Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Cardiogenic shock complicating acute myocardial infarction is a complex clinical condition associated with dismal prognosis. Routine early target vessel revascularization remains the most effective treatment to substantially improve outcomes, but mortality remains high. Temporary circulatory support devices have emerged with the aim to enhance cardiac unloading and improve end-organ perfusion.
- cardiogenic shock
- acute myocardial infarction
- mechanical circulatory support
1. Introduction
Cardiogenic shock (CS) is the leading cause of death in acute myocardial infarction (AMI), and it is characterized by tissue hypoperfusion and hypoxia related to low cardiac output [1]. It is often associated with rapid hemodynamic deterioration, unresponsiveness to intensive supportive measures, and high mortality rate [2].
Nationwide databases examining temporal trends in CS have shown inconsistent data regarding the incidence of CS. While some studies demonstrate an increase in the overall incidence of CS in recent years [3], others report a decrease [4,5].
CS complicates approximately 5–10% of AMI’s with a higher incidence in ST elevation myocardial infarction (STEMI) and is more frequently seen among women and patients > 75 years old [3,6].
The clinical and hemodynamic heterogenicity of CS with only few randomized clinical trials evaluating the various therapeutic approaches and recommendations lead to uncertainties as to the best treatment strategies. Thus, management of CS is often challenging and requires early diagnosis and institution of high-quality interdisciplinary care [7]. When treated conservatively, CS carries ~70–80% risk of mortality [8]. In contrast, early reperfusion has been associated with improvements in survival [9]. However, for more than two decades, in-hospital and 1-year mortality remain unchanged and unacceptably high with a reported rate of 40–50% [10].
Supportive pharmacologic and device-based therapies are also frequently utilized with little evidence of benefit [11]. Hence, several mechanical circulatory support (MCS) devices have emerged as a treatment option for CS. Nevertheless, data regarding this MCS devices in CS are still debatable and ambiguous [12].
2. Mechanical Circulatory Support
The main goals of temporary MCS devices are to improve cardiac output by reducing intracardiac filling pressures; reduce left ventricular LV volumes, wall stress, and myocardial oxygen consumption; and ameliorate coronary perfusion to improve tissue perfusion.
MCS devices are designed to provide either a temporary, short-term cardiac output support or a long-term assistance to the left and/or right ventricle. Short-term percutaneous platforms are widely used in the setting of CS, in particular in patients refractory to medical therapy, either alone or in combination. Temporary devices may serve as a bridge to recovery or until further decisions in management are made (bridge to decision), such as the need for long-term support, heart transplantation, or destination therapy. Short-term MCS is increasingly used as a bridge to decision in patients with refractory cardiogenic shock [22]. In a meta-analysis evaluating support duration and clinical outcome of a bridge to decision strategy using multiple temporary MCS devices in CS due to various etiologies, including AMI patients, the mean duration (range) of support duration was 1.6–25 days, the mean (range) rates of conversion to durable VAD was 3–30%, and the mean (range) discharge proportion was 45–66% [22]. Assessment of the utility (and futility) of invasive therapy is complex and often requires shared decision making of the multidisciplinary team caring for the patient, with the patient and family taking into consideration patient wishes and objective clinical information.
Recent studies have shown that standardized approach to CS, including early target vessel revascularization along with early use of MCS along with close monitoring of hemodynamic parameters and markers of target organ perfusion, may improve outcomes [23,24]. However, there is lack of evidence regarding patient selection and the use of a specific device criteria. Thus, MCS candidacy should be evaluated by a multidisciplinary team with expertise in management of cardiac support devices. Currently, the use of MCS in CS has a general class IIa–III level of recommendation depending on the specific MCS device [11].
Options for acute MCS (Figure 1) include the intra-aortic balloon pump (IABP), percutaneous ventricular assist devices (VAD) (Impella, TandemHeart), and veno-arterial extracorporeal membrane oxygenation (VA-ECMO) [25]. The characteristics of the various devices are summarized in Table 2 [10,23,25,26].
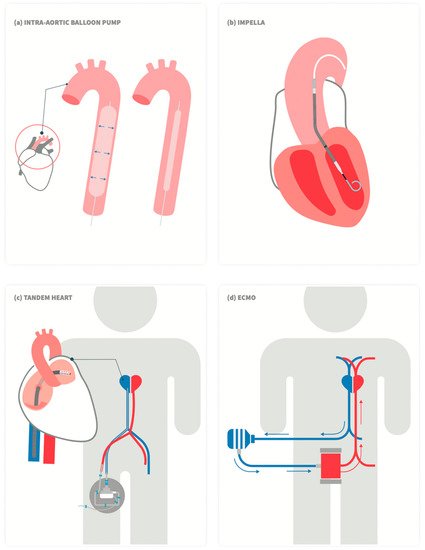
Figure 1. Schematic drawing of commercially available left ventricular percutaneous mechanical support devices. (a) Intra-aortic balloon pump, (b) Impella, (c)TandemHeart, and (d) Veno-arterial (VA) extracorporeal membrane oxygenation (ECMO).
3. Intra-Aortic Balloon Pump (IABP)
Intra-aortic balloon pump (IABP) counter-pulsation is one of the earliest types of short term MCS. It consists of a flexible 30–50 cc helium-filled balloon catheter (7–8F), inserted percutaneously via the femoral artery, connected to a mobile console that times periodic balloon inflation and deflation according to the cardiac cycle. When inflated in diastole (immediately after the closure of the aortic valve), diastolic and mean arterial pressure rise, thus theoretically improving coronary flow and myocardial oxygenation. On the other hand, when rapidly deflated just prior to blood ejection from the LV, it provides immediate systolic blood pressure attenuation and consequently afterload reduction, leading to an increase in stroke volume. Overall, myocardial oxygen demand is reduced [27].
IABP has been investigated in multiple clinical scenarios, including high-risk PCI and CS in the setting of AMI [28,29,30]. One of the most important trials investigating IABP in the setting of CS was the IABP-SHOCK II trial, which randomized 600 patients with CS complicating AMI to routine use of IABP vs. no IABP in addition to early revascularization along with the accepted available medical therapy [31]. At 30 days, no difference in mortality or any secondary endpoint (serum lactate levels, creatinine clearance, C-reactive protein levels, and severity of disease as assessed with the use of the Simplified Acute Physiology Score [SAPS] II) was evident. In addition, long-term mortality also did not differ between the IABP and the control group [32]. Lack of clinical benefit has also been reported in metanalyses [33] and registries [34].
Accordingly, the routine use of IBAP was given a class III indication for CS complicating AMI in the STEMI European guidelines [35]. Moreover, the timing for initiation the use of IABP therapy (before vs. post primary PCI) does not appear to impact short-term and long-term survival in patients with CS complicating AMI undergoing primary PCI [36].
In summary, there is no convincing evidence to support routine use of IABP in post-MI CS patients. Consequently, the overall use of IBAP in the management of ischemic CS is consistently decreasing, with the exception of CS due to severe mitral regurgitation, where the use of IABP is still rated as IIa indication [3,6,35].
4. Impella
Impella (Abiomed Inc., Danvers, MA, USA) is a temporary VAD frequently included in the management of patients with post-AMI CS and as a support measure in PCI for high-risk patients [30,37]. The device requires a large bore access (12–14F) and is introduced retrogradely, via the femoral artery, under fluoroscopic guidance, across the aortic valve. It consists of a pump motor that delivers forward blood flow from the LV into the aorta in a non-pulsatile, continuous fashion. The Impella 2.5 and Impella CP allow for a sustained peak flow of 2.5 L/min and 4.3 L/min, respectively. The Impella 5.0 and Impella 5.5 with SmartAssist require a surgical access to the femoral/subclavian arteries and provide up to 5 L/min and > 6 L/min of blood flow, respectively. By unloading the ventricle, the Impella reduces intracardiac pressures and myocardial oxygen consumption. Coronary blood flow is, theoretically, increased by means of increased blood pressure and reduced LV end diastolic pressure [38]. The new Impella ECP (Expandable CP) (9F) can provide peak flow of > 3.5 L/min [10].
The safety and feasibility of the Impella 2.5 and CP devices have been reported in large registries [39]. Impella was also evaluated in comparison to IBAP in the setting of CS. The ISAR-SHOCK (Efficacy Study of LV Assist Device to Treat Patients With Cardiogenic Shock) trial showed that the use of Impella provided more hemodynamic support than IABP, but there was no difference in the mortality rate between the two devices [40]. The IMPRESS in Severe Shock (IMPella versus IABP Reduces mortality in STEMI patients treated with primary PCI in Severe cardiogenic Shock) study randomized 48 patients with CS complicating AMI to Impella CP vs. IABP. However, there was, again, no significant difference in 30-day and 6-months mortality rates (~50% at 6 months for both groups) [41]. In addition, no mortality difference between groups was observed on long-term 5-year follow up [42]. Nevertheless, in one large cohort of 15,259 consecutive patients with post-MI CS treated with Impella, pre-PCI Impella placement was associated with improved survival as compared with post PCI [43]. Other than the rather disappointing evidence of benefit, the use of Impella has been linked to a greater risk of vascular complications, major bleeding, and stroke compared with the use IABP [10,38,44] (Schrage, 2019, Impella Support for Acute Myocardial Infarction Complicated by Cardiogenic Shock).
The Impella RP (right percutaneous), introduced via the femoral vein, supports the RV. It is utilized to maintain blood flow from the inferior vena cava into the pulmonary artery with peak flow rate > 4 L/min. The RECOVER RIGHT (The Use of Impella RP Support System in Patients With Right Heart Failure) study was the first to suggest the feasibility and safety of the RV support device in selected patients with RV failure [45]. Nevertheless, data regarding its benefit are still scarce. Interestingly, despite the absence of good clinical data to support the use of Impella in CS complicating AMI, studies have reported a substantial and consistent use of VADs in recent years [46].
This entry is adapted from the peer-reviewed paper 10.3390/jcm11175241
This entry is offline, you can click here to edit this entry!