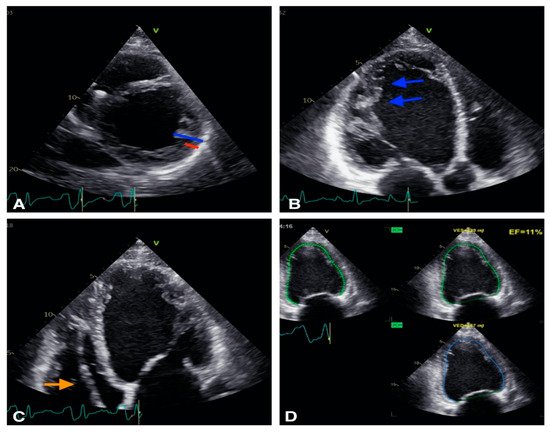
Finally, echocardiography may diagnose cardiomyopathy as the substrate for VA (Figure 2).
Figure 2. Example of a patient with non-compaction cardiomiopathy. (A): 2D short axis view, the non compaction myocardium (blue) is twice thicker than the compacted myocardium (red). (B): 2D apical 3 chambers view, trabeculations are visible (blue arrows). (C): 2D apical 4 chambers view: defibrillator lead is visibile in right ventricle (orange arrow). (D): Biplane EF is calculated at 11% showing severe LV systolic dysfunction.
The established echocardiographic criteria for diagnosis of the different cardiomyopathies are summarized in
Table 1. However, CMR provides more precise information of VA substrate, as it is able to distinguish between ischemic and non-ischemic etiology and detect subtle structural abnormalities such as myocarditis, sarcoid or amyloid cardiomyopathies [
6]. CMR also brings incremental information for the diagnosis of HCM and ARVD [
6].
Table 1. Echocardiographic criteria for the diagnosis of cardiomyopathy.
| Cardiomyopathy |
Echocardiographic Parameters |
| HCM [7,8,9] |
- -
-
LV maximal wall thickness > 15 mm *
- -
-
Ratio of septal and posterior wall thickness ratio > 1.3 **
|
| ARVC [10] |
- -
-
Major criteria:
Regional RV akinesia, dyskinesia, or aneurysm and one of the following:
- -
-
Minor criteria:
Regional RV akinesia or dyskinesia and one of the following:
|
| NCCM [11] |
- -
-
Presence of numerous trabeculations and recesses: most proeminent at LV apex and least proeminent at the level of mitral valve
- -
-
Ratio of thickness of NC and C myocardial layers at the site of maximal WT averages around 3.5 (2–3.5)
- -
-
>3 trabeculations protrunding from the LV apex to the papillary muscles
- -
-
Maximum linear length of NC-C myocardium
- -
-
Planimetry of NC area on A4C
|
| DCM [12] |
- -
-
LVIDd >112% (2 s.d.) corrected for age and BSA ****
- -
-
LVEF < 45%
- -
-
LVFS < 25%
- -
-
Mitral regurgitation
- -
-
SI < 1.5
- -
-
Septal flash and apical rocking
- -
-
Presence of dysynchrony indices
|
2.2. VA in Structurally Normal Hearts
Almost 50% of SCD events occur in patients without structural heart disease [
1].
Table 2 summarizes the possible etiology of VA in patients without any obvious structural changes. There is data that “normal” structural hearts associated with VA and channelopathies actually show structural changes. A group by Scheirlynck et al. studied 175 patients with Brugada Syndrome (BrS) compared to 82 controls and found that BrS patients had lower longitudinal strain and more heterogeneous contractions than healthy controls [
13]. Furthermore, BrS patients with a history of life-threatening VA had more heterogeneous LV contractions [
13]. Therefore, LV mechanical dispersion may be a risk marker in BrS and its evaluation in prospective studies is needed [
9]. Studies on RV function also seem to be relevant in BrS patients, in whom subtle contractile RV mechanical abnormalities were demonstrated, including impaired RV longitudinal strain and a greater contraction delay between the lateral and the septal aspect of the RV [
14].
Table 2. Etiology of VA.
| VA in Structural Heart Disease |
VA in Structurally Normal Heart |
IHD
pARVC
HCM
DCM
NCCM
Valvular heart disease (i.e., aortic stenosis, mitral valve prolapse)
Congenital heart disease |
Outflow tract VT
Fascicular VT
Interfascicular reentrant VT (Belhassen Tachycardia)
Papillary muscle VA
Channelopathies:
- -
-
Long QT syndrome
- -
-
Short QT syndrome
- -
-
Brugada syndrome
- -
-
Catecholaminergic polymorphic VT
- -
-
Early repolarization syndrome
|
Other studies show an overlap between different VA etiology as for BrS and arrhythmogenic cardiomyopathy [
15]. The presence of arrhythmogenic cardiomyopathy diagnostic criteria in BrS patients was associated with a trend towards higher arrhythmic risk [
15].
Prior to VA ablation, echocardiographic data can be completed with cardiac magnetic resonance (CMR). CMR may be later combined with EAM information. Several studies have confirmed that low endocardial voltage corresponds to the presence of scar tissue as defined by the late gadolinium enhanced CMR [
16]. Pre-procedural CMRs have been extremely helpful in localizing scar tissue in the ventricles and have helped to guide and target the arrhythmogenic tissue with catheter ablation [
17].
This entry is adapted from the peer-reviewed paper 10.3390/diagnostics12092109