Biocompatible hyaluronic acid (HA, hyaluronan) gel implants have altered the therapeutic landscape of surgery and medicine, fostering an array of innovative products that include viscosurgical aids, synovial supplements, and drug-eluting nanomaterials. However, it is perhaps the explosive growth in the cosmetic applications of injectable dermal fillers that has captured the brightest spotlight, emerging as the dominant modality in plastic surgery and aesthetic medicine. The popularity surge with which injectable HA fillers have risen to in vogue status has also brought a concomitant increase in the incidence of once-rare iatrogenic vaso-occlusive injuries ranging from disfiguring facial skin necrosis to disabling neuro-ophthalmological sequelae. As researchers' understanding of the pathophysiology of these injuries has evolved, supplemented by more than a century of astute observations, the formulation of novel therapeutic and preventative strategies has permitted the amelioration of this burdensome complication.
- hyaluronic acid
- dermal fillers
- hyaluronidase
- urokinase
- fibrinolytic therapy
- skin necrosis
- retinal injury
- cerebrovascular stroke
- pulmonary embolism
- angiosome
1. Introduction
2. Hyaluronan Biophysiology and Aesthetic Applications
2.1. Basic Biochemical Properties and Function
2.2. Physiological HA Biosynthesis and Degradation
2.3. Commercial HA Synthesis and Reversal Agents
3. Pathophysiology of HA-Mediated Vascular Occlusion
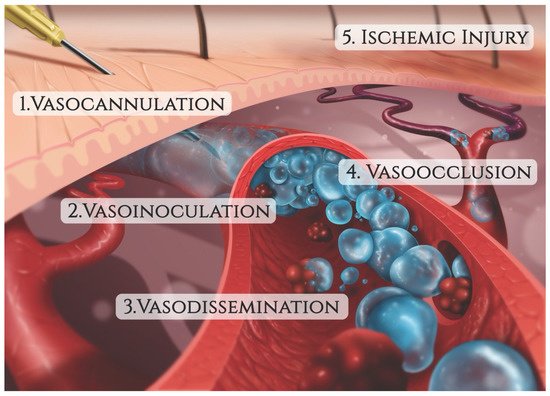
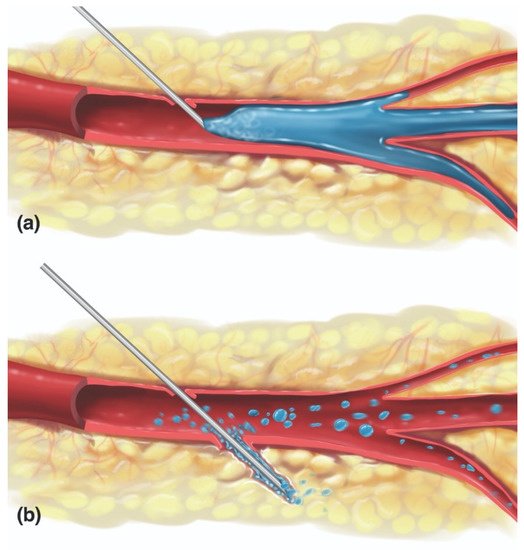
3.1. Vaso-Cannulation
3.2. Vaso-Inoculation
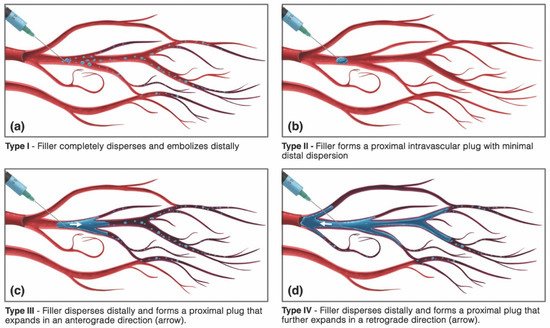
3.3. Vaso-Dissemination
| Arterial * | Venous |
|---|---|
| Muco-Cutaneous/Soft Tissue Necrosis | Local Venous Thrombophlebitis |
| Vision Loss +/− Ophthalmoplegia | Cerebral Sinus Thrombosis |
| Ischemic Cerebral Stroke | Pulmonary Embolism |
| Facial Paralysis/Peripheral Nerve Injury | Myocardial Infarction (PFO **) |
This entry is adapted from the peer-reviewed paper 10.3390/molecules27175398
References
- Hintze, V.; Schnabelrauch, M.; Rother, S. Chemical modification of hyaluronan and their biomedical applications. Front. Chem. 2022, 10, 830671.
- Burdick, J.A.; Prestwich, G.D. Hyaluronic acid hydrogels for biomedical applications. Adv. Mater. 2011, 23, H41–H56.
- American Society of Plastic Surgeons. 2020 Plastic Surgery Statistics Report. 2021. Available online: https://www.plasticsurgery.org/documents/News/Statistics/2020/plastic-surgery-statistics-full-report-2020.pdf (accessed on 15 June 2022).
- Facial Injectables Market. Available online: https://www.fortunebusinessinsights.com/industry-reports/facial-injectables-market-100603 (accessed on 15 June 2022).
- Global Facial Injectable Market Size Report, 2022–2030. Available online: https://www.grandviewresearch.com/industry-analysis/facial-injectables-industry (accessed on 15 June 2022).
- Meyer, K.; Palmer, J. The polysaccharide of the vitreous humor. J. Biol. Chem. 1934, 107, 629–634.
- Highley, C.B.; Prestwich, G.D.; Burdick, J.A. Recent advances in hyaluronic acid hydrogels for biomedical applications. Curr Opin Biotechnol. 2016, 40, 35–40.
- Weissman, B.; Meyer, K. The structure of hyalobiuronic acid and of hyaluronic acid from umbilical cord. J. Am. Chem. Soc. 1954, 76, 1753–1757.
- Chong, B.F.; Blank, L.M.; Mclaughlin, R.; Nielsen, L.K. Microbial hyaluronic acid production. Appl. Microbiol. Biotechnol. 2005, 66, 341–351.
- de Oliveira, J.D.; Carvalho, L.S.; Gomes, A.M.; Queiroz, L.R.; Magalhães, B.S.; Parachin, N.S. Genetic basis for hyper production of hyaluronic acid in natural and engineered microorganisms. Microb. Cell Fact. 2016, 15, 119.
- Selyanin, M.A.; Boykov, P.Y.; Khabarov, V.N.; Polyak, F. The history of hyaluronic acid discovery, foundational research and initial use. In Hyaluronic Acid; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2015.
- Greco, T.M.; Antunes, M.B.; Yellin, S.A. Injectable fillers for volume replacement in the aging face. Facial Plast. Surg. 2012, 28, 8–20.
- Ugarte, A.; Blevins, L.W.; Wills-Kofford, J.C.; Soares, D.J. Dermal filler re-contouring of the aged jawline: A useful non-surgical modality in facial rejuvenation. J. Aesthetic Nurs. 2022, 11, 70–78.
- Fallacara, A.; Baldini, E.; Manfredini, S.; Vertuani, S. Hyaluronic acid in the third millennium. Polymers 2018, 10, 701.
- Volpi, N.; Schiller, J.; Stern, R.; Soltés, L. Role, metabolism, chemical modifications and applications of hyaluronan. Curr. Med. Chem. 2009, 16, 1718–1745.
- Laurent, T.C.; Fraser, J.R. Hyaluronan. FASEB J. 1992, 6, 2397–2404.
- O’Regan, M.; Martini, I.; Crescenzi, F.; De Luca, C.; Lansing, M. Molecular mechanisms and genetics of hyaluronan biosynthesis. Int. J. Biol. Macromol. 1994, 16, 283–286.
- Laurent, U.B.G.; Reed, R.K. Turnover of hyaluronan in the tissues. Adv. Drug Del. Rev. 1991, 7, 237–256.
- Cowman, M.K.; Lee, H.G.; Schwertfeger, K.L.; McCarthy, J.B.; Turley, E.A. The content and size of hyaluronan in biological fluids and tissues. Front. Immunol. 2015, 2, 261.
- Scott, J.E.; Heatley, F. Hyaluronan forms specific stable tertiary structures in aqueous solution: A 13C NMR study. Proc. Natl. Acad. Sci. USA 1999, 27, 4850–4855.
- Liao, Y.-H.; Jones, S.A.; Forbes, B.; Martin, G.P.; Brown, M.B. Hyaluronan: Pharmaceutical characterization and drug delivery. Drug Deliv. 2005, 12, 327–342.
- Dea, I.C.; Moorhouse, R.; Rees, D.A.; Arnott, S.; Guss, J.M.; Balazs, E.A. Hyaluronic acid: A novel, double helical molecule. Science 1973, 179, 560–562.
- Papakonstantinou, E.; Roth, M.; Karakiulakis, G. Hyaluronic acid: A key molecule in skin aging. Dermato-Endocrinology 2012, 4, 253–258.
- Maytin, E.V. Hyaluronan: More than just a wrinkle filler. Glycobiology 2016, 26, 553–559.
- Jordan, A.R.; Racine, R.R.; Hennig, M.J.; Lokeshwar, V.B. The Role of CD44 in Disease Pathophysiology and Targeted Treatment. Front. Immunol. 2015, 6, 182.
- Wang, S.J.; Bourguignon, L.Y. Role of hyaluronan-mediated CD44 signaling in head and neck squamous cell carcinoma progression and chemoresistance. Am. J. Pathol. 2011, 178, 956–963.
- Webber, J.; Jenkins, R.H.; Meran, S.; Phillips, A.; Steadman, R. Modulation of TGFbeta1-dependent myofibroblast differentiation by hyaluronan. Am. J. Pathol. 2009, 175, 148–160.
- Stern, R.; Asari, A.A.; Sugahara, K.N. Hyaluronan fragments: An information-rich system. Eur. J. Cell Biol. 2006, 85, 699–715.
- Caon, I.; Parnigoni, A.; Viola, M.; Karousou, E.; Passi, A.; Vigetti, D. Cell Energy metabolism and hyaluronan synthesis. J. Histochem. Cytochem. 2021, 69, 35–47.
- Itano, N.; Kimata, K. Mammalian hyaluronan synthases. IUBMB Life 2002, 54, 195–199.
- Viola, M.; Vigetti, D.; Karousou, E.; D’Angelo, M.L.; Caon, I.; Moretto, P.; De Luca, G.; Passi, A. Biology and biotechnology of hyaluronan. Glycoconj. J. 2015, 32, 93–103.
- Tammi, R.H.; Passi, A.G.; Rilla, K.; Karousou, E.; Vigetti, D.; Makkonen, K.; Tammi, M.I. Transcriptional and posttranslational regulation of hyaluronan synthesis. FEBS J. 2011, 278, 1419–1428.
- Viola, M.; Bartolini, B.; Vigetti, D.; Karousou, E.; Moretto, P.; Deleonibus, S.; Sawamura, T.; Wight, T.N.; Hascall, V.C.; De Luca, G.; et al. Oxidized low density lipoprotein (LDL) affects hyaluronan synthesis in human aortic smooth muscle cells. J. Biol. Chem. 2013, 288, 29595–29603.
- Bastow, E.R.; Byers, S.; Golub, S.B.; Clarkin, C.E.; Pitsillides, A.; Fosang, A.J. Hyaluronan synthesis and degradation in cartilage and bone. Cell. Mol. Life Sci. 2008, 65, 395–413.
- Jung, H. Hyaluronidase: An overview of its properties, applications, and side effects. Arch. Plast. Surg. 2020, 47, 297–300.
- Girish, K.S.; Kemparaju, K.; Nagaraju, S.; Vishwanath, B.S. Hyaluronidase inhibitors: A biological and therapeutic perspective. Curr. Med. Chem. 2009, 16, 2261–2288.
- Kim, H.J.; Kwon, S.B.; Whang, K.U.; Lee, J.S.; Park, Y.L.; Lee, S.Y. The duration of hyaluronidase and optimal timing of hyaluronic acid (HA) filler reinjection after hyaluronidase injection. J. Cosmet. Laser Ther. 2018, 20, 52–57.
- Kwak, S.S.; Yoon, K.H.; Kwon, J.H.; Kang, W.H.; Rhee, C.H.; Yang, G.H.; Cruz, D.J.M.; Son, W.C. Comparative analysis of hyaluronidase-mediated degradation among seven hyaluronic acid fillers in hairless mice. Clin. Cosmet. Investig. Dermatol. 2021, 8, 241–248.
- Kim, D.-W.; Yoon, E.-S.; Ji, Y.-H.; Park, S.-H.; Lee, B.-I.; Dhong, E.-S. Vascular complications of hyaluronic acid fillers and the role of hyaluronidase in management. J. Plast. Reconstr. Aesthet. Surg. 2011, 64, 1590–1595.
- Weigel, J.A.; Weigel, P.H. Characterization of the recombinant rat 175-kDa hyaluronan receptor for endocytosis (HARE). J. Biol. Chem. 2003, 278, 42802–42811.
- Yoshida, H.; Okada, Y. Role of HYBID (hyaluronan binding protein involved in hyaluronan depolymerization), Alias KIAA1199/CEMIP, in hyaluronan degradation in normal and photoaged skin. Int. J. Mol. Sci. 2019, 20, 5804.
- Mikulic, M.U.S. Hyaluronic acid raw material market size 2014–2024, by application Hyaluronic acid raw material market size in the U.S from 2014 to 2024, by application. Statista 2018, 212, 1–2.
- Huerta-Ángeles, G.; Nešporová, K.; Ambrožová, G.; Kubala, L.; Velebný, V. An effective translation: The development of hyaluronan-based medical products from the physicochemical, and preclinical aspects. Front. Bioeng. Biotechnol. 2018, 6, 62.
- Liu, L.; Liu, Y.; Li, J.; Du, G.; Chen, J. Microbial production of hyaluronic acid: Current state, challenges, and perspectives. Microb. Cell Fact. 2011, 10, 99.
- Ucm, R.; Aem, M.; Lhb, Z.; Kumar, V.; Taherzadeh, M.J.; Garlapati, V.K.; Chandel, A.K. Comprehensive review on biotechnological production of hyaluronic acid: Status, innovation, market and applications. Bioengineered 2022, 13, 9645–9661.
- Widner, B.; Behr, R.; von Dollen, S.; Tang, M.; Heu, T.; Sloma, A.; Sternberg, D.; DeAngelis, P.L.; Weigel, P.H.; Brown, S. Hyaluronic acid production in Bacillus subtilis. Appl. Environ. Microbiol. 2005, 71, 3747–3752.
- Jing, W.; Deangelis, P.L. Dissection of the two transferase activities of the Pasteurella multocida hyaluronan synthase: Two active sites exist in one polypeptide. Glycobiology 2000, 10, 883–889.
- Jing, W.; Deangelis, P.L. Synchronized chemoenzymatic synthesis of monodisperse hyaluronan polymers. J. Biol. Chem. 2004, 279, 42345–42349.
- Ferreira, R.G.; Azzoni, A.R.; Santana, M.H.A.; Petrides, D. Technoeconomic analysis of a hyaluronic acid production process utilizing streptococcal fermentation. Processes 2021, 9, 241.
- Silverstein, S.M.; Greenbaum, S.; Stern, R. Hyaluronidase in ophthalmology. J. Appl. Res. 2012, 1, 12–13.
- Murray, G.; Convery, C.; Walker, L.; Davies, E. Guideline for the safe use of hyaluronidase in aesthetic medicine, including modified high-dose protocol. J. Clin. Aesthet. Dermatol. 2021, 14, 69–75.
- Murray, G.; Convery, C.; Walker, L.; Davies, E. Guideline for the management of hyaluronic acid filler-induced vascular occlusion. J. Clin. Aesthet. Dermatol. 2021, 14, 61–69.
- Walker, L.; Convery, C.; Davies, E.; Murray, G.; Croasdell, B. Consensus opinion for the management of soft tissue filler induced vision loss. J. Clin. Aesthet. Dermatol. 2021, 14, 84–94.
- Urdiales-Gálvez, F.; Delgado, N.E.; Figueiredo, V.; Lajo-Plaza, J.V.; Mira, M.; Moreno, A.; Ortíz-Martí, F.; Del Rio-Reyes, R.; Romero-Álvarez, N.; Del Cueto, S.R.; et al. Treatment of soft tissue filler complications: Expert consensus recommendations. Aesthet. Plast. Surg. 2018, 42, 498–510.
- Lima, V.G.F.; Regattieri, N.A.T.; Pompeu, M.F.; Costa, I.M.C. External vascular compression by hyaluronic acid filler documented with high-frequency ultrasound. J. Cosmet. Dermatol. 2019, 18, 1629–1631.
- Chang, S.-H.; Yousefi, S.; Qin, J.; Tarbet, K.; Dziennis, S.; Wang, R.; Chappell, M.C. External compression versus intravascular injection: A mechanistic animal model of filler-induced tissue ischemia. Ophthalmic Plast. Reconstr. Surg. 2016, 32, 261–266.
- Hwang, C.J.; Morgan, P.V.; Pimentel, A.; Sayre, J.W.; Goldberg, R.A.; Duckwiler, G. Rethinking the role of nitroglycerin ointment in ischemic vascular filler complications: An animal model with ICG imaging. Ophthalmic Plast. Reconstr. Surg. 2016, 32, 118–122.
- Rocha, P.S.; Guerra, T.A.; Teixeira, D.A. Description of a safe doppler ultrasound-guided technique for hyaluronic acid filler in the face-A method to avoid adverse vascular events. J. Cosmet. Dermatol. 2021, 21, 2783–2787.
- Wolferman, A.; Dwyer, F.P., Jr. Unilateral and bilateral ligation of the external carotid for epistaxis. AMA Arch. Otolaryngol. 1955, 62, 310–315.
- Hassard, A.D.; Kirkpatrick, D.A.; Wong, F.S. Ligation of the external carotid and anterior ethmoidal arteries for severe or unusual epistaxis resulting from facial fractures. Can. J. Surg. 1986, 29, 447–449.
- Cooke, E.T. An evaluation and clinical study of severe epistaxis treated by arterial ligation. J. Laryngol. Otol. 1985, 99, 745–749.
- Schelke, L.; Decates, T.; Kadouch, J.; Velthuis, P. Incidence of vascular obstruction after filler injections. Aesthet. Surg. J. 2020, 40, 457–460.
- Wollina, U.; Goldman, A. Facial vascular danger zones for filler injections. Dermatol. Ther. 2020, 3, 4285.
- Humzah, M.D.; Ataullah, S.; Chiang, C.; Malhotra, R.; Goldberg, R. The treatment of hyaluronic acid aesthetic interventional induced visual loss (AIIVL): A consensus on practical guidance. J. Cosmet. Dermatol. 2019, 18, 71–76.
- Cohen, J.L.; Biesman, B.S.; Dayan, S.H.; de Lorenzi, C.; Lambros, V.L.; Nestor, M.S.; Sadick, N.; Sykes, J. Treatment of hyaluronic acid filler-induced impending necrosis with hyaluronidase: Consensus recommendations. Aesthet. Surg. J. 2015, 35, 844–849.
- Hexsel, D.; Soirefmann, M.; Porto, M.D.; Siega, C.; Schilling-Souza, J.; Brum, C. Double-blind, randomized, controlled clinical trial to compare safety and efficacy of a metallic cannula with that of a standard needle for soft tissue augmentation of the nasolabial folds. Dermatol. Surg. 2012, 38, 207–214.
- van Loghem, J.A.J.; Humzah, D.; Kerscher, M. Cannula versus sharp needle for placement of soft tissue fillers: An observational cadaver study. Aesthet. Surg. J. 2017, 38, 73–88.
- Pavicic, T.; Frank, K.; Erlbacher, K.; Neuner, R.; Targosinski, S.; Schenck, T.; Gotkin, H.; Cotofana, S. Precision in dermal filling: A comparison between needle and cannula when using soft tissue fillers. J. Drugs. Dermatol. 2017, 16, 866–872.
- Jones, D.; Palm, M.; Cox, S.E.; McDermott, M.; Sartor, M.; Chawla, S. Safety and effectiveness of hyaluronic acid filler, VYC-20L, via cannula for cheek augmentation: A randomized, single-blind, controlled study. Dermatol. Surg. 2021, 47, 1590–1594.
- Alam, M.; Kakar, R.; Dover, J.S.; Harikumar, V.; Kang, B.Y.; Wan, H.T.; Poon, E.; Jones, D.H. Rates of vascular occlusion associated with using needles vs cannulas for filler injection. JAMA Dermatol. 2021, 157, 174–180.
- Ugradar, S.; Hoenig, J. Measurement of the force required by blunt-tipped microcannulas to perforate the facial artery. Ophthalmic Plast. Reconstr. Surg. 2019, 35, 444–446.
- Pavicic, T.; Webb, K.L.; Frank, K.; Gotkin, R.H.; Tamura, B.; Cotofana, S. Arterial wall penetration forces in needles versus cannulas. Plast. Reconstr. Surg. 2019, 143, 504–512.
- Ghassemi, A.; Prescher, A.; Riediger, D.; Axer, H. Anatomy of the SMAS revisited. Aesthet. Plast. Surg. 2003, 27, 258–264.
- Yang, Q.; Lu, B.; Guo, N.; Li, L.; Wang, Y.; Ma, X.; Su, Y. Fatal cerebral infarction and ophthalmic artery occlusion after nasal augmentation with hyaluronic acid—A case report and review of literature. Aesthet. Plast. Surg. 2020, 44, 543–548.
- Thanasarnaksorn, W.; Cotofana, S.; Rudolph, C.; Kraisak, P.; Chanasumon, N.; Suwanchinda, A. Severe vision loss caused by cosmetic filler augmentation: Case series with review of cause and therapy. J. Cosmet. Dermatol. 2018, 17, 712–718.
- Hu, X.Z.; Hu, J.Y.; Wu, P.S.; Yu, S.B.; Kikkawa, D.O.; Lu, W. Posterior ciliary artery occlusion caused by hyaluronic acid injections into the forehead: A case report. Medicine 2016, 95, e3124.
- Darling, M.D.; Peterson, J.D.; Fabi, S.G. Impending necrosis after injection of hyaluronic acid and calcium hydroxylapatite fillers: Report of 2 cases treated with hyperbaric oxygen therapy. Dermatol. Surg. 2014, 40, 1049–1052.
- Wibowo, A.; Kapoor, K.M.; Philipp-Dormston, W.G. Reversal of post-filler vision loss and skin ischaemia with high-dose pulsed hyaluronidase injections. Aesthet. Plast. Surg. 2019, 43, 1337–1344.
- Goodman, G.J.; Magnusson, M.R.; Callan, P.; Roberts, S.; Hart, S.; McDonald, C.B.; Liew, S.; Porter, C.; Corduff, N.; Clague, M. Neither positive nor negative aspiration before filler injection should be relied upon as a safety maneuver. Aesthet. Surg. J. 2021, 41, 134–136.
- Casabona, G. Blood aspiration test for cosmetic fillers to prevent accidental intravascular injection in the face. Dermatol. Surg. 2015, 41, 841–847.
- Goodman, G.J.; Magnusson, M.R.; Callan, P.; Roberts, S.; Hart, S.; Lin, F.; Rahman, E.; McDonald, C.B.; Liew, S.; Porter, C.; et al. Aspiration before tissue filler-an exercise in futility and unsafe practice. Aesthet. Surg. J. 2022, 42, 89–101.
- Kapoor, K.M.; Murthy, R.; Hart, S.L.A.; Cattin, T.A.; Nola, P.F.; Rossiter, A.P.; Singh, R.; Singh, S. Factors influencing pre-injection aspiration for hyaluronic acid fillers: A systematic literature review and meta-analysis. Dermatol. Ther. 2021, 34, e14360.
- Moon, H.-J.; Lee, W.; Kim, J.-S.; Yang, E.-J.; Sundaram, H. Aspiration revisited: Prospective evaluation of a physiologically pressurized model with animal correlation and broader applicability to filler complications. Aesthet. Surg. J. 2021, 41, 1073–1083.
- Schelke, L.W.; Decates, T.S.; Velthuis, P.J. Ultrasound to improve the safety of hyaluronic acid filler treatments. J. Cosmet. Dermatol. 2018, 17, 1019–1024.
- Lee, G.S.K. Use of handheld ultrasound Doppler to prevent complications from intra-arterial injection of dermal fillers: Clinical experience. J. Cosmet. Dermatol. 2019, 18, 1267–1270.
- Jagus, D.; Skrzypek, E.; Migda, B.; Wozniak, W.; Mlosek, R.K. Usefulness of Doppler sonography in aesthetic medicine. J. Ultrason. 2021, 20, 268–272.
- Lee, W.; Kim, J.-S.; Moon, H.-J.; Yang, E.-J. A safe doppler ultrasound-guided method for nasolabial fold correction with hyaluronic acid filler. Aesthet. Surg. J. 2021, 41, 486–492.
- Iwayama, T.; Hashikawa, K.; Osaki, T.; Yamashiro, K.; Horita, N.; Fukumoto, T. Ultrasonography-guided cannula method for hyaluronic acid filler injection with evaluation using laser speckle flowgraphy. Plast. Reconstr. Surg. Glob. Open 2018, 6, 1776.
- Quezada-Gaón, N.; Wortsman, X. Ultrasound-guided hyaluronidase injection in cosmetic complications. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 39–40.
- Munia, M.A.; Munia, C.G.; Parada, M.B.; Ben-Hurferraz Parente, J.; Wolosker, N. Doppler ultrasound in the management of vascular complications associated with hyaluronic acid dermal fillers. J. Clin. Aesthet. Dermatol. 2022, 15, 40–43.
- Levy, J.; Barrett, D.L.; Harris, N.; Jeong, J.J.; Yang, X.; Chen, S.C. High-frequency ultrasound in clinical dermatology: A review. Ultrasound J. 2021, 13, 24.
- DeLorenzi, C. New high dose pulsed hyaluronidase protocol for hyaluronic acid filler vascular adverse events. Aesthet. Surg. J. 2017, 37, 814–825.
- Paul, S.; Hoey, M.; Egbert, J. Pressure measurements during injection of corticosteroids: In vivo studies. Med. Biol. Eng. Comput. 1999, 37, 645–651.
- Cho, K.-H.; Pozza, E.D.; Toth, G.; Gharb, B.B.; Zins, J.E. Pathophysiology study of filler-induced blindness. Aesthet. Surg. J. 2019, 39, 96–106.
- Townsend, J.M.; Beck, E.C.; Gehrke, S.H.; Berkland, C.J.; Detamore, M.S. Flow behavior prior to crosslinking: The need for precursor rheology for placement of hydrogels in medical applications and for 3D bioprinting. Prog. Polym. Sci. 2019, 91, 126–140.
- Lee, Y.; Oh, S.M.; Lee, W.; Yang, E.J. Comparison of hyaluronic acid filler ejection pressure with injection force for safe filler injection. J. Cosmet. Dermatol. 2021, 20, 1551–1556.
- Nie, F.; Xie, H.; Wang, G.; An, Y. Risk Comparison of filler embolism between polymethyl methacrylate (PMMA) and hyaluronic acid (HA). Aesthet. Plast. Surg. 2019, 43, 853–860.
- Koziej, M.; Polak, J.; Wnuk, J.; Trybus, M.; Walocha, J.; Chrapusta, A.; Brzegowy, P.; Mizia, E.; Popiela, T.; Hołda, M. The transverse facial artery anatomy: Implications for plastic surgery procedures. PLoS ONE 2019, 14, 0211974.
- Lee, S.-H.; Ha, T.-J.; Koh, K.-S.; Song, W.-C. External and internal diameters of the facial artery relevant to intravascular filler injection. Plast. Reconstr. Surg. 2019, 143, 1031–1037.
- Kim, B.S.; Jung, Y.J.; Chang, C.H.; Choi, B.Y. The anatomy of the superficial temporal artery in adult koreans using 3-dimensional computed tomographic angiogram: Clinical research. J. Cerebrovasc. Endovasc. Neurosurg. 2013, 15, 145–151.
- Phumyoo, T.; Jiirasutat, N.; Jitaree, B.; Rungsawang, C.; Uruwan, S.; Tansatit, T. Anatomical and ultrasonography-based investigation to localize the arteries on the central forehead region during the glabellar augmentation procedure. Clin. Anat. 2020, 33, 370–382.
- Money, S.M.; Wall, W.B.; Davis, L.S.; Edmondson, A.C. Lumen diameter and associated anatomy of the superior labial artery with a clinical application to dermal filler injection. Dermatol. Surg. 2020, 46, 678–684.
- Khan, T.T.; Colon-Acevedo, B.; Mettu, P.; DeLorenzi, C.; Woodward, J.A. An anatomical analysis of the supratrochlear artery: Considerations in facial filler injections and preventing vision loss. Aesthet. Surg. J. 2017, 37, 203–208.
- Edsman, K.L.M.; Öhrlund, Å. Cohesion of hyaluronic acid fillers: Correlation between cohesion and other physicochemical properties. Dermatol. Surg. 2018, 44, 557–562.
- van Loghem, J.; Sattler, S.; Casabona, G.; Cotofana, S.; Fabi, S.G.; Goldie, K.; Gout, U.; Kerscher, M.; Lim, T.S.; de Sanctis Pecora, C.; et al. Consensus on the use of hyaluronic acid fillers from the cohesive polydensified matrix range: Best practice in specific facial indications. Clin. Cosmet. Investig. Dermatol. 2021, 14, 1175–1199.
- Goodman, G.J.; Liew, S.; Callan, P.; Hart, S. Facial aesthetic injections in clinical practice: Pretreatment and posttreatment consensus recommendations to minimise adverse outcomes. Australas. J. Dermatol. 2020, 61, 217–225.
- Chen, Y.; Zhang, Y.-L.; Luo, S.-K. Experimentally induced arterial embolism by hyaluronic acid injection: Clinicopathologic observations and treatment. Plast. Reconstr. Surg. 2019, 143, 1088–1097.
- Zhang, L.; Feng, X.; Shi, H.; Wu, W.T.L.; Wu, S. Blindness after facial filler injections: The role of extravascular hyaluronidase on intravascular hyaluronic acid embolism in the rabbit experimental model. Aesthet. Surg. J. 2020, 40, 319–326.
- Nie, F.; Xie, H. Effect of local massage on prevention and treatment of intra-arterial polymethyl methacrylate embolism complications: An experimental animal study. Chin. J. Plast. Reconstr. Surg. 2022, 4, 6–12.
- Taylor, G.I.; Shoukath, S.; Gascoigne, A.; Corlett, R.J.; Ashton, M.W. The functional anatomy of the ophthalmic angiosome and its implications in blindness as a complication of cosmetic facial filler procedures. Plast. Reconstr. Surg. 2020, 146, 745.
- Abduljabbar, M.H.; Basendwh, M.A. Complications of hyaluronic acid fillers and their managements. J. Derm. Derm. Surg. 2016, 20, 100–106.
- Park, H.J.; Jung, K.H.; Kim, S.Y.; Lee, J.H.; Jeong, J.Y.; Kim, J.H. Hyaluronic acid pulmonary embolism: A critical consequence of an illegal cosmetic vaginal procedure. Thorax 2010, 65, 360–361.
- Zhuang, Y.; Yang, M.; Liu, C. An islanded rabbit auricular skin flap model of hyaluronic acid injection-induced embolism. Aesthet. Plast. Surg. 2016, 40, 421–427.
- Taylor, G.I.; Palmer, J.H. The vascular territories (angiosomes) of the body: Experimental study and clinical applications. Br. J. Plast. Surg. 1987, 40, 113–141.
- Taylor, G.I.; Corlett, R.J.; Ashton, M.W. The functional angiosome: Clinical implications of the anatomical concept. Plast. Reconstr. Surg. 2017, 140, 721–733.
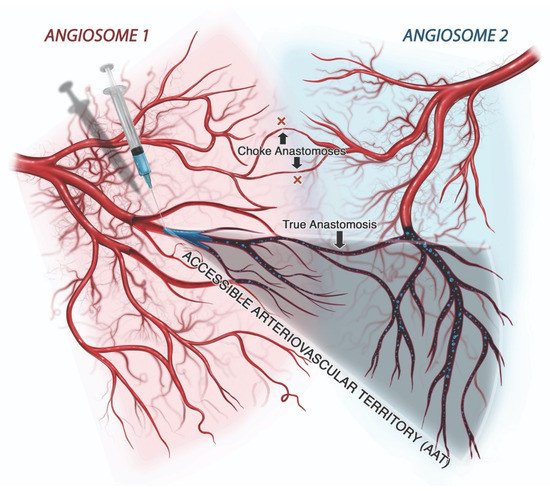
- Jajoria, H.; Venkataram, A.; Mysore, V. Importance of choke vessels in injectable fillers. J. Cutan. Aesthet. Surg. 2020, 13, 185–190.
- Gascoigne, A.C.; Taylor, G.I.; Corlett, R.J.; Briggs, C.; Ashton, M.W. Increasing perfusion pressure does not distend perforators or anastomoses but reveals arteriovenous shuntings. Plast. Reconstr. Surg. Glob. Open 2020, 8, e2857.
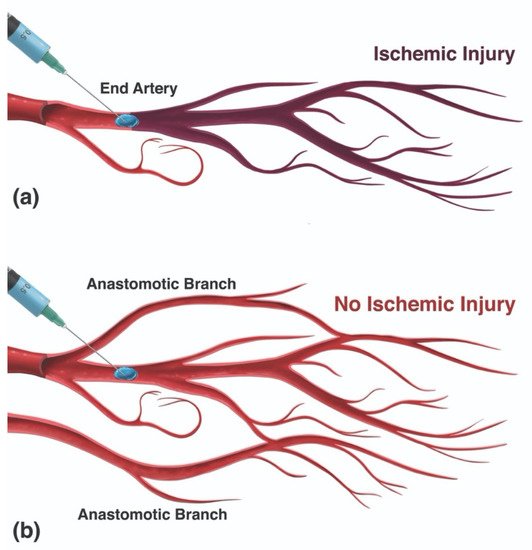
- Ashton, M.W.; Taylor, G.I.; Corlett, R.J. The role of anastomotic vessels in controlling tissue viability and defining tissue necrosis with special reference to complications following injection of hyaluronic acid fillers. Plast. Reconstr. Surg. 2018, 141, 818–830.
- Ogawa, R.; Oki, K.; Hyakusoku, H. Skin perforator freeways and pathways: Understanding the role of true and choke anastomoses between perforator angiosomes and their impact on skin flap planning and outcomes. Plast. Reconstr. Surg. 2014, 133, 719–720.
- Mao, Y.; Li, H.; Ding, M.; Hao, X.; Pan, J.; Tang, M.; Chen, S. Comparative study of choke vessel reconstruction with single and multiple perforator-based flaps on the murine back using delayed surgery. Ann. Plast. Surg. 2019, 82, 93–98.