2.3. Effects of Growth Hormone on the Sensitivity of Oocytes to Gonadotropins
In some studies, GH supplementation has been shown to reduce the need for gonadotropin and shorten the stimulation time, which suggests that supplementary GH could be capable of increasing the sensitivity of oocytes to gonadotropins [
34,
55,
134]. Indeed, GHR/GH-binding protein knockout mice have been reported to have a significantly lower responsiveness to exogenous gonadotropin treatment [
4,
74]. Additionally, in vivo and ex vivo studies have revealed that GH supplementation as a part of IVF treatment upregulated the expressions of LHR, FSHR, and GHR in human GCs, when isolated after egg collection from women with decreased ovarian reserves [
128,
135]. FSHR and LHR signaling in GCs is required for follicular selection and dominant follicle formation. Interestingly, GH also acts to support the maturation process of luteinization by increasing LHR density and by reducing FSHR expression prior to ovulation [
135]. The stimulation of protein kinase A (PKA) by GH and the prevention of GH-induced effects by PKA blockers have been reported to suggest that both the stimulatory and inhibitory effects of GH on porcine ovarian cells were probably mediated by the cAMP/PKA system. Based on the above evidence, the beneficial effect of GH on gonadotropin responses are probably via the cAMP/PKA pathway. Interestingly, IGF treatment has not been able to improve either fertility or ovarian responsiveness to exogenous gonadotropins [
4]; however, the administration of GH has been experimentally shown to enhance the development of small antral follicles into the gonadotropin-dependent phase in vivo [
136]. Thus, the effects of GH on the gonadotropin responses via the regulations of FSHR, LHR, and GHR, as well as the activation of the cAMP/PKA pathway, may be independent from IGF1.
2.4. Effects of Growth Hormone on Granulosa Cells and Thecal Cells
2.4.1. Steroidogenesis
During ovarian steroidogenesis, cholesterol is transferred from outer mitochondrial membranes to the inner mitochondrial membranes with the help of an acute regulatory protein (StAR), and is then converted into pregnenolone by CYP11A1, which is a rate-limiting enzyme [
137]. Subsequently, CYP17A1 and HSD3B1 sequentially catalyze pregnenolone into androstenedione. Finally, estradiol is generated by the sequential catalyzation of CYP19A1 and HSD17B7 in the GCs [
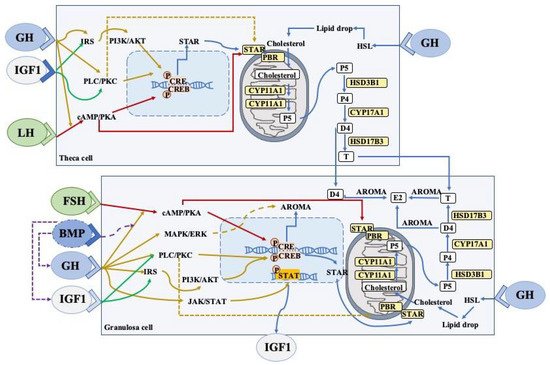
138]. This steroidogenic process can reflect the follicular development and the functions of GCs and theca cells. GH has been demonstrated to affect steroid productions in ovaries, and various intracellular signaling has been shown to be involved in the above process (
Figure 2).
Figure 2. A schematic representation of the major GH/IGF signaling and BMP system networks in ovarian cells (theca and granulosa cells).
GH can induce local IGF1 expression in granulosa cells via JAK-STAT signaling. Both GH and IGF can participate in steroidogenic events and promote cell proliferation via the stimulation of the PLC-PKC and PI3K-AKT pathways, which interact with FSHR and LHR. The expression of aromatase (granulosa cells) and StAR (theca/granulosa cells) is dependent on the CREB pathway. Bone morphogenetic proteins (BMP) suppresses GHR, IGF1, and IGF1R expression, whereas the GH/IGF1 axis downregulates the BMP receptors in the ovaries. Cell proliferation can also be promoted by estrogen and testosterone via autocrine mechanisms.
The abbreviations used are as follows: LHR, luteinising hormone receptor; FSHR, follicle stimulating hormone receptor; cAMP, cyclic AMP; PKA, protein kinase A; CRE, cAMP response element; CREB, cAMP response element binding protein; PLC, phospholipase C, IRS, insulin receptor substrate; PI3K-AKT, phosphoinositide 3-kinase/protein kinase B; StAR, steroidogenic acute regulatory protein; P4, progesterone; P5, pregnenolone; E2, estradiol; D4, androstenedione; T, testosterone; STAT, signal transducer and activator of transcription; AROMA, aromatase, HSL, hormone-sensitive lipase. Arrow, stimulation; Dotted arrows, inhibition.
By binding to the GHRs in the GCs and thecal cells of Graafian follicles, GH has been shown to augment the proliferation of GCs and thecal cells, and to promote steroidogenesis as well [
1,
139]. Increasing numbers of in vitro studies have found that GH supplementation stimulated the synthesis of progesterone in primary GCs cultures, which could be related to the increased expression of CYP11A1 and HSD3B [
8,
140]. Moreover, the GH-increased progesterone has been shown to disappear when conditioned media were treated with antiserum against GH [
8]. However, there have been contradictory reports about the regulation of GH in the FSH-induced estradiol production [
8,
140]. Many years ago, 24 normal patients who received short-term GH treatment showed increased E2 production, which was significantly higher than the increase that was induced by FSH injections without GH administration [
141]. In isolated preantral caprine follicles, GH has been shown to increase FSH-induced estradiol (E2) production, which could be due to the elevated activity or expression of CYP19A1 [
142]. However, another in vitro study found that GH suppressed FSH-induced E2 production, as well as causing reductions in aromatase expression [
140]. Interestingly, GH alone has been reported to be unable to induce any steroidogenic responses [
141], which implied that the GH steroidogenic effects might be dependent on the FSH actions. Additionally, the incubation of GCs with either recombinant chicken GH or conditioned media that predominantly contained a 15 kDa GH isoform has been shown to significantly increase GC proliferation; meanwhile, the knockdown of local ovarian GH with a specific cGH siRNA in hen GC cultures reduced the proliferation rate of GCs [
143]. Thus, GH-mediated disruptions to progesterone and E2 production in GCs may be associated with the expressions of steroidogenic enzymes and the proliferation of GCs.
2.4.2. JAK2-Dependent Signaling Pathway
The binding of GH to the GHR dimer results in the activation of the intracellular Janus Kinase 2 (JAK2) pathway, which can phosphorylate itself and the cytoplasmic regions of GHR [
144], and then subsequently phosphorylates STAT molecules (particularly STAT5a, 5b, 1, and 3). STAT5b is considered to be of the utmost importance as it directly regulates the expression of IGF1 [
145] and has been shown to act as a mediator of GH-induced IGF1 production in rat GCs [
140,
146]. When the transcription molecule STAT is recruited, the subsequently mitogen-activated protein kinases (MAPK)/phosphatidylinositol 3-kinase (PI3K)/protein kinase C (PKC)/phospholipase A2 (PLA2) pathway is stimulated. MAPK activation has been demonstrated to regulate FSH-mediated steroidogenesis in the GCs [
147,
148]. ERK1/2 is involved in the synthesis of progesterone and E2 which is induced by FSH [
149]. GH can also enhance FSH-induced ERK signaling, which is likely to be involved in the effects of GH on FSH-induced E2 and progesterone production [
140]. Considering that the inhibition of IGF1 blocks the GH-induced stimulation of FSH-induced progesterone production, GH affects the production of steroid hormones via the JAK/STAT and ERK pathways, which are functionally involved in the activation of IGF1 expression. Based on the fact that BMP regulates steroidogenesis and the mitosis of GCs, one study revealed that GH/IGF1 actions impaired BMP-SMA and Mad-related protein 1/5/8 signaling, and that BMP in turn inhibited the IGF1 effects that increased FSH-induced E2 production via the suppression of the expression of the GH/IGF1 system [
140]. The effects of GH on the steroidogenesis of GCs have been demonstrated to be enhanced in the presence of the BMP antagonist noggin [
140].
2.4.3. JAK2-Independent Signaling Pathway
Other studies have also found that when GH bound to GHR, the PLC/PKC pathway is also activated, which is independent from JAK2 recruitment [
146,
150]. PKC has been demonstrated to directly trigger cyclic AMP response-element binding protein (CREB)-mediated gene transcription and, subsequently, StAR and/or aromatase expression in GCs, for example [
151]. StAR can bind to cholesterol in the cytosol and transport it to outer mitochondrial membranes, where peripheral-type benzodiazepine receptors (PBRs) are involved in its transport from the outer to inner mitochondrial membranes. However, the phosphorylation of StAR by PKC inhibits the transportation of cholesterol in GCs by interfering in StAR-PBR interactions [
152].
2.4.4. FSHR Pathway
FSH exerts its actions on GCs mainly through the stimulation of the cAMP-PKA pathway [
153,
154,
155]. CREB, which is a PKA substrate, is known to play an important role in the regulation of the FSH responsive genes (
Star and
Cyp19a1) in GCs [
155,
156]. Additionally, the phosphorylation of StAR by PKA stimulates cholesterol transportation by enhancing the interactions between StAR and PBR [
152]. Accumulated evidence has shown that GH supplementation could elevate the expressions of LHR, FSHR, and GHR in human GCs [
128,
135]. Thus, GH can regulate the steroidogenesis of GCs via the FSHR pathway.
2.4.5. GH/IGFs Signaling Pathway
The GH–GHR interaction can induce the production of ovarian IGF1 via the GHR/JAK2/STAT5b pathway [
145]. Several GH-deficient mouse models have shown significantly reduced plasma IGF1 concentrations [
157,
158]. As well as IGF1, other members of the IGF family have also been shown to be influenced by GH [
6]. The IGF system comprises two ligands (IGF1 and IGF2), three receptors (IGF1R, IGF2R, and insulin receptors), six secreted IGF-binding proteins (IGFBPs), and IGFBP proteases [
159]. Female IGF1R knockout mice have been shown to have ovaries with no antral follicles and demonstrate a 90% reduction in serum E2 levels [
160]. Additionally, IGF1 knockout mice have also been shown to exhibit the decreased expression of FSH receptors and, consequently, reduced aromatase expression and E2 secretion [
161]. An in vitro study also confirmed that the inhibition of IGF1 signaling restored GH-induced stimulation of FSH-induced progesterone production, which suggested that endogenous IGF1 could be functionally involved with the effects of GH on progesterone production [
140]. The biological effects of IGF1 have been further demonstrated to be mediated by IGF1 binding proteins, which are synthesized and secreted in human ovarian GCs [
162]. Interestingly, increased free IGF1 has been demonstrated to decrease the synthesis of IGF2R, thereby allowing for more IGF2 to be bioavailable (free) for the induction of steroidogenesis and mitogenesis via the IGF1R [
163]. Thus, the above evidence has suggested that by regulating the sensitivity of GCs to gonadotropin, IGF1 and IGF2 could be important downstream factors of GH in female reproduction and that the physiological effects of GH on ovary functions could be due to the direct and/or indirect action of GH.
2.5. Mitochondrial Functions
Oxidative stress is induced by the overproduction of reactive oxygen species (ROS), which are mainly generated by mitochondria [
164]. Therefore, mitochondrial dysfunction can lead to pathological changes, disruption to the production of normal ATP levels, and increases in the levels of ROS [
165]. Oxidative stress is also considered to be one of the important aspects that causes reproductive dysfunction, including abnormal follicular atresia, ovum meiosis, lower fertilization rates, and delayed embryonic development [
166]. Additionally, oxidative stress can initiate during several reproductive diseases, including PCOS [
167], endometriosis [
168], premature ovarian failure, etc. Mitochondrial dysfunction that is caused by ROS is also involved in reduced oocyte developmental competence and fertilization failure [
165]. Recently, GH has been widely applied in the treatment of the above reproductive pathologies, which could be due to its downregulation of oxidative stress in ovaries. GH has been shown to alleviate the total oxidative stress and oxidative stress index level in follicular fluid, and increase GC mitochondrial membrane potential in Chinese patients with PCOS [
23]. Additionally, the GCs in the above patients suffered from higher apoptosis, which could be associated with the decreased function of the PI3K-AKT signaling pathway; meanwhile, GH could alleviate caspase-dependent apoptosis of GCs and activate the PI3K-AKT signaling pathway in GCs [
169]. Recent studies on mammals have confirmed that the PI3K-AKT signaling pathway could regulate the growth and apoptosis of GCs during follicular development [
170,
171]. Similarly, GH has been found to reduce ROS-induced apoptosis in some types of cells including the vascular endothelium, cardiomyocytes, and neural and skeletal muscle cells, by activating the PI3K-AKT signaling pathway [
172,
173]. Furthermore, GH has been shown to exert protective effects on cisplatin-induced ovarian GC apoptosis by downregulating oxidative stress and enhancing mitochondrial functions (i.e., mitochondrial membrane potential and mtDNA copy numbers) via the Sirt3-Sod2 pathway [
174]. Sirt3 exists in the mitochondrial matrices and participates in the regulation of mitochondrial functions, as well as acting as an oxidative stress sensor and playing a protective role in controlling ROS generation [
175]. In addition to directly reducing the production of ROS, Sirt3 can also regulate the acetylation levels of manganese superoxide dismutase (Sod2), thereby promoting the detoxification of ROS and suppressing mitochondrial oxidative stress [
174]. Thus, GH may alleviate apoptosis by lowering the levels of ROS, elevating mitochondrial membrane potential, and recovering mtDNA copy numbers in GCs.