2. The Role of Imaging in Stereotactic Body Radiotherapy (SBRT)
Radiotherapy is one of the definitive local treatment options for MSCC and includes cEBRT and SBRT. SBRT is technically feasible in low-grade MSCC (up to Bilsky 1c) [
105] and is mainly indicated in the setting of oligometastatic disease, re-irradiation, and in the treatment of radioresistant primary tumors where durable local control and symptom relief are required [
106].
SBRT is a high-precision technique that relies on the accurate anatomical delineation of the tumour and adjacent critical structures to deliver highly conformal ablative doses while minimizing radiation to the surrounding organs at risk due to a steep dose gradient. This is achieved with highly precise and accurate image guidance in both SBRT planning and delivery [
12,
107,
108,
109,
110].
The delivery of higher dose per fraction enables a shorter treatment time and allows the effective treatment of tumours previously considered radioresistant to cEBRT [
12,
17,
107,
111,
112]. The effectiveness of SBRT in local tumour and symptom relief has been widely studied with favourable results [
98,
111,
112,
113,
114,
115,
116]. A systemic review by Gerszten et al. showed that SBRT can achieve local control rates of approximately 90% and pain improvement rates of 85% [
107], superior to that of cEBRT.
The role of imaging in SBRT lies in three main areas:
2.1. Pre-Treatment Planning
The Spine response assessment in Neuro-Oncology (SPINO) group recommends performing a high-resolution CT with slice thickness ≤ 2 mm for SBRT planning [
98]. This allows depiction of bony structures with good spatial accuracy, metastatic lesion characterization and assessment of electron density of tissues. Due to the inferior soft tissue resolution in CT, there can be limited information on the tumour extent (particularly in the para-spinal and epidural areas). Moreover, accurate segmentation of the spinal cord is critical for SBRT, and limiting the cord dose is prioritized during SBRT planning. The SPINO group therefore recommends performing volumetric thin slice (≤3 mm) axial T1-weighted pre- and post-contrast and T2-weighted MRI close to the date of CT-simulation (ideally, within 1 week of simulation) [
98].
Isotropic volumetric MRI acquisitions enable multiplanar reconstructions to facilitate co-registration between the MRI and CT (
Figure 9) [
117]. Whenever possible, the treatment position should be replicated during the time of planning MRI, so as to facilitate accurate co-registration. Despite these measures, perfect co-registration is usually not achieved, due to spatial distortion artifacts commonly encountered in MRI [
118,
119].
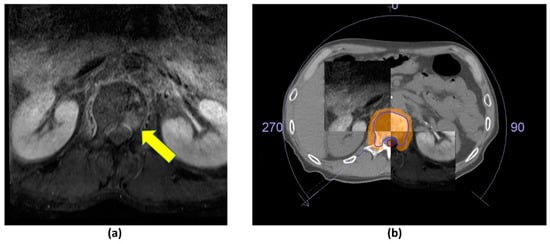
Figure 9. Axial post-contrast fat-suppressed T1-weighted MRI. (a) Metastatic lesion in the L1 vertebral body (yellow arrow). (b) CT and MR fusion for stereotactic body radiotherapy (SBRT) planning; 27 Gy over 3 fractions delivered using volumetric modulated arc therapy. Clinical target volume (CTV—blue outline), planning organ at risk volume (PRV, cord—red outline), 95% isodose (orange colour wash).
Rogé et al. (2022) recently demonstrated that semi-automated clinical target volume (CTV) generation for SBRT planning of spinal metastasis had favourable accuracy when compared to manual contouring, and did not show a significant dosimetric increase to the organs at risk [
120]. It is anticipated that future research would focus on the automation of tumour contouring, an otherwise laborious task if performed manually [
121].
2.2. Image-Guided Radiotherapy (IGRT)
Image-guided radiation therapy (IGRT) for SBRT requires three-dimensional positional verification of the treatment isocentre prior to SBRT delivery. There are several points where anatomic or positional deviation may occur in radiation therapy, affecting the precision and accuracy of dose delivery. Daily set-up errors and deviations between the patient anatomy at pre-treatment planning and at the treatment itself (e.g., tumour growth, patient weight loss) are referred to as interfractional variation. Movement occurring in the course of a treatment session (e.g., patient motion and inherent cord motion secondary to the cardio-respiratory cycle) is referred to as intrafractional movement [
117,
122,
123]. Inherent cord motion may account for up to 0.7 mm in the axial direction [
124].
Failure to account for inter- and intrafractional motion can lead to adverse effects including underdosing the target volume, and/or harmful dose delivery to adjacent radiosensitive organs [
122]. This is particularly important in SBRT treatment for less severe MSCC (e.g., Bilsky grade 1c), where the spinal cord lies in close proximity. Intrafractional movement may be increased in treatments lasting more than 20 min [
125]. In such cases, our group recommends a mid-treatment CBCT to verify and correct for the treatment isocentre. A study by Oztek et al. (2020) had previously recommended a planning organ at risk volume (PRV) margin of at least 1.5–2 mm around the spinal cord to account for intrafractional cord motion [
126].
IGRT for SBRT is predominantly performed through an onboard kilovoltage cone-beam CT. This allows for sub-millimeter spatial resolution, and modern radiotherapy treatment couches are able to correct for any deviations in the treatment isocentre, along the translational and rotational axes, i.e., 6D correction [
127,
128,
129].
In CBCT, a cone-shaped X-ray beam is used with reciprocal two-dimensional area detectors instead of the collimated fan-shaped X-ray beam with the one-dimensional linear group of detectors that is used in conventional diagnostic CT. This enables volumetric acquisition with just a single rotation of the gantry without patient motion, compared to the helical acquisition of data seen in conventional CT imaging. The resultant three-dimensional volumetric data set can be reconstructed in all three orthogonal planes and is compared to the planning CT to calculate and correct for changes in target position prior to each radiation session [
127,
128]. It has to be noted that the time required for on-board CBCT acquisition (approximately 3–5 min) is considerably longer than conventional diagnostic CT. This limitation is predominantly due to the speed of gantry rotation.
Compared to conventional CT, CBCT has a reduced radiation dose [
128,
130]. However, there is increased scatter, beam hardening and other artifacts, causing a grainy and nonuniform appearance of the image [
127,
131,
132,
133,
134]. These result in reduced soft tissue contrast and CT number accuracy [
131,
132,
133]. Several strategies have been employed to overcome the artifacts in CBCT. For example, Bowtie filters and correction software have been employed to overcome beam hardening artifacts, motion artifacts have been reduced by patient immobilization and instruction to keep still, and other reconstruction and post-processing algorithms have been developed to tackle various other artifacts to improve image quality [
127,
133,
134]. Preliminary research has also explored the role of dual-energy CBCT in overcoming these artifacts [
132].
Other advanced imaging strategies in IGRT employ the use of onboard MR imaging, for example, Co60 MRI-guided radiotherapy and the more recent MRI-guided linear accelerator (MRI-LINAC) [
135,
136]. Unlike two-dimensional planar imaging and CBCT, MR-guided radiotherapy does not contribute to radiation dose. It also has the added benefit of being the imaging-of-choice for MSCC. Due to its superior soft tissue contrast, there are reduced safety margin requirements [
137,
138]. Other advantages include the ability of MRI to provide functional information on the tumour during the course of SBRT (e.g., apparent diffusion coefficient hypointensity as a marker of cellularity from high mitotic rate) [
137]. Processes to do away with the mandatory CT simulation are being explored, by using MRI data to estimate the electron density for dose calculation [
137,
139].
Importantly, MRI has the potential to achieve real-time image guidance of the spinal cord in MSCC patients [
135,
136]. This allows detection of intrafractional motion. Treatment can then be halted almost instantly for patient repositioning, which had been previously shown to correlate with positional changes of the spinal cord in the vertebral canal [
140]. Previous methods to control intrafractional variation have mostly relied on periodic mid-treatment imaging [
125,
141]. Another strategy to mitigate intrafractional motion employs the use of flattening filter free (FFF) SBRT to improve the dose rate and thereby reduce treatment time [
142].
2.3. Post-Treatment Follow-Up
The SPINO group recommends performing an MRI of the spine 2–3 months after SBRT, with an interval MRI every 8–12 weeks thereafter to assess response to treatment. The studies should be reviewed by a radiologist and radiation oncologist. Earlier imaging may be warranted if the patient develops new neurological deficits or increasing pain [
98].
Local control is defined by a lack of disease progression within the treated region (
Figure 10). This should be observed on two or three consecutive MRI studies that are performed 6–8 weeks apart. Local progression has several definitions. These include a definite expansion in tumour volume or increase in linear measurement, new epidural lesions and the presence of neurological deterioration with borderline increased extent of epidural disease on MRI [
98].
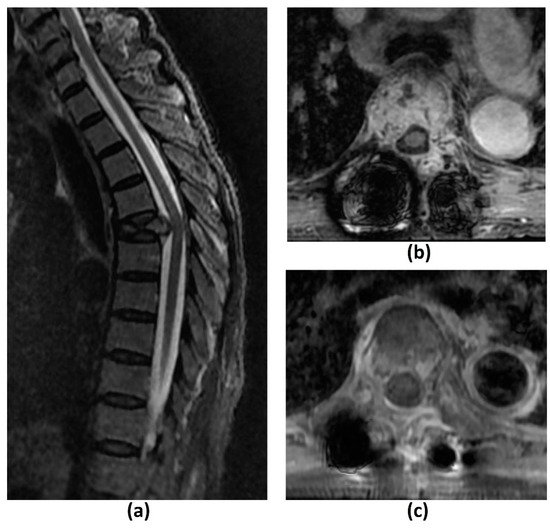
Figure 10. Sagittal T2-weighted image (a) of a 69-year-old female patient with metastatic rectal cancer to the spine shows a pathological T5 vertebral fracture. Axial post-contrast fat-suppressed T1-weighted images of the same patient, post separation surgery and planning for stereotactic body radiotherapy (SBRT) (b), and 6 months post-treatment (c). There is reduced tumour enhancement and bulk between (b) and (c) due to favourable post-SBRT response.
Volumetric changes are a standard indicator of treatment efficacy of spinal lesions [
117,
143]. However, this may not be seen uniformly, even in patients who respond to SBRT. There is limited literature on the MRI appearances of bone metastasis post SBRT and it is still uncertain which signal changes are associated with treatment response or failure [
98]. Hwang et al. (2011) studied changes in signal intensity of osteoblastic lesions post stereotactic radiosurgery, as these lesions normally show no volumetric changes during remission. Indicators of local control were shown to be increased T2-weighted signal intensities intermixed with areas of T2-weighted hypointensities [
143]. This contrasts with another study by Zhou et al. (2014), which found that increased T2-weighted signal intensity was a predictor of local failure [
144]. It should be noted that these studies had small sample sizes and further research is required.
The feasibility of functional imaging techniques (e.g., DCE MRI, diffusion-weighted MRI and PET/CT) in assessing treatment response of spinal metastasis post SBRT have also been studied. Kumar et al. (2017) showed that an increase in plasma volume on DCE MRI from pre- to post-radiotherapy was associated with local recurrence and a cut-off of −20% could predict local recurrence with high sensitivity and specificity. These changes were able to detect local recurrence up to 18 months earlier than conventional MRI [
145]. The findings concur with a retrospective study by Chu et al. (2013), which also showed that reduction in plasma volume was the strongest predictor of treatment response [
146]. Regarding DWI, Lee et al. (2021) found that the percentage change in ADC pre- and post-radiotherapy for bone metastasis from hepatocellular carcinoma was closely related to local tumour progression with a lower value predicting progressive disease [
147]. Similarly, another study by Byun et al. (2002) showed that decreased DWI signal intensity of the bone marrow within metastatic spinal disease was indicative of successful radiation therapy [
148]. Regarding PET/CT imaging, a preliminary study by Gwak et al. (2006) involving three patients with recurrent spinal metastasis treated with radiotherapy found that changes in SUV on 18F-FDG PET/CT correlated with clinical outcomes [
102]. More recently, Choi et al. (2018) noted that >70% reduction in maximum SUV post SBRT in 42 patients with spinal metastasis who underwent 18F-FDG PET/CT before and after treatment was predictive of good progression-free-survival [
149]. It should be noted however, that there is a possibility of a flare response post SBRT with variable increased radiotracer uptake that may persist up to 6 months [
150]. While further research is needed to validate these findings, they suggest that post SBRT follow-up imaging may require a combination of functional and structural MRI for greater diagnostic accuracy.
Assessing for progression or regression in paraspinal and epidural disease is more straightforward. The former requires a definite change in volume and/or linear measurements, while the latter utilizes grading with the Bilsky criteria [
21,
98]. It should be noted that the most frequent site of disease progression post SBRT is the epidural space. This is due to planning criteria to limit the dose received by the spinal cord, and consequently underdosing the tumour abutting the spinal cord [
98].
The role of CT in post SBRT follow-up imaging is complementary to MRI. It can assess the integrity of cortical bone, which can be affected by SBRT [
98,
117].
A common pitfall in post SBRT imaging is the phenomenon of pseudoprogression. This occurs when there is a significant increase in post-treatment lesion volume usually without significant clinical symptoms, with eventual stabilization or regression on subsequent imaging [
117,
151]. This is well documented in the brain, lung and liver [
117]. These can be confused with true disease progression particularly if the patient experiences a pain flare, which reportedly affects 10–68% of patients post SBRT [
152,
153]. A biopsy may be warranted for a definitive diagnosis in such cases [
98].
Pseudoprogression reportedly occurs in 14–18% of cases after spine SBRT [
154,
155]. A retrospective review by Bahig et al. (2016) found that pseudoprogression tended to be confined within the vertebral body while true local recurrences often involved the epidural space [
155]. However, more research may be needed as a recent case report demonstrated a patient with pseudoprogression in the form of an epidural mass [
156]. The timeframe is also important, with pseudoprogression occurring within a few weeks up to 6 months post SBRT, in contrast to the late presentation of radio-necrosis which may occur years after therapy [
151]. Growth confined within the 80% prescription isodose-line and lytic lesions (as opposed to sclerotic lesions) have also been shown to be predictive of pseudoprogression [
155,
157].
VCF is a commonly encountered complication of SBRT [
151]. The incidence rate of VCF ranges from 11–39%, with a systematic literature review by Faruqi et al. (2018) reporting a crude rate of 13.9% [
158,
159,
160]. There is a median time of 2.6 months to VCF excluding outliers [
158], as late-onset VCF of 2–3 years post SBRT have also been seen [
161].
Both MRI and CT have limited ability to ascertain if a VCF was induced by SBRT or related to local tumour progression [
162]. The SPINO group recommends histological confirmation in uncertain cases [
98]. Al-Omair et al. (2013) had previously reported two patients who underwent spine SBRT, and subsequently developed imaging findings concerning for local tumour progression and VCF. However, biopsy eventually showed radiation-induced changes in the bone without evidence of tumour progression [
161].
There are currently no established guidelines on the use of advanced imaging techniques/functional imaging like PET/CT or DCE MRI to distinguish between the two processes. While several studies have proposed a role of PET/CT in distinguishing benign and malignant compression fractures, these generally were not performed in the post-SBRT setting. Radiation-induced inflammatory changes may result in variably increased uptake on PET/CT in the immediate 6 months post SBRT and limit its diagnostic utility in such settings [
150,
162]. On perfusion/DCE MRI, vertebral metastases with or without associated pathological fracture were noted to demonstrate a significantly steeper enhancement slope and greater peak enhancement percentage than chronic compression fractures in a previous study involving 42 patients by Chen et al. (2002). However, no significant difference was found with acute compression fractures [
163]. Further research into the role of functional imaging in evaluating VCF post SBRT is warranted, given the potential morbidity associated with salvage therapies. Future research may also focus on tools that predict the risk of VCF post SBRT treatment, so that prophylactic measures may be instituted. For example, Gui et al. (2021) had recently shown the feasibility of using the patient’s clinical information and radiomic features of the patient’s pretreatment imaging to develop a model that predicts the risk of VCF one year post SBRT treatment [
164].
3. Summary
MSCC is a debilitating complication in cancer patients with spinal metastasis, and its incidence is expected to rise due to improving cancer treatments and survival. Radiotherapy, including cEBRT and SBRT, constitutes one of the major treatment arms of MSCC. Imaging plays an important role in SBRT for pre-treatment planning, in-room image-guidance, and post-treatment follow-up. Recommendations from the SPINO group have been made on the definitions of local progression and local control post SBRT. However, there remain inherent difficulties in determining treatment response due to factors like pseudoprogression, and the uncertainty in signal changes indicating treatment response in bone metastasis. Functional MRI may help in the latter.
VCF is the most common complication post SBRT, and may be related to local tumour progression or the SBRT treatment itself. Current imaging modalities like MRI and CT have limited ability to distinguish between these two processes, and further research into the role of functional imaging in evaluating VCF post SBRT is warranted.