Sickle cell disease (SCD) is the most common hereditary disorder of hemoglobin (Hb), which affects approximately a million people worldwide. It is characterized by a single nucleotide substitution in the β-globin gene, leading to the production of abnormal sickle hemoglobin (HbS) with multi-system consequences. HbS polymerization is the primary event in SCD. Repeated polymerization and depolymerization of Hb causes oxidative stress that plays a key role in the pathophysiology of hemolysis, vessel occlusion and the following organ damage in sickle cell patients. For this reason, reactive oxidizing species and the (end)-products of their oxidative reactions have been proposed as markers of both tissue pro-oxidant status and disease severity. Although more studies are needed to clarify their role, antioxidant agents have been shown to be effective in reducing pathological consequences of the disease by preventing oxidative damage in SCD, i.e., by decreasing the oxidant formation or repairing the induced damage.
1. Introduction
Sickle cell disease (SCD) is an inherited hemoglobinopathy and the most common severe monogenic disorder in the world. The United Nations (UN) and the World Health Organization (WHO) define the inherited blood disorders such as SCD as a global health problem, since there are more than 300,000 births annually affected [
1,
2,
3].
This disease prevails in large areas of sub-Saharan Africa, the Middle East, India, the Caribbean, South and Central America, some countries along the Mediterranean Sea, as well as the United States and Europe. The global distribution of SCD is driven by two factors: (i) selection for carriers through their survival and (ii) population movements [
4,
5,
6].
SCD is caused by a single nucleotide substitution (GTG for GAG) at the sixth codon of the β-globin gene, which is located on the short arm of chromosome 11 [
7]. This induces the substitution of valine for glutamic acid at the sixth amino acid position in the β-globin chain, leading to the production of abnormal HbS (sickle hemoglobin), which has the propensity to polymerize under conditions of low oxygen saturation, such as occur in the microcirculation [
8]. HbS polymerization is the primary event in SCD. Repeated polymerization cycles cause irreversible damage to red blood cell (RBC) deformability, while a single polymerization results in reversible decreased RBC deformability and increased mechanical fragility [
9].
In addition to homozygous sickle cell disease (HbSS), other forms of such sickling hemoglobin anomalies exist, such as HbSC disease and HbSβ-thalassemia [
10]. Repeated sickling of the RBCs results in membrane fragility and hemolysis, ischemia-reperfusion, occlusion of post-capillary venules and infarction [
11].
Sickle cell disease is a chronic disease that has detrimental effects on the entire body and requires a multidisciplinary team for management.
In addition to HbS polymerization, vessel occlusion and hemolytic anemia, which play a central role in the pathophysiology of SCD, vascular-endothelial dysfunction, functional nitric oxide deficiency, inflammation, oxidative stress, reperfusion injury, hypercoagulability, increased neutrophil adhesiveness and platelet activation can lead to several complications [
4].
A wide variability was observed in the clinical severity of SCD, as well as in the life expectancy [
12]. Genetic variants controlling the expression of the HbF (fetal hemoglobin) genes and coinheritance of the α-thalassemia gene are associated, on average, with milder SCD phenotypes [
12]. The role of other potential genetic modifiers is less clear.
The health and survival of children with sickle cell disease has been improved considerably by penicillin prophylaxis, pneumococcal immunization, advent of newborn screening and education about disease complications.
Wider use of transfusions, hydroxycarbamide and newer therapeutic approaches have offered hope for improved health-related quality of life and decreased mortality. Nevertheless, even with the best of care, life expectancy of affected adults is still reduced by about 30 years.
Pathological events occurring in sickle cell disease increase the free-radicals generation through activation of pro-oxidant enzymes, release of free hemoglobin, and heme induced by hemolysis which foster Fenton reaction, modification of mitochondrial respiratory chain activity and RBC auto-oxidation [
10,
13,
14]. Excess of free radicals contributes to increased oxidative stress in RBCs, endothelial cells (ECs), neutrophils and platelets, which manifests as multiorgan vasculopathy.
Oxidative stress is defined as the imbalance between the levels of reactive oxygen species (ROS), reactive nitrogen species (RNS) and antioxidants activity or concentration. ROS derive from the reduction of molecular oxygen and include radical species, such as the poorly reactive superoxide anion radical (O
2•−) and the strong reactive hydroxyl radical (
•OH), as well as non-radical oxidants such as hydrogen peroxide (H
2O
2), hypochlorous acid (HClO) and hypobromous acid (HOBr) [
11,
14,
15]. Similarly, RNS include radical species, such as the poorly reactive nitric oxide (
•NO) and nitrogen dioxide (
•NO
2) and non-radical species such as nitrous acid (HNO
2), dinitrogen trioxide (N
2O
4) and peroxynitrite (ONOO
−). The latter, formed by the interaction between
•NO and O
2•−, can induce irreversible modification of the activity and function of several key intracellular targets through the formation of strong oxidizing radicals such as
•NO
2 and carbonate radical (CO
3•). Moreover, peroxynitrite can induce the oxidation and nitration of sensible key target compounds, such as thiols, damaging cell membranes and mitochondria, causing DNA strand breakage and apoptosis [
16]. The oxidation of biological molecules such as proteins, lipids, carbohydrates and DNA persists when it is not neutralized by the defense mechanisms, leading to impaired intracellular signaling, cellular dysfunction and death [
10,
11].
To counteract ROS and RNS, both non-enzymatic and enzymatic defense mechanisms have evolved [
10,
11]. Non-enzymatic antioxidants include ascorbic acid, glutathione, tocopherols, carotenoids, riboflavin and microelements such as zinc [
10]. Enzymatic antioxidants include superoxide dismutase (SOD), catalase (Cat), glutathione peroxidase (Gpx), glutathione reductase, glutaredoxin (Grx), thioredoxin/thioredoxin reductase system and peroxiredoxins (Prx) [
10].
Due to the high levels of oxidative stress, levels of both enzymatic and non-enzymatic antioxidants are reduced in SCD [
16,
17,
18]. A wide range of non-enzymatic antioxidants has been found to be deficient in red blood cells, mononuclear cells, and platelets of SCD patients. They include glutathione, vitamin E and C, β-carotene, and plasma retinol [
16,
17,
18,
19]. Serum and plasma levels of the enzymatic antioxidants SOD, Gpx and Cat are also diminished [
16,
17,
18,
19].
The emerging idea for new SCD therapeutic approaches is that vasculopathy, adhesion events and inflammation, formation of dense RBCs, as well as oxidative stress might constitute new pharmacological targets. Oxidative stress is an important feature of SCD. In fact, reactive oxidizing species and the (end)-products of their oxidative reactions are potential markers of disease severity, thus representing targets for antioxidant therapies.
2. Source of ROS in SCD
In SCD, reactive oxidizing species are generated by sickle RBCs as well as by activated leukocytes, platelets, ECs, and plasma enzymes. Several mechanisms contribute to ROS and RNS formation in tissues of SCD patients such as (i) increased activity of nicotinamide-adenine dinucleotide phosphate (NADPH) oxidase and endothelial xanthine oxidase (XO) [
8,
10], (ii) HbS autoxidation [
11], (iii) heme and iron release, (iv) increased asymmetric dimethylarginine (ADMA) [
12,
13], and (v) uncoupling of nitric oxide synthase (NOS) activity and decreased
•NO bioavailability [
20].
2.1. Increased Activity of Several Oxidases
It has been demonstrated that in SCD, the enzymes NADPH oxidase, XO and uncoupled endothelial nitric oxide synthase (eNOS) can generate ROS in the vascular compartment [
21,
22,
23,
24].
NADPH oxidase is the major O
2•− producing enzyme in leucocytes, vascular endothelial cells and RBCs. ROS produced by activated leucocyte NADPH oxidase contribute to the hemolysis associated with infections or vessel occlusive crises [
23]. The O
2•−, derived from endothelial cell NADPH oxidase, contributes to the pro-inflammatory and pro-thrombogenic responses associated with SCD [
24]. In RBCs, NADPH oxidase activity is regulated intracellularly by protein kinase C and Rac GTPases and extracellularly by signaling factors such as transforming growth factor β1 and endothelin-1 present in the plasma from SCD patients [
24]. ROS derived by RBC NADPH oxidase may cause direct oxidative damage to a variety of subcellular structures, reducing RBC deformability and resulting in increased RBC fragility and hemolysis [
24].
XO represents a potent source of superoxide O
2•− and H
2O
2, and its activity is increased in the plasma of SCD patients. The source of XO is not completely clear, but episodes of hypoxia/reoxygenation in SCD patients can stimulate the release of this enzyme from the liver into the circulation. Increased circulating XO can then bind avidly to vessel luminal cells and impairing vascular function and creating an oxidative milieu [
25].
2.2. HbS Autoxidation
Normal RBCs continuously generate ROS during oxygenation/deoxygenation cycles occurring in the circulation. The oxygen exchange physiologically generates a continuous slow autoxidation of oxygenated Hb (ferrous, Hb-FeII) producing O2•− and methemoglobin (ferric, Hb-FeIII), which no longer binds oxygen, at a rate of 0.5–3% per day. The spontaneous and enzymatic O2•− dismutation forms H2O2, but both these species are neutralized by the efficient RBC antioxidant system involving both non-enzymatic low molecular weight antioxidants (glutathione, ascorbic acid and vitamin E) and enzymatic antioxidants (SOD, Cat, GR, Prx2 and Gpx). These antioxidant activities, coupled to the methemoglobin reductase-dependent reduction of Hb-FeIII to Hb-FeII, preserve RBCs integrity and function. Under conditions of oxidative stress, ROS are produced in greater quantities in normal RBCs, which by activating the pseudo-peroxidase cycle detoxify the generated oxidants leading to the complete consumption of H2O2.
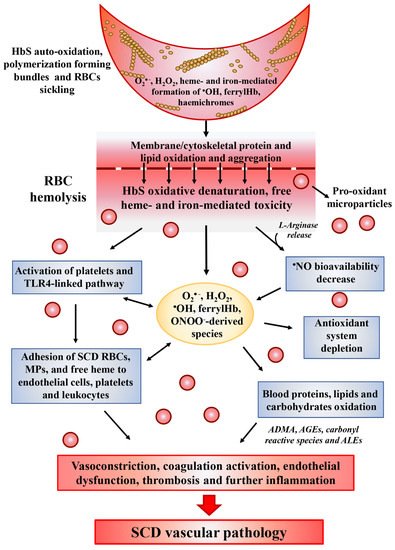
In SCD, intravascular hemolysis results in the toxic accumulation of free HbS and heme in the plasma (
Figure 1). Compared to normal Hb, HbS molecules are highly unstable in particular under hypoxic condition and more prone to autoxidation [
26,
27]. The rate of HbS autoxidation has been calculated to be about 2 times faster than that of normal Hb, resulting in the increase of about 2 times the generation of O
2•−, H
2O
2,
•OH and lipid oxidation products [
28,
29]. This exacerbated pseudo-peroxidase cycle is followed by heme release and iron loss, both able to amplify oxidative reactions. In addition, the autoreduction of ferryl back to ferric heme is slower than that of normal Hb, leading to a longer lived and more damaging free ferryl Hb and to free ferryl radical. The latter has been shown to migrate and induce further damage in the protein, including the irreversible oxidation and dimerization of Cysβ93, as well as to induce, in target cells, damage and dysfunction in other biological organelles, such as in the mitochondria likely, contributing to SCD-induced vascular pathology [
29]. In SCD, as well as in other hemolityc disorders, the high amounts of plasma hemoglobin is in the ferrous form and can stoichiometrically react with equivalent amounts of
•NO [
30]. This reaction leads to the in vivo formation of
•NO–hemoglobin deoxygenation end-products (methemoglobin, nitrate) and iron–nitrosylhemoglobin complexes, thus contributing to decrease
•NO bioavailability [
30].
Figure 1. Pathophysiological effects of oxidative stress in sickle cell disease (SCD). Following oxygenation/deoxygenation cycles, HbS in RBCs undergoes autoxidation generating reactive oxidizing H
2O
2 and the release of free heme and iron. Heme and iron are key players in SCD oxidative damage by (i) catalyzing the generation of strong oxidizing species, such
•OH and ferrylHb through the H
2O
2-dependent Fenton reaction; (ii) boosting platelets activation and adhesion to endothelial cells; (iii) stimulating the Toll-like receptor-4 (TLR4) in endothelial cells, and promoting inflammasome activation and cytokines production (IL-1β, IL-6, IL-18, TNF-α) through NF-κB-linked pathways, (iv) activating neutrophils, leading to the release of neutrophil extracellular trap which can also affect endothelial cells and act as a scaffold for platelets and RBCs; (vi) favoring the expression of adhesion molecules (VCAM-1, ICAM-1, E-selectin, P-selectin) that are all markers of endothelial dysfunction and function as receptors for leukocyte (lymphocytes, neutrophils and monocytes); and (vi) stimulating the blood coagulation, inducing the exposure of intraluminal tissue factor in endothelial cell boosting the coagulation cascade through binding of tissue factor with Factor VIIa. Importantly, the vascular availability of
•NO, which has well known vasodilating, anti-thrombotic, and anti-inflammatory properties, is decreased by the hemolysis-mediated release of (i) HbS and free heme, which can bind
•NO in plasma, (ii) the enzyme L-arginase, which degrades the nitric oxide synthase substrate L-arginine to ornithine, and (iii) the O
2•− enzymatically produced by ROS-generating enzymes (NADPH oxidases, xanthine oxidase and uncoupled NOS) in activated leukocytes and platelets. In this latter case, the fast reaction between
•NO and O
2•− produces the strong oxidant peroxynitrite (ONOO
−) and its derived oxidants (such as
•OH,
•CO
3,
•NO
2). The pro-oxidant status of SCD blood induces the depletion of both extra- and intra-cellular antioxidant defenses. The enhanced release of MPs by SCD RBCs could further exacerbate inflammation and oxidative stress, being overloaded with pro-oxidants molecules (methemoglobin, heme/iron and their derived oxidation products). All these combined pathways contribute to activate a vicious circle, which amplifies the formation of ROS from heme/iron and in cells activated as a result of inflammation. Moreover, it inhibits antioxidants depletion or in some cases boosts their replenishment (see the text) and promotes the oxidation of intra- and extracellular targets, i.e., proteins and lipids leading to the formation of asymmetric-dimethyl arginine (ADMA). In particular, new carbonyl groups can be introduced into proteins by: (i) direct oxidation of lysine, arginine, proline and threonine residues; (ii) reaction of oxylipin carbonyls bearing α,β-unsaturated bonds, such as a number of aldehydes (e.g., acrolein, malondialdehyde [MDA], 4-hydroxy-2-nonenal [HNE], 4-hydroxy-2-hexenal (HHE)) and some isoprostanes deriving from the peroxidation of polyunsaturated fatty acids (PUFAs), with lysyl residues; (iii) reaction of reducing sugars and their oxidation products (e.g., ketoaldehydes like methylglyoxal, deoxyosones like 3-deoxyglucosone and ketoamines) with lysyl residues [
37]. Compounds in group (ii) are referred to as “advanced lipoxidation end-products” (ALEs). Compounds in group (iii) are referred to as “advanced glycoxidation end-products” (AGEs). This inclusive definition should be preferred over the widespread definition of “advanced glycation end-products”. Oxylipin carbonyls bearing α,β-unsaturated bonds, such as acrolein, MDA, HNE, HHE and some F2-isoprostanes deriving from the endocyclization of lipid hydroperoxyl radicals are collectively referred to as “reactive carbonyl compounds” [
38]. Reactive compounds generated by these mechanisms participate in the vicious cycle of leukocyte and endothelial cell activation, leukocyte aggregation with RBCs/MPs and platelets, and eventually vascular occlusion.
2.3. Heme and Iron Release
Under mild to moderate hemolysis, Hb is bound in plasma by haptoglobin (Hp) forming a complex, which prevents the release of free iron while continuing to maintain the ability to bind
•NO [
31]. The complex is internalized and degraded through the CD163 receptor found on macrophages and CD91 receptors found on hepatocytes [
32]. The release of heme from HbS is faster than from normal Hb [
29]. Its characteristic hydrophobicity allows heme to intercalate into the cell membranes and magnify the intracellular heme-dependent reactive oxidizing species generation. In addition, under inflammatory condition, O
2•− and H
2O
2, released by activated cells, can react with heme and catalyze both the non-enzymatic generation of reactive oxidizing species as well as the release of free reducing ferrous ions, which in turn may increase the Fenton-driven reactions and induce further oxidative and nitrosative stress [
33] (
Figure 1). These events amplify the formation of ROS inside cells leading to additional damage to intracellular components including proteins, lipids, and DNA [
34,
35]. Consequently, fundamental functions of cells may be compromised by this heme- and iron-mediated increase of ROS formation, such as the intracellular signaling mediated by oxidant-sensitive targets, the expression of pro-inflammatory transcription factors, the integrity of membrane channels, the activity of metabolic enzymes, inducing finally cell apoptosis and death. In addition, heme-derived oxidants induce recruitment of leukocytes, platelets and RBCs to the vessel wall; produce lipoproteins oxidation and consume
•NO in the formation of strong oxidants such as ONOO
− (
Figure 1) [
36].
2.4. Decreased •NO Bioavailability
In SCD, all
•NO biological functions, including the regulation of vascular tone, the control of cell activation, aggregation and adhesion in the vascular compartment, are compromised so that vasoconstriction, pulmonary hypertension, endothelial dysfunction, thrombosis and inflammation characterize the vasculopathy linked to this disease [
39,
40,
41]. In the absence of interactions with biological targets,
•NO reacts with oxygen (9 × 10
7 M
−1s
−1) to form nitrite. In biological systems, this reaction is slower with respect to those occurring with metal-containing macromolecules generating either nitrate, as in the case of hemoglobin (6–8 × 10
7 M
−1s
−1) and nitrite in the case of ceruloplasmin acting as a
•NO oxidase and nitrite synthase [
42]. Nitrite is not an inert end-product, but it has bioactivity since it can generate
•NO from its reaction with metalloproteins, as in the case of HbS itself, which has been reported to possess nitrite reductase activity [
43]. In addition, the concentration of these
•NO-derived metabolites is deeply affected by the dietary intake and renal function. In plasma of SCD patients, the concentrations of nitrite and nitrate appear to undergo modifications, i.e., in the steady state of disease they have been found to be comparable to those measured in normal volunteers, but they decreased with acute pain and acute chest syndrome [
44,
45]. The impairment of
•NO availability in SCD is mainly linked to the intravascular hemolysis (
Figure 1). Cell-free hemoglobin has indeed a large impact on the bioavailability of
•NO. While the reaction of
•NO with oxygenated Hb results in methemoglobin and nitrate formation, its binding to deoxygenated hemoglobin favors the formation of a stable FeIIHb-NO complex, which can be involved in Fenton reactions [
36]. Interestingly, a gender difference was also described in
•NO availability in SCD patients. In particular, thanks to the protective effects of estrogen on the expression and activity of NOS, women are more protected from the decrease of
•NO availability [
46].
Another crucial metabolite contributing to vascular impairment in SCD is L-arginine. Besides being used by NOS to generate
•NO, L-arginine is also the substrate of the enzyme arginase, which competes with NOS for L-arginine, generating urea and ornithine. Since the arginase activity is significantly high in RBCs compared to plasma [
47], the hemolysis causes the release of the enzyme from RBCs into plasma allowing to the rapid consumption of L-arginine, reducing the substrate for
•NO synthesis and consequently its bioavailability in SCD (
Figure 1) [
48]. In SCD patients the L-arginine supplementation increases both the nitrite plasma concentration as well as the HbF synthesis, suggesting the beneficial effects of
•NO on the erythroid progenitor cells [
49].
Finally,
•NO-derived metabolite nitrite is also consumed by the heme-containing myeloperoxidase (MPO). This enzyme, localized within neutrophils and released upon cell activation, catalytically reacts with nitrite in the presence of H
2O
2, generating powerful radical intermediates, such as nitrogen dioxide (
•NO
2), which can oxidize and nitrate protein tyrosine residues [
50]. MPO also could contribute to the pulmonary hypertension and acute chest syndrome in SCD, since elevated MPO immunoreactivity has been measured in the alveolar epithelium of lung tissues from patients with SCD [
51].
3. Antioxidant Therapy for SCD
The research of suitable compounds able to (i) limit the hemoglobin-dependent oxidative reactions, (ii) scavenge reactive oxidizing species released and (iii) repair the reactive oxidizing species-mediated tissue oxidative damage is a fundamental step in the clinical management of SCD.
There are currently two types of treatment for SCD: primary treatments, which treat the root causes of the disease (gene therapy and HbF inducers antisickling agents) and secondary treatments, which target one of the downstream sequelae of HbS polymerization. In the secondary type of treatment, beside factors working against adhesion, inflammation and thrombophilia, the antioxidant therapy plays an important role for SCD treatment [
156]. In fact, as already mentioned, oxidative stress can lead to disturbance of cell membranes, exposure of adhesion molecules and damage to the contents of the sickle red blood cells [
157]. In
Table 2 are reported the most promising antioxidant therapeutic strategies, which showed a benefit either in the reducing oxidative stress parameters or in the prevention of pathophysiologic events in SCD patients.
3.1. L-Glutamine
L- Glutamine is a precursor of nicotinamide adenine dinucleotide (NAD) required for antioxidant mechanism through the formation of reduced nicotinamide adenine dinucleotide (NADH) [
156]. Oral administration of L-glutamine in SCD patients has been approved on July 2017 by Food and Drug Administration (FDA).
The RBC oxidative damage is most likely consequence of instability of HbS, increasing in free radical generation and impairing antioxidant defenses. This hemoglobin instability leads to denaturation of HbS, through its oxidation to methemoglobin. Methemoglobin reductases slow down this process using NADH. In sickle RBC, there is a decreased NADH/NAD ratio with a consequent decreased NAD redox potential, manifestation of a compensatory mechanism against increased oxidant sensitivity [
134]. Several trials demonstrated the beneficial effects of oral administration of L-glutamine in SCD in improving cellular redox potential and facilitating protein and glutathione synthesis [
157,
158,
159]. Finally, additional studies suggested that oral L-glutamine supplementation improves the endothelial adhesion of sickle RBC, one of the major factors involved in the pathophysiology of vessel-occlusion. The mechanism underlying this effect is still unclear; however, the improvement of NAD redox potential may protect RBC from oxidant damage and the consequent stimulation of inflammation and expression of adhesion molecules [
158].
Table 2. Antioxidants in SCD therapy.
| Antioxidants |
Mechanisms |
Effects in SCD Patients |
Comments |
| L- Glutamine |
Acts through the formation of reduced NADH. |
Improves cellular redox potential and adhesion of sickle RBCs to the endothelium; facilitates protein and glutathione synthesis. |
FDA approved; [155,156] |
| N-Acetylcysteine |
Substrate for GSH generation. |
Reduces the number of RBCs expressing phosphatidylserine, marker of peroxidative damage to inner membrane of RBCs. |
NCT01800526 phase 2 trial; NCT01849016 phase 3 trial |
| Zinc supplementation |
Zinc deficiency is associated with high incidence of infections, vaso-occlusion events and the chronic oxidative stress. |
In young SCD patients improves linear growth and weight gain. Has beneficial effects on immunity, inflammatory state and oxidative stress. |
NS; [159,160] |
| Nitric oxide |
Reduced •NO concentration can be associated to increased levels of free O2•−. |
Inhaled •NO improves tissue oxygenation and reduces pain in SCD patients with pulmonary hypertension. |
NCT00094887 phase 2 trial |
| L-arginine |
Induces GSH synthesis. |
Improves •NO bioavailability. |
NCT02447874 phase 2 trial |
| Alfa-lipoic acid |
Induces GSH synthesis. |
Increases glutathione level. |
NCT01054768 phase 2 trial |
| L-acetyl-L-carnitine |
Improves mitochondrial metabolism, facilitating entry of long-chain fatty acids into mitochondria and decreasing lipid peroxidation in tissue. |
Decreases lipid peroxidation. |
NCT01054768 phase 2 trial |
| Gum Arabic |
Acts as immuno-modulatory. |
Increases total antioxidant capacity and decreased MDA and H2O2 levels. |
NCT04191213 phase 2 trial |
| Omega-3 fatty acids |
O3FA deficiency correlates with an increase in plasma levels of the inflammatory biomarker |
Have beneficial effects on vascular activation, inflammation and antioxidant systems. |
[156,157,158,159,160,161,162,163,164,165,166,167,168,169,170] |
| Curcumin |
Can modulate the activity of enzymes active in the neutralization of free radicals and it can inhibit ROS-generating enzymes. |
Mitigates the effects of iron induced oxidative stress on lipid peroxidation and •NO levels. |
[169,170] |
| Vitamins A, C and E |
Their deficiency increases susceptibility to infection and hemolysis. |
Conflicting results about the effectiveness of their supplementation on oxidative stress. |
NCT03903133 phase 4 trial |
| Iron chelators |
Avoids excessive iron overload and the consequent ROS generation. |
Have a central role in the treatment of transfusion-dependent hemoglobinopathy. |
NS; [158] |
3.2. N-Acetylcysteine (NAC)
NAC is an important antioxidant with pleiotropic effects on inflammation and vasomotor function [
156,
160]. It is a substrate for the synthesis of GSH, one of the most important intracellular antioxidants and may play an important role as antioxidant treatment. Indeed, within the cytoplasm, NAC is converted to L-Cysteine, which is a precursor of GSH resulting in an increase of its concentration. GSH has been found to be 32–36% lower in RBCs from SCD patients compared to healthy controls, while some antioxidant enzymes involved in oxidant detoxification, such as SOD and Gpx, have been found significantly higher in patients with SCD [
28].
In sickle cell, there is an increased consumption of GSH due to excessive reactive oxidizing species formation, resulting in a decreased ration between GSH and its oxidized form GSSG. In an open label randomized pilot study, Nur and colleagues [
135] observed that NAC treatment reduced oxidative stress. In particular, they observed (i) a reduced cell membrane phosphatidylserine expression, marker of peroxidative damage to the erythrocyte inner membrane, and (ii) a decrease of AGEs and cell-free hemoglobin. The association between AGEs and the degree of hemolysis and organ complication in sickle cell patients and, on the other hand, an inverse correlation with GSH levels has been recently demonstrated. These results probably suggest that, enhancing GSH levels, NAC treatment could reduce AGEs levels and oxidative tissue damage [
135].
3.3. Zinc Supplementation
Zinc deficiency has been implicated in SCD pathological events. Thus, this element as a therapeutic agent may be very useful in these patients. Zinc deficiency was associated with high incidence of infections connected to weakened cell mediated immunity, with vaso-occlusion events correlated with high level of endothelial cell VCAM-1 molecule and with the chronic oxidative stress. In a study of prepubertal children with SCD-SS, the therapeutic effect of zinc supplementation was evaluated on growth and body composition. Results demonstrated that young SCD patients can benefit from zinc supplementation to improve linear growth and weight gain [
161]. Furthermore, in a very important double-blind, placebo-controlled study, zinc supplementation (with 25mg elemental zinc as acetate, three times a day for 3 months) ameliorated several pathophysiological parameters chronically existent in these patients: Beneficial effects were observed on immunity, inflammatory state and oxidative stress [
162].
3.4. Nitric Oxide and L-Arginine
In addition to its role in vascular tone, blood flow and adhesion,
•NO is known to possess antioxidant properties. Moreover, inhalation of exogenous
•NO, can be used to reduce pain in SCD patients with pulmonary hypertension [
86] and microvascular occlusion in different parts of the body, but controversial results are reported by randomized trials (NCT00094887) [
163].
In SCD patients,
•NO concentration declines, and its reduced bioavailability can be associated to increased levels of free O
2•−. Therapy with L-arginine has been demonstrated to improve
•NO bioavailability either in transgenic knockout sickle mice or in SCD patients, although in different clinical trials, conflicting results were obtained [
164,
165]. The cause of this result has in part been attributed to a deficiency of R-BH4 action. This is an endogenous pterin widely distributed in mammalian tissues that works as a cofactor of aromatic amino acid hydroxylases and nitric oxide synthases. In SCD patients, its deficit is implicated in the mechanism of several diseases such as atherosclerosis, hypertension, diabetic vascular disease and vascular complications [
166].
3.5. α-Lipoic Acid and Acetyl-L-Carnitine
Other compounds with antioxidant properties are α-lipoic acid (LA) and acetyl-L-carnitine (ALCAR). LA increases glutathione level, whereas ALCAR decreases lipid peroxidation [
156].
One of the mechanisms of antioxidant protection by LA is the induction of GSH synthesis, with a dose-related mechanism, through inducing Nrf2-dependent transcription of γ-glutamyl cysteine ligase (GCL), the rate-controlling enzyme in the synthesis of GSH [
167,
168]. On the contrary, the reason of the beneficial effect of ALCAR is not so clear; however, this might occur from improved mitochondrial metabolism, facilitating entry of long-chain fatty acids into mitochondria and decreasing lipid peroxidation in tissue. Studies suggest that this nutrient may be able to maintain the normal shape of RBCs and decrease peroxidative damage [
160,
168].
Finally, the evaluation of oxidative stress in human fibroblast exposed to iron excess shows an increased antioxidant effect of combination treatment with LA and ALCAR, suggesting a synergic influence of two compounds [
168].
3.6. Other Antioxidant Agents
Gum Arabic (GA), omega-3 fatty acids and curcumin are reported to diminish oxidative stress in SCD, but their role has not been widely accepted [
156].
Oral intake of GA has been shown to provide several health benefits, such as probiotic, immuno-modulatory, antioxidant and cytoprotective effects. Available experimental data show its protection against hepatic, renal and cardiac toxicities in rats and, due to its antioxidant properties, this compound may find clinical application sickle cell anemia. In a phase II trial, Kaddam and colleagues treated 47 SCD patients with 30 g/day GA for 12 weeks and demonstrated that GA significantly increased total anti-oxidant capacity and decreased MDA and H
2O
2-related oxidative markers [
169].
Limited studies dealing with Ω-3 dietary supplementation are available. Kalish demonstrated the impact of ω-3 fatty acids on vascular activation, inflammation, and antioxidant systems. Authors assessed a modified red cell membrane composition (lower ω -6/ ω -3 ratio), a reduction of neutrophil count and beneficial effects on the cardiovascular system [
170].
Curcumin could mitigate the effects of iron induced oxidative stress on lipid peroxidation and
•NO levels, as showed in rats exposed to iron overloaded toxicity [
171,
172].
Despite the observed increased susceptibility to infection and hemolysis in SCD patients with deficiency of vitamins A, C and E, conflicting results are available about the effectiveness of their supplementation on oxidative stress in these patients.
Finally, the role of iron chelators (deferiprone, deferoxamine and deferasirox) is central in the treatment of transfusion-dependent hemoglobinopathy, avoiding excessive labile iron overload and the consequent ROS generation [
160]. Both in in vitro and in animal models, it has been shown that these compounds (i) decrease the RBC membrane-oxidative damage and the production of lipid oxidation product (deferiprone) and (ii) attenuate blood cell adhesion to endothelial cerebral venules (deferoxamine) [
160]. Finally, in a longitudinal study, SCD patients receiving simultaneously deferasirox and hydroxyurea showed a marked decrease of plasma lipid peroxidation products as well as increased antioxidant capacity levels [
173].
These promising results should encourage the development of the future research focused on the antioxidant therapy also in combination with the drug treatments. This therapeutic strategy targeted to the reactive oxidizing species-releasing pathway and limiting the intra- and extra-cellular oxidative damage, could reduce the clinical complications of the disease with particular regard to SCD-associated vasculopathy.
This entry is adapted from the peer-reviewed paper 10.3390/antiox10020296