Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Subjects:
Neurosciences
Apathy is a neurobehavioural symptom affecting Parkinson’s disease patients of all disease stages. Apathy seems to be associated with a specific underlying non-motor disease subtype and reflects dysfunction of separate neural networks with distinct neurotransmitter systems.
- Parkinson’s disease
- apathy
- neuropsychiatry
- neuropsychiatric symptoms in Parkinson's disease
- non-motor subtyping
- non-motor symptoms
1. Pathophysiology
1.1. Psychological Model
To understand the pathophysiology of apathy it is necessary to evaluate how apathy arises as a behavioural concept. Apathy is essentially the reduction of voluntary, goal-directed behaviour (GDB) [18]. The neuro-cognitive formulation of how GDB arises is convoluted, so we provide an abbreviated model based on Brown and Pluck’s theory (Figure 1) [67]. The process of GDB emerges from an interaction of internal and external drives, intention, planning, motivation, and emotional state. Theoretically, interference in any of these processes can lead to apathy [18,67].
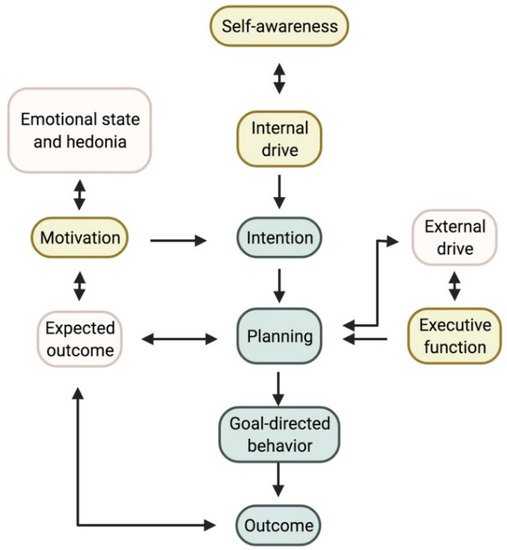
Figure 1. Proposed model for goal-directed behaviour. The three accepted subtypes and where they plug into the model are shown in yellow. Self-awareness, which is currently not yet considered a subtype, could interact with the internal drive and planning. Note on the left the importance of the hedonic state, which can affect those suffering from depression. Created with https://biorender.com/ (accessed on 27 June 2022).
Stuss and coworkers described three distinct subtypes of apathy. First, difficulties with self-activating thoughts or initiating the necessary motor functions for GDB are the predominant feature in the first type. We summarized this as a reduction of ‘internal drive’. This reduced internal drive and response starkly contrast the preserved reaction to external drives and stimuli [18,68]. In an everyday setting, these patients do little unless instructed [69,70]. Daily productivity is low and there is no variation in activities in daily life [49], resulting in severe inertia that can be reversed successfully with external stimuli [18]. This subtype of apathy is sometimes referred to as ‘behavioural apathy’; however since all forms of apathy lead to a reduction in GDB, we suggest an alternative terminology [71]. Aphrenic apathy, derived from the Greek word for ‘inability to think’, is a more apt description of this subtype.
A disruption in the planning aspect of GDB leads to ‘cognitive’ apathy or cognitive inertia. Faulty executive processing lies at the basis here, rendering difficulties with planning, working memory, rule-finding, and set-shifting [18]. The underlying executive dysfunction makes it difficult to plan the actions needed to perform GDB [18,67,68]. Executive dysfunction does not always reflect underlying dementia but may herald it [72]. This clinically manifests as a decreased interest, or more accurately, a decreased (intellectual) curiosity [69]. These patients spend little or no time on leisure activities and have few interests. Often, they do not wish to pursue (new) hobbies or social engagements. They quickly give up on a task when facing difficulties, reflecting their executive dysfunction [49,69].
A final subtype of apathy is an underlying reward deficiency syndrome, in which a patient cannot relate the GDB to the (pleasurable) outcome or reward. This is the result of emotional blunting or reduced emotional resonance [18,68,69]. This third subtype is often referred to as ‘motivational’ apathy [18,68]. It results in a reduced emotional response, for instance when the patient is confronted with upsetting news or watching something humorous. Patients can also display a decreased concern for their families and often no longer inquire after their health and well-being spontaneously [18,49].
It is necessary to differentiate this apathy subtype from the symptoms of an underlying depression or mood disorder. Apathy can also be related to anhedonia, resulting in decreased GDB [67,73]. Apathy in patients suffering from a depressive episode can improve with adequate treatment of their mood disorder [74].
Aside from these three widely accepted apathy subtypes, a fourth dimension called ‘self-awareness’ was initially proposed by Stuss and coworkers [68]. These authors described self-awareness as a critical component of GDB. They defined it as ‘[…] a metacognitive ability, necessary to mediate information from a personal, social past and current history with projections to the future […]’ [68]. The Lille Apathy Rating Scale (LARS) was developed with this fourth dimension in mind, reflected by a fourth and independent cluster in their data analysis, separate from depression [49]. The question remains whether reduced self-awareness can be considered an underlying mechanism of apathy or a different construct altogether [69]. Self-awareness in essence organizes an individual’s understanding of a social environment and the function of this individual within it [75]. Clinically, impaired self-awareness can manifest as anosognosia, or reduced insight into one’s own physical limitations due to an illness. Reduced self-awareness has often been described in Parkinson's disease (PD) patients and is associated with cognitive decline [76,77,78]. Clinically, this may manifest itself in social interactions, where the patient might be quite headstrong in an argument, unwilling to concede to another’s point of view. This results from a decrease in self-reflection, making it difficult to assess one’s own faults accurately [49].
1.2. Neural Networks
It is often assumed that apathy results from a pure hypodopaminergic state, as it often can arise following dopamine withdrawal for Deep Brain Stimulation (DBS) surgery. Dopaminergic treatment has shown improvement in some patients, but a more complex model is required to explain the implicated neurotransmitter systems [19]. Despite adequate dopaminergic treatment, apathy occurs in PD patients, and the severity of apathy is independent of medication dosage [39,79]. Apathy can co-occur in PD patients suffering from impulse control disorders related to a hyperdopaminergic state [80,81]. Co-occurrence of apathy and impulse disorders was also reported in other neurological disorders [82]. Lastly, animal models and imaging studies in patients have shown the involvement of other neurotransmitter systems [83,84,85]. To further study the complex underlying physiology of apathy, the definition of the neuroanatomical correlates is an important starting point. Generally, the occurrence of apathy can be reduced to a dysfunctional circuitry between the frontal lobes and the basal ganglia. Within this circuitry, separate networks can be identified (see Figure 2) [68,86,87].
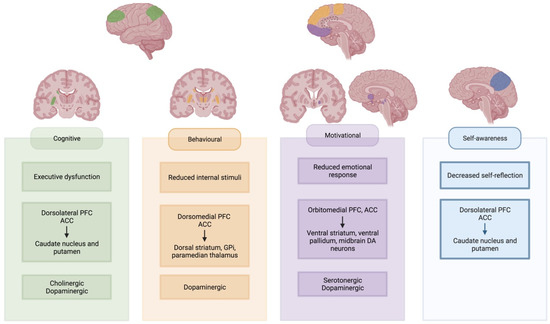
Figure 2. Neural networks underlying apathy subtypes. Involved cortical regions and basal ganglia regions are highlighted for each subtype. Created with https://biorender.com/ (accessed on 27 June 2022). Abbreviations: PFC: prefrontal cortex; ACC: anterior cingulate cortex; Gpi: internal globus pallidus; DA: dopaminergic.
‘Behavioural’ or ‘aphrenic’ apathy is often equated to a lack of initiation or internal drive to perform the GDB [18,68]. It is often referred to as an auto-activation deficit, with a reduced response to internal stimuli [18]. This type of apathy is often considered the most severe form. It has been described in bilateral dysfunction of the pathway between the dorsomedial prefrontal cortex (dmPFC) and anterior cingulate cortex (ACC) with the dorsal striatum, paramedian thalamus and the internal part of the globus pallidus (GPi) [88,89,90,91,92,93,94,95,96]. Similar syndromes have been described in uni- or bilateral lesions of the supplementary motor area (SMA) [70]. These are regions of interest in the ‘lateral orbitofrontal cortex’ circuit as described by Garrett and colleagues, which also receives input from temporal gryi and projects to the substantia nigra pars reticulata [87]. This circuit is partially dopamine-mediated, as evidenced by reduced dopaminergic binding and response to DRT [88,89,92,97].
Executive dysfunction leads to ‘cognitive’ apathy, where planning difficulties interfere with GDB. The dorsolateral PFC, cooperating with the ACC, is vital to executive processing, resulting in apathetic behaviour when lesioned [18,87,98,99]. This region has projections to the lateral parts of the dorsal striatum [87,92,100,101,102]. The lateral dorsal striatum also receives input from the posterior parietal cortex [87]. Cognitive apathy has been linked to decreased functional connectivity (FC) between the orbitofrontal cortex (OFC) and the right putamen [103]. We assume that the ‘dorsolateral PFC’ circuit is largely acetylcholine-mediated due to its implication in executive dysfunction [104]. In Alzheimer’s disease patients with predominant cognitive apathy, there was reduced response to dextroamphetamine administration, suggesting some possible dopaminergic involvement as well [105].
‘Motivational’ apathy is mediated by the mesocorticolimbic pathway or the reward system [18,68,106]. Involved regions are the orbitomedial PFC, the ACC, the ventral striatum, the ventral pallidum and the dopaminergic midbrain neurons [18,107]. This system is mediated by the amygdala, hippocampus, thalamus, lateral habenular nucleus, the dorsal PFC, as well as the pedunculopontine nucleus and raphe nucleus in the brainstem [107,108]. Patients with ‘motivational’ apathy according to the LARS showed altered FC between the left inferior frontal gyrus and the left pallidum. There was an increased FC between the left inferior frontal gyrus and the right caudate [103]. Apathetic PD patients showed selective impairment of reward processing, reducing their ability to differentiate between favourable and unfavourable outcomes [109]. Dopamine plays an important role in this circuit, yet its relation to manifest apathy is complex [110]. Administration of dopamine agonists blunts reward sensitivity in healthy adults, while use in apathetic patients shows promise as a potential therapy [111,112]. Yet, some studies found no difference in dopaminergic uptake between apathetic and non-apathetic patients [84]. Serotonin could act as a modulator, with reduced uptake found in critical parts of the mesocorticolimbic pathway in apathetic PD patients [84,85]. The uptake reduction was proportional to apathy’s severity [84]. Reduced serotonergic uptake in the raphe nucleus was also associated with the presence and severity of apathy in possible prodromal PD patients [113].
In our abbreviated and modified model in Figure 1, we propose a new role for self-awareness in developing GDB. Recent imaging findings have identified common underlying brain regions and networks in patients with reduced self-awareness and apathy. The precuneus is part of the default-mode network and plays an important role in self-awareness [114,115,116]. Studies found that isolated apathy in PD was associated with atrophy and hypometabolism of the precuneus compared to healthy controls [117,118]. Other regions of interest in self-awareness are the ACC, the posterior cingulate cortex (PCC), the temporoparietal junction, the ventromedial and dorsolateral prefrontal cortex and the insula [119,120,121].
It is unlikely that a different type of apathy develops in each patient. Patients with typical auto-activation deficit lesions were also shown to have reduced reward sensitivity [97,122]. One study found that apathy profiles differed, depending on disease stage. In stable PD patients, defined by the authors as well-controlled motor symptoms without fluctuations and absence of dementia, there was a trend towards decreased intellectual curiosity or ‘cognitive’ apathy. In PD patients with motor fluctuations without dementia, mostly intellectual curiosity and action initiation were inhibited. In PDD, both domains as well as self-awareness were decreased. Interestingly, in all groups, motivational apathy, as measured by the emotion subscore of the LARS, did not differ significantly from healthy controls [13]. Another study found a predominant decrease in intellectual curiosity in early-stage PD patients [4]. These findings suggest that apathy subtypes might have a distinct temporal profile.
1.3. Imaging Biomarkers
Aside from neurotransmitter changes in different networks, additional imaging biomarkers of apathy have been investigated. Changes have been reported in grey-matter volume (GMV), white and grey matter integrity, FC and network analysis, regional homogeneity (ReHo), glucose metabolism, and resting activity pattern.
Decrease in GMV in the subgenual AAC, left superior temporal, left precuneus, inferior parietal, right superior frontal, and the dorsolateral part of the caput of the left caudate nucleus is related to the presence of apathy. Severity of apathy was related to morphological abnormalities in the superior cerebellar peduncle decussation, bilateral posterior cerebellum and vermis, left superior frontal gyrus, and left nucleus accumbens [84,117,123]. GMV increases were noted in the left superior frontal gyrus and cerebellar vermis [117]. Other imaging studies, however, could not confirm these changes [86,124,125]. The connectivity between the parietal cortex and frontal lobes might explain part of these findings, as frontal lesions lead to parietal hyperactivity [116]. Input of temporal gyri has also been described in the ‘lateral orbitofrontal cortex’ circuit of the basal ganglia, implicated in ‘behavioural’ apathy [87].
Fractional anisotropy (FA) was significantly decreased in the genu and body of the corpus callosum, bilaterally in the anterior corona radiata and the left superior part of the corona radiata and left cingulum in apathetic PD patients. The grade of integrity was related to apathy severity [126]. Another study found reduced FA in the anterior thalamic fibres, the cingulate bundle, and the corpus callosum’s interhemispheric connections and projection fibres. FA was also decreased bilaterally in the medial thalamus [84].
FC was reduced between the left ventral striatum and left frontal lobe in apathetic PD patients. Reduced FC between ventral and dorsal striatum and left frontal lobe, between the limbic region of the left frontal lobe and left striatum, between the caudal and rostral frontal lobe and right striatum and in between subdivisions of the left frontal lobe was related to increased severity of apathy [86] A regional network analysis could not find differences in connectivity between apathetic and non-apathetic PD patients [124].
Analysis of low-frequency function (ALFF), which evaluates the resting state of the entire brain, showed decreased ALFF signal in the left supplementary motor region, left inferior parietal love, left fusiform gyrus, and bilaterally in the cerebellum [127].
ReHo measures synchronization of local neural activity. In apathetic PD patients, ReHo was decreased in right caudate and dorsal ACC [128]. Some studies found reduced glucose metabolism in the precuneus bilaterally and right lingual gyrus and increased metabolism in the middle frontal gyrus in apathetic patients [117]. Additionally, the severity of white matter hyperintensities on FLAIR sequence also showed a link to apathy in PD, independent of depression [129]. These findings suggest top-down control from other cortical regions and support the involvement of the parietal cortex in certain subtypes [87,116].
2. Treatment
2.1. Pharmacological
As discussed above, many neurotransmitters are involved in the underlying process of apathy. Evidence has been found of dopaminergic, serotonergic, and cholinergic involvement in PD. [79,83,88,89,92,97].
Use of dopamine replacement therapy (DRT) has shown promising results, and administration of dopamine agonists is often most successful. A recent meta-analysis concluded that using rotigotine improved apathy scores, which was not confirmed in a more recent placebo-controlled study [147,148]. Other dopamine agonists such as pramipexole or apomorphine might also be beneficial, as patients score better on the items ‘intellectual curiosity’ and ‘self-awareness’ after administration [112,149]. Global apathy scores improved in those receiving apomorphine when combined with rotigotine [149,150]. Rotigotine and pramipexol were effective in reversing an auto-activation deficit in a case series [151].
DRT is assumed to improve apathy in the long term, as evidenced by the decreasing prevalence after the introduction of medication [23]. Apathy scores do not differ significantly in ON or OFF stages, showing no significant response to DRT in the acute phase [152]. No studies comparing different DRT strategies in these patients are available.
Results on serotonergic treatment are scarce. Selective serotonin receptor inhibitors are known to induce flat affect and apathy, both in healthy individuals and PD patients [153]. A cross-over study in 25 PD subjects with 5-hydroxytryptophan, a precursor of serotonin, had no significant impact on apathy scores [154]. Use of both selective serotonin and serotonin noradrenaline reuptake inhibitors (SSRI and SNRI respectively) did not significantly alter apathy scores compared to baselines [155].
In those already receiving optimized dopaminergic treatment without PDD, add-on of rivastigmine improved apathy scores [79]. Although rivastigmine was reported to improve apathy in PDD in a few case reports, a more extensive patient series showed no improvement in this group [104,156]. Use of rivastigmine decreased caregiver distress associated with apathy [157]. Galantamine might be effective in apathetic PDD patients [158].
Other strategies include the use of stimulants. Administration of dextroamphetamine in a PD sample with cognitive decline improved apathy scores in nearly a third of patients. Most of these patients were already receiving cholinesterase inhibitors [159]. Singular positive reports have been published on the use of methylphenidate, istradefylline, MAO inhibitors, yokukansan, and exenatide [160,161,162,163,164,165]. Bupropion and choline alphoscerate, a cholinergic precursor, was shown to be effective in treating apathy in other neurodegenerative diseases [166,167,168]. A case report of a patient suffering from an auto-activation deficit reported spectacular improvement of symptoms following administration of tricyclic antidepressants [169].
2.2. Non-Pharmacological
Non-pharmacological treatment options have garnered increasing interest. Exercise especially is beneficial in the treatment of both motor and NMS [170,171]. For the treatment of apathy, exercise and physical activity may also prove useful. A longitudinal study found that patients with baseline higher activity levels had improved apathy scores at follow-up. Apathy scores at baseline were not related to activity level [172]. Others however found very little difference between those following an intensive exercise schedule with sessions thrice a week and those without intervention. Only those following individual therapy showed slight improvement [173]. Apathy scores did improve in patients following biweekly Nordic walking sessions over 12 weeks, compared to control patients [174]. Though there is some evidence for a positive effect of dance, a recent meta-analysis concluded it was not superior to self-directed exercise or the best medical treatment [175,176]. There is need for structured research into the matter, wherein different physical activities and interventions are systematically researched and compared. As current evidence does not support one type of physical activity above another, it is advised to tailor the type of physical exercise to the patients’ needs and preferences [177].
A small body of evidence exists for using repetitive transcranial magnetic stimulation (rTMS). A cross-over study found that rTMS over the supplementary motor area improved apathy scores compared to placebo [178]. Stimulation of the M1 area in the precentral gyrus showed similar improvement [179]. Benefit was also found after targeting the dorsolateral PFC, after which both apathy and emotional processing improved [180]. Cognitive rehabilitation is beneficial in treating apathy in the healthy elderly, but no such benefits were observed in PD patients [181,182,183]. A pilot project showed slight benefits in the short term, but longitudinal data is not available [184].
This entry is adapted from the peer-reviewed paper 10.3390/brainsci12070923
This entry is offline, you can click here to edit this entry!