Sjögren’s syndrome (SS) is a systemic chronic autoimmune disorder characterized by lymphoplasmacytic infiltration of salivary glands (SGs) and lacrimal glands, causing glandular damage. The disease shows a combination of dryness symptoms found in the oral cavity, pharynx, larynx, and vagina, representing a systemic disease. The following content reports the data present in the literature relating to organ fibrosis correlated with SS. The phenomenon has been extensively studied in SGs, where the molecular mechanisms that could trigger fibrosis are known and have been correlated with EMT. Cases of secondary fibrosis have also been observed, which could be correlated with the state of chronic inflammation that characterizes SS.
1. EMT-Dependent Salivary Gland Fibrosis
A clear link between chronic inflammation and fibrosis has been demonstrated in SGs, recently associated with SG atrophy [
28,
29]. In SS, fibrosis seems to be involved in the decreased secretory function of SGs, which leads to hyposalivation and xerostomia [
12]. It is now widely accepted that the development of a fibrotic program in SS is due to the production of fibrogenic mediators by inflammatory and epithelial cells; among these mediators, a prevailing role is played by TGF-β1 [
30]. Sisto et al. demonstrated that TGF-β1 promotes salivary gland epithelial cells transition towards mesenchymal cells through the activation of the EMT-dependent fibrosis [
31,
32,
33]. Experiments performed on human salivary gland epithelial cells in vitro demonstrated that TGF-β1 was able to shift salivary gland epithelial cells from the classic cobblestone morphology to a more fibroblast-like morphology characterized by a weakening of cell–cell adhesion. This was supported by the observation that SS SG biopsies show an elevated expression of TGF-β1 [
34].
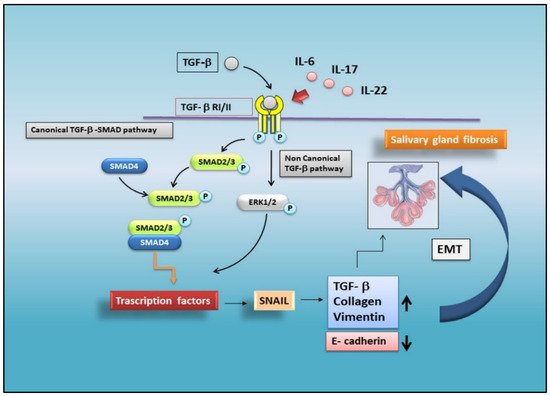
The aberrant upregulation of TGF-β1 in the SS SGs causes EMT via the activation of canonical and non-canonical pathways. As recently demonstrated, the TGF-β1/SMAD/Snail signaling pathway was involved, as confirmed by the detection of a wide distribution of TGF-β1, pSMAD2/3, and SMAD4 proteins in the SS SG tissues. Furthermore, in SS SGs, a strong positivity for EMT-cascade factors and mesenchymal markers was also evidenced, such as SNAIL, vimentin, and collagen type I. Additionally, SS SGs were characterized by a decreased expression of typical epithelial markers, such as E-cadherin [
11,
35] (
Figure 1).
Figure 1. Schematic representation of TGF-β-mediated EMT signalling in SS. In a situation of chronic inflammation, TGF-β activates the canonical SMAD2/3 and the non-canonical ERK-mediated pathways, triggering the EMT process in salivary gland epithelial cells. The activation of transcription factors (such as SNAIL), promotes the prolonged induction of EMT, repressing epithelial marker genes and activating genes linked to the mesenchymal phenotype. Pro-inflammatory cytokines, such as IL-17, IL-22, and IL-6, induce EMT-dependent severe fibrosis in SGs.
A breakthrough in research has recently been made showing that the loss of epithelial markers and the acquisition of mesenchymal markers was strictly correlated with the grade of SG inflammation. Currently, attempts to explain the development of fibrotic phenomena in SS SGs, induced by the initiation of an EMT program, have focused their attention on the role of several pro-inflammatory cytokines. The results are very encouraging; Sisto et al. demonstrated that IL-17 and IL-22 participate in TGF-β1/EMT-dependent SG fibrosis. Both the cytokines are upregulated in SS and linked to low levels of saliva production; in addition, both IL-17 and IL-22 are abundantly secreted in SS SGs and correlated with the inflammatory degree of the glands [
36].
2. Cardiac Fibrosis
Cardiac fibrosis is the accumulation of scar tissue in the heart, and is defined as the imbalance between production and degradation of ECM protein production. Cardiac fibrosis is strongly associated with many cardiac pathophysiologic conditions, and recently, several interesting studies have detected an increased incidence of cardiovascular disease (CVD) morbidity and mortality in patients affected by rheumatic autoimmune diseases, such as SLE and RA [
38,
39]. In recent years, substantial evidence has emerged demonstrating a link of SS with an increased risk of cardiovascular manifestations, such as stroke and myocardial infarction [
40]. Furthermore, intriguing observations have been reported that chronic inflammation in SS patients can trigger a coronary event and, thus, an increased risk of CVD [
40], but this needs further investigation [
40,
41]. Indeed, it was also reported that myocardial injury is typically clinically silent in patients with RA, and this could explain the lack of data on cardiac events in patients with SS, since clinical and pathophysiological characteristics are often shared between RA and SS. In recent papers, it was a high prevalence of myocardial fibrosis in the patients with SS who underwent to cardiac magnetic resonance imaging (cMRI) was observed, which can be used to obtain a quantitative functional evaluation of the myocardium [
42,
43]. In these studies, emerging data highlight that lymphocytic infiltration into the myocardium is conceivable as a pathological characteristic of myocardial fibrosis in SS patients. The results clearly highlight that the higher the extent of lymphocytic infiltration into salivary glands, the greater the possibility of development of myocardial fibrosis [
42]. In fact, myocardial fibrosis is present in patients with SS without cardiac symptoms, and alterations in cMRI data were often linked with SG focus score (FS) ≥ 3 [
42,
44]. This study suggests a significant association between myocardial fibrosis and the degree of lymphocytic infiltration into the SGs as an important prognosis factor for SS [
43]. Yokoe et al., in an interesting study, have obtained several important results from the observation of a representative number of SS patients by the use of non-contrast cMRI, without cardiovascular clinical symptoms [
43]. These findings suggest and confirm that cardiac dysfunction and cardiac fibrosis are strongly evident in SS patients. Furthermore, the importance of this study was to demonstrate that myocardial fibrosis could be considered as an extra-glandular event of SS [
43], and that cMRI could be a useful tool for detecting asymptomatic myocardial fibrosis in patients with SS with a higher SG FS [
42].
3. Liver Fibrosis
The autoimmune destruction of exocrine glands that occurs in SS often extends to non-exocrine organs. Liver involvement was one of the main extra-glandular events reported in patients with SS [
45,
46]. In this context, the main causes of liver disease in primary SS are chronic viral hepatitis infections and autoimmune hepatitis [
47]. With regards to viral infections, chronic hepatitis C virus infection is often involved in hepatic impairment in SS patients deriving from the Mediterranean area, while chronic hepatitis B virus infection seems to be the main cause of liver involvement in Asian SS patients. Autoimmune hepatitis is the second leading cause of liver damage in SS patients [
47]. Liver fibrotic processes depend on the activation of an initial injury of hepatocytes by autoreactive immunological phenomena; these events lead to the proliferation of myofibroblasts and the activation of stellate cells [
48]. These manifestations may, in turn, accelerate the deposition of collagen or glycoproteins in the liver, leading to liver fibrosis that interferes with the liver function and contributes to gradual organ failure [
49]. The immunological parallel between SS and autoimmune-related hepatitis increases the progression and the development of liver fibrosis in SS. Thus, the assessment of the presence of liver fibrosis and its severity might have a value as prognostic factor in patients with SS. In a recent study, the transient elastography (TE) technique was used, which represents a new non-invasive method for the assessment of hepatic fibrosis in SS patients with normal liver function and structures, and without manifestations of evident liver diseases [
46]. Using this approach, a high percentage of SS patients examined present a substantial liver fibrosis, suggesting that the frequency of potential liver fibrosis may have been underestimated in SS patients without clinical symptoms. Furthermore, this study proposed that TE could be used to evaluate the degree of hepatic fibrosis at an earlier stage of SS disease with a notable precision grade [
46].
4. Lung Fibrosis
Pulmonary involvement in SS is an understudied condition with important clinical implications. The common pulmonary manifestations of SS are interstitial lung disease (ILD), airway abnormalities, and lymphoproliferative disorders [
50]. Among them, ILD represents a frequent extra-glandular manifestation of SS, with the majority of the studies indicating a prevalence of about 20%, and resulting in significant morbidity and mortality [
50,
51]. This condition is associated with an injured respiratory function that leads to a poor quality of life and, indeed, is considered a significant cause of fatal outcomes in SS [
52]. Therefore, the identification of poor prognostic predictive factors is required in order to provide appropriate management in patients with SS-associated ILD. When ILD includes scar tissue and the injury and damage of the walls of the air sacs of the lung, as well as in the tissue and space around these air sacs, this condition is known as pulmonary fibrosis. Pulmonary fibrosis is part of this wide group of more than 200 ILD. Efforts have been made to characterize the relationship between SS and ILD, with an emphasis upon idiopathic pulmonary fibrosis (IPF). Roca et al. highlighted that ILD is observed in a significant percentage of SS patients, and that this condition is associated with severe lung injury that develops versus fibrosis pulmonary [
53]. Recently, an interesting study was addressed to systematically evaluate the incidence and characterize ILD fibrosis phenotype in a well-defined SS-ILD cohort [
54]. These data have revealed that pulmonary disease is commonly linked with SS, resulting in a wide variety of clinical manifestations [
54]. Firstly, symptomatic lung involvement triggers scar tissue and injury, provoking an evolution toward a progressive fibrosing phenotype in the lung identified in 13% of SS patients and so confirming previous investigations [
55,
56]. The second important implication is the need for effective SS screening in patients presenting apparently idiopathic ILD [
54]. Subsequently, recent studies from different countries have, however, all observed that the prognosis of pulmonary involvement is not favorable in patients with SS [
57]. Thus, early ILD and IPF detection is very important in SS disease evolution [
58]. However, it remains controversial whether all SS patients should undergo a systematic search for lung involvement [
59] with the view to redefine disease recognition strategies.
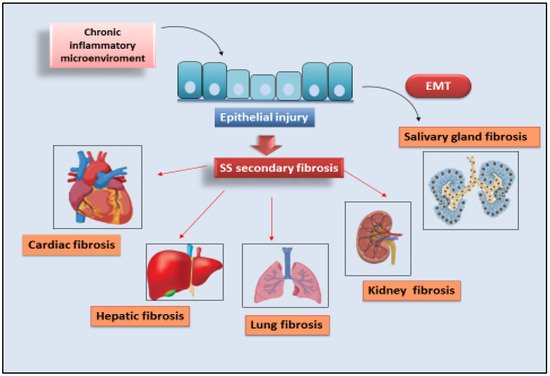
A schematic representation of all the identified secondary fibrosis in SS is shown in Figure 2.
Figure 2. Secondary organ fibrogenesis in SS. Chronic inflammatory microenvironment cooperates for the progression of organ fibrosis in SS patients. Injury events lead to organ damage, inflammation, and fibrosis in the liver, kidney, lung, heart, and SGs.
This entry is adapted from the peer-reviewed paper 10.3390/jcm11123551