1. Introduction
OA is an idiopathic disorder, and the management reflects the lack of understanding of the disease. The non-surgical approach involves the usage of treatment such as physiotherapy, kinesitherapy, weight control, drugs. The main drugs used are hormones (parathyroid hormones, calcitonin, leptin), which act as regulating molecular pathways of cartilage metabolism; bisphosphonates (zoledronic acid, alendronate) which act as improving bone metabolism, reducing bone reabsorption; monoclonal antibodies (bevacizumab, adalimumab,) which act on articular cartilage promoting collagen production; statins (atorvastatin, which reduces cartilage degradation); supplements (glucosamine, chondroitin sulfate, vitamin C, vitamin D, Selenium, Zinc, Magnesium), which act as a cartilage nourishment [41,42].
2. Regenerative Treatment for Osteoarthritis Disease
2.1. Platelet-Rich Plasma (PRP)
Platelet-Rich Plasma (PRP) may be described as plasma volume platelet concentration derived from centrifuged whole blood [
43]. Numerous platelets or thrombocyte functions involve damage to tissue, and platelet activity leads to the release of proteins and molecules that are related to vasoconstriction, inflammation, immune reaction, angiogenesis and the repair of tissue. PRP is rich in growth factors such as platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), transforming growth factor beta (TGF-b), epidermal growth factor (EGF), fibroblast growth factor (FGF) and insulin-like growth factor (IGF) [
44]. Various preparations have been obtained [
45], with or without leukocytes [
46,
47]. Some authors have highlighted that, in the case of intra-articular infiltration, the presence of leukocytes is of vital importance as they produce metalloproteinases and cytokines that are able to reduce inflammation and pain [
48,
49] as well as release mediators that trigger a cartilage repair process [
50]. In contrast with the evidence reported by “in vitro” studies, where a cellular pro-inflammatory response appears to be induced by the presence of leukocytes, other authors suggest that the presence of leukocyte-rich PRP does not induce a relevant in vivo upregulation of pro-inflammatory mediators [
51]. PRP is efficient in mediating fundamental elements such as chemokines, cytokines, growth factors, adhesive proteins, proteases and other small molecules (ADP, Serotonin, Calcium, Histamine and Epinephrine). In addition, safety of PRP has been observed in repeated administration of intra-articular PRP to manage moderate pain, swelling and effusion [
52]. Furthermore, investigations report beneficial outcomes of PRP to reduce joint pain in the knee affected by OA in a period lasting from 6 to 12 months [
53]. Novel trends are considering the application of PRP intraosseously [
54]. Besides, an observational study has reported improved results at 6 and 12 months on intraosseous and intra-articular application of PRP compared to the intra-articular administration alone [
55]. However, evidence of overall benefits is still low and is most likely due to scarce standardization of platelet-rich-plasma therapeutics.
2.2. Mesenchymal Stem Cells Therapy
Different approaches have been performed as potential regenerative solution for osteochondral replacement: osteochondral autografts and allografts or autologous chondrocyte implantation [
56]. Moreover, the clinical use of these techniques is limited by tissue availability, donor site morbidity and unsuccessful integration. In response to limitation with the use of cells in the osteochondral grafts, mesenchymal stem cells (MSCs) have been identified in the field of regenerative surgery. Mesenchymal stem cells (MSCs) are located in numerous tissues and may be defined as specialized precursor cells. MSCs are able to self-generate and, via relevant signals, may differentiate into different tissue-specific adult cells. In that way, MSCs will substitute aged or impaired cells [
57]. MSCs form the tissues of the mesodermal line such as cartilage, bone and adipose tissue, as well as tissue such as the intervertebral disc, ligaments and muscles [
58]. The International Society of Cellular Therapy [
59] established a set of defining characteristics for MSCs which include the ability to adhere to plastic, expression of surface markers CD73, CD90, CD105 and a lack of hematopoietic markers CD34, Cd45, CD14, CD19. Moreover, characteristics would include tripotent differentiation into chondrogenic, osteogenic, and adipogenic phenotypes. In addition to their differentiating capacities, MSCs also represent noteworthy potential in regenerative medicine due to their anti-inflammatory and immunomodulatory potential [
60]. MSCs are considered fundamental in tissue engineering since they are able to differentiate into terminal specialized cells, although currently, MSCs are exploited to “convince” the tissue or organ to self-regenerate. Regenerative medicine intends restoration principally via cell provision and specific stem cells that further enhance regeneration. It is therefore valid to define regenerative medicine as the restoration of human cells, tissue or organs to maintain regular functionality [
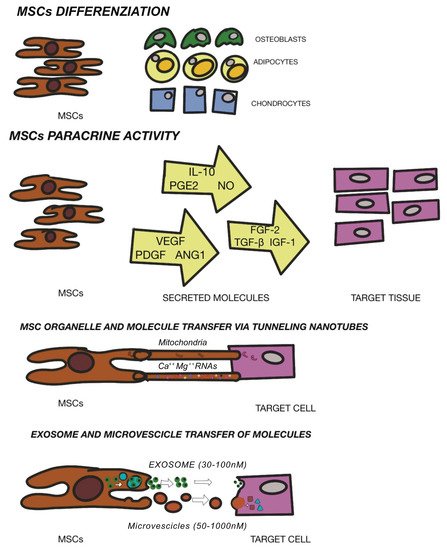
61]. As aforementioned, the beneficial effects of MSCs are due to enhancement of both viability and proliferation of native cells, mitigation of cell death, delay cell senescence and anti-inflammatory and immunomodulatory effects. These reparative actions are obtained through MSC-secreting paracrine growth factors and cytokines, dynamic and direct cellular inter-communication along with extracellular vesicle release (defined exosomes)-containing peptides, mRNA and microRNAs [
62,
63,
64]. The regulation of stem cell renewal and differentiation occur in the “niche” [
65]. Multiple niches may be observed in different tissues [
66] and stem cells contained here within have been utilized to repair cartilage. MSCs have been found in bone marrow [
67], adipose tissue [
68], dental pulp [
69], umbilical cord tissue [
70], but also in resident joint tissue such as the articular cartilage, synovium, periosteum, infrapatellar fat pad and trabecular bone [
38]. The efficacy of stem cell treatment for OA has not yet been defined, but the secretion of anti-scarring (KGF, SDF1, MIP1a, MIP1b), anti-apoptotic (STC-1, SFRP2, TGFbeta1, HGF), angiogenic (VEGF), and mitogenic (TGF-a, TGF-b, HGF, IGF-1, FGF-2, EGF) factors may explain the natural repair mechanisms [
71]. Other investigations have demonstrated a possible interaction between immune cells and MSCs as well as the potential to restrain propagation of inflammatory T cells and development of monocytes and the ability to impede B cell activity, which interfere with the underlying pathological or inflammatory process [
72]. AI Caplan has proposed that the pericyte is released from its position in the vascular network in the case of a focal injury and have an immunomodulatory function. This immune modulation turns off T-cell surveillance of the injured tissue and thus provides a blockage of immune responses, while its trophic activity ensures that the field of damage is limited, that scarring does not occur and that tissue-intrinsic progenitors replace the expired cells. Angiogenesis occurs via MSC secretion of bioactive factors, such as VEGF, and via stabilization of newly forming vessels [
73]. The new era of cell-mediated therapy (
Figure 1) in the clinical trial database is promising. Multiple ongoing trials involving MSCs are evidence of the growing interest and viability of these cells. Further investigations are required to assess safety and subsequent efficacy with an urgency of broad diffusion of publications within the scientific communities to better understand therapeutic options.
Figure 1. Mechanism of MSC mediated repair. Modified from Fellows CR et al. Front Genet. 2016.
2.3. Intra-articular Application of Autologous Microfragmented Adipose Tissue with Stromal Vascular Fraction
Adipose stem cells (ASCs) are able to renew themselves and create multiple lineages [
74]; besides, they can readily and rapidly expand in vitro, will not age easily and provoke fewer morbidities in patients [
75]. ASCs have also displayed significant potential to propagate and differentiate into mesoderm-like tissue in relation to bone marrow derived- MSCs or other sources [
76]. Importantly, ASCs are easily isolated and particularly accessible from subcutaneous adipose tissue [
77,
78,
79]. ASCs have also shown efficient chondrogenic differentiation during in vitro expansion under adequate conditions [
80]. In any case, physical and mechanical factors are required to perform an adequate formation of the cartilage tissue in vivo such as mechanical stimuli or a particular texture of the scaffolds [
81,
82]. The clinical use of ASCs is strictly regulated, because these products are considered “drugs” and therefore particularly restricted in clinical practice in Europe and the USA [
83]. Such restrictions have led to novel studies regarding ASC alternative therapeutics considering “minimal manipulation” [
84]. In particular, if ASCs are not expanded in vitro but extracted from the adipose tissue within the operating room without substantial manipulation and without use of collagenase, then the United States Food and Drug Administration (US FDA)/European Medicine Agency (EMA) allow such treatments [
85]. Enzymatic tissue digestions are considered by the FDA (and EMA) as “substantial manipulations” and have accordingly imposed important restrictions. The issue of ASC “minimal manipulation” is considered during the isolation of several cells’ populations using mechanical processes to adhere to the regulations set by the FDA and EMA worldwide [
86]. Additionally, alteration of biological, physiological, or structural features of cells or tissues is considered as important manipulation. The bone marrow aspirate concentration is an invasive procedure provoking donor morbidity, while the liposuction for obtaining SVF is a minimally invasive procedure [
87]. Albeit efficient, the enzymatic digestion necessitates xenogenic substances that may cause immune reactions and is discordant with the European Good Manufacturing Practice (eGMP) Guidelines (Regulation (EC) No. 1394/2007 of the European Parliament and the European Council). To elude this problem, single devices have been adopted to separate and isolate SVF from adipose tissue [
88,
89]. Non-enzymatic methods to isolate SVF use mechanical or physical forces to manipulate the structural integrity of adipose tissue. These procedures are less specific and are sufficiently able to displace SVF cells from their own niche, and some authors have consequently introduced the concept of a stromal vascular niche [
90,
91]. The end product acquired via non-enzymatic digestion is not strictly cellular stromal vascular material, as would be generally acquired via enzymatic digestion, but a combination of cellular debris, blood cells, and components of ECM [
92]. Moreover, the mechanical devices can preserve cells in clusters, or rather, in their native environment, which will aid in retaining cell function, including exosome discharge and secretion. The stromal vascular niche, therefore, protects the activated ASCs, enhancing their potency in the recipient environment, but also actuates a cascade of biological events that mimic the natural healing process. Non-enzymatic procedures have been proposed including mechanical dissociation of adipose tissue using closing devices and operator-dependent tools (
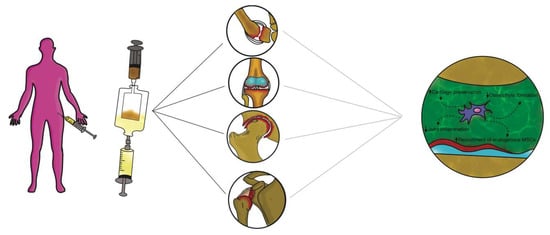
Figure 2).
Figure 2. Non-enzymatic procedures have been proposed including mechanical dissociation of adipose tissue using automated closing devices and non-operator-dependent tools.
These devices differ from each other in the isolation protocol, in time and in the category of tissue dissociation, but also vary in the final SVF product. Non-enzymatic isolation methods are based on centrifugation force, pressure, filtration and washing. Mechanical systems commonly used to harvest and purify adipose tissue to obtain SVF are: Puregraft (Bimini Technologies LLC, Plano, Texas, USA), LipiVage (Genesis-Byosystems-Inc, Lewisville, Texas, USA), Lipogems (Lipogems Int Spa, Milan, Italy), Rigenera (HBW srl, Turin, Italy), Lipo-Kit GT (Medikan-International Inc, Seul, Korea), Hy-Tissue Nanofat (Fidia Farmaceutici, Abano Terme, Italy), Hy-Tissue SVF (Fidia Farmaceutici, Abano Terme, Italy), StromaCell (Micro-Aire-Surgical Instruments, Charlottesville, Virginia, USA), MyStem (MyStem LLC, Wilmington, NC, USA), Revolve (Life Cell Corporation, Branchburg, New Jersey, USA), Wal Body-Jet and Q-Graft system (Human Med AG, Schwerin, Germany), IntelliCell (Biosciences Inc, New York, NY, USA). Many of the devices reported have received evaluations in pre-clinical and clinical trials. Older systems are LipiVage and PureGraft, which were among the first products to be commercialized [
93,
94]. The LipiVage collection, washing and transfer technology is a device that allows collection of adipose grafts in controlled conditions with low vacuum, avoiding centrifugation or decantation. The lipoaspirate fat, inside the cannula, is separated from oils and fluids by an integrated filter in an extremely short time (15 min). In addition, fragmented adipose tissue from LipiVage showed no differences by normal adipose tissue, yielding large-sized grafts. However, an analysis of particles has not yet been conducted. The PureGraft technology is based on the filtration of adipose tissue through a particular membrane, an equally rapid procedure (15 min). In addition, grafts from PureGraft displayed larger particles (>1000 μm) and were able to operate a “dialysis” of the adipose tissue without resorting to other, more destructive methods such as centrifugation [
95]. The main use of these technologies is in the field of fat grafting for breast volumes [
96]. The most studied and commonly used system in clinical practice is the LIPOGEMS device. This technology is a closed device that allows collection of uniform products containing pericytes/ASCs with a slight mechanical force The end product is adipose tissue reduced into small fragments (600 / 400 μm), which progressively reduce in size and are without oil or blood residues, rich ASCs [
97,
98]. This device has been widely used especially in orthopedics for the treatment of tendinopathies and osteoarthritis [
99,
100]. Moreover, some authors have devised a “pure” system of mechanical disintegration [
101] of tissues that is easy to use, less expensive and faster. This technology, called Rigenera micrografting technology, can disaggregate autologous tissue, with a calibrated size of 80 mm, collecting autologous micrografts enriched in progenitor cells, growth factors, and particles of ECM, by in vitro studies [
84,
102]. Some authors have performed comparative analyses between different mechanical and enzymatic systems. Raposio et al. [
103,
104] compared two procedures for isolation of ASCs, based on enzymatic + mechanical (centrifugation/vibrating plus collagenase) and mechanical (centrifugation or vibrating) methods. The authors showed that the enzymatic + mechanical procedure endorsed a major number of ASCs compared to the mechanical method alone. Indeed, Domenis et al. [
105] showed that ASCs obtained from a mechanical device (Fastem kit) was less efficient in relation to the enzymatic tools (Lipo-kit and Celution). All three procedures, nevertheless, were able to maintain the amount of adipose tissue and thickness in the reconstructed breast. Additionally, Senesi et al. [
106] showed good cell viability, CD markers expression, and differentiation potency of ASCs obtained from mechanical devices (Rigenera and Lipogems) compared to enzymatic digestion. Furthermore, the authors asserted that the mechanical methods acted differently on the release of the ASCs from the SVF perivascular niches. Only enzymatic digestion was able to acquire a “pure” cell population and ASCs could rapidly differentiate into all mesodermal lines. Of the two mechanical systems analyzed, only the micro-grafts obtained by Rigenera (compared to Lipogems) were able to differentiate into all mesodermal lines, albeit more slowly than by enzymatic digestion. Some authors have studied a new promising device (Hy-Tissue SVF) that allow the stromal vascular fraction to isolate in the form of free cells and micro-fragments (30 / 70 μm) of connective tissue containing stromal cells and extracellular matrix [
107]. This system is able to disaggregate autologous adipose tissue using a double bag with an inner filter bag of 120 μm mesh by using a small plastic rod. The main structural and morphological unit, the adipose niche, is maintained after disintegration and protects the activated ASCs, strengthening their effectiveness in the receiving environment. This is the main difference between this system and the others, because the preservation of the adipose structural niches increases the effectiveness of the ASCs. In addition, the elimination of enzymatic action will reduce tissue trauma while maintaining cellular integrity. The reduction in the size of adipose clusters favors engraftment because of a more convenient, more effective, and rapid revascularization of the micrograft owing to the interaction with the receiving vascular microenvironment.
2.4. Exosome and Extracellular Vescicles (EVs)
Studies have revealed that MSCs are able to modulate the gene expression of the surrounding cells through miRNA secretion and provide relevant exosome involvement in the benefits of MSC-based therapy [
108]. Exosomes are extracellular vesicles with a diameter measurement ranging from 30 to 150 nm. In the course of multi-vesicular body development, inward budding of endosomal membranes is observed which contributes to the fundamental inter-cell communication. The multi-vesicular body endosomes fuse with the cell membrane leading to secretion of exosomes [
109,
110]. Most of the MSC paracrine factors are crucial to tissue regeneration and lined to the discharge of EVs. MSC exosomes (
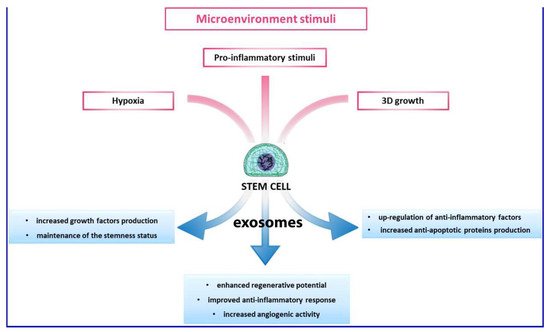
Figure 3) originate in adipose tissue, the bone marrow and other tissues and bear a rich and complex load of nucleic acid (mRNA and miRNA), proteins and lipids [
111].
Figure 3. Different modes of action of exosomes.
In OA, the in vitro studies revealed chondroprotective and anti-inflammatory functions of exosomes, as observed in chondrocyte models [
112]. Moreover, in various studies, the significance of exosomes has been demonstrated as regards the benefits of MSC-based therapies in treating cartilage lesions and OA. Outcomes in pre-clinical trials have shown efficacy of MSC exosomes in cartilage repair and renewal, enhancing chondrocytes to amalgamate type II collagen and reduce production and expression of ADAMTS-5. Such a development will ensure ECM [
113] as well as boost restoration of cartilage via paracrine signaling mechanisms along with secretion of soluble trophic factors [
114]; reduction in inflammatory markers (iNOS) [
115] and downregulation of inflammatory signals by secretion of IL-1, IL-6, IL8, MMP-1 and MMP-13 [
116]. EVs that are isolated from human ASCs use various chondroprotective mechanisms to reduce inflammatory mediators (TNF-alpha, IL-6, PGE2, NO) and minimize MMP activity therefore enhancing generation of the anti-inflammatory cytokine IL-10 [
117]. Many authors demonstrated, also, that exosomes from ASCs could inhibit and defer cartilage deterioration in OA models through the suppression of catabolic molecules [
118] and through the immunoregulatory stimuli of hyaluronan [
119]. These pioneering findings have consolidated the positive outcomes of ASC-derived EVs as a new therapeutic alternative for OA. Adequate investigations are scarce, especially considering these therapeutic options as authentic products of mechanical digestion activated by the various available medical devices. In any case, a detailed analysis to investigate the functions and mechanisms of exosomes in clinical practice is urgently required taking into account the positive outcomes of preclinical studies. In clinical trials, therapy based on exosomes derived from ASCs should aim to optimize criteria involving exosome concentration and dosage, with injection times and intervals. Additionally, the immune response in individuals is to be assessed following exosome administration.
This entry is adapted from the peer-reviewed paper 10.3390/ijms221910197