The eye, the photoreceptive organ used to perceive the external environment, is of great importance to humans. It has been proven that some diseases in humans are accompanied by fundus changes; therefore, the health status of people may be interpreted from retinal images. However, the human eye is not a perfect refractive system for the existence of ocular aberrations. These aberrations not only affect the ability of human visual discrimination and recognition, but restrict the observation of the fine structures of human eye and reduce the possibility of exploring the mechanisms of eye disease. Adaptive optics (AO) is a technique that corrects optical wavefront aberrations. Once integrated into ophthalmoscopes, AO enables retinal imaging at the cellular level.
1. Introduction
The eye is one of the most important organs for humans to understand their external environment. Most of the knowledge and memory stored in the brain is acquired through the eyes. Further, some diseases, such as diabetes, high blood pressure, atherosclerosis, etc., can be diagnosed by examination of the fundus, which provides a way to interpret the health status of the body. However, it is not easy to detect early retinopathy and fundus lesions, which may cause irreversible visual impairment and even blindness if not treated in time. Fundus imaging is generally used for detecting and diagnosing human diseases that influence the retina. Some kinds of retinal imaging technologies, such as optical coherence tomography (OCT) [
1], flood-illumination fundus camera (FC) [
2], and scanning laser ophthalmoscopy (SLO) [
3], can obtain living human retinal images, but none of them can provide details at the cellular level due to the resolution limitations imposed by aberrations in the human eye. Adaptive optics (AO) provides a solution for ophthalmic imaging with high resolution, which is close to the diffraction limit, to accurately obtain the structural and functional information of retina.
The idea of AO comes from astronomical observations [
4], where AO is used to compensate the dynamic wavefront distortion caused by atmospheric turbulence and allows a telescope to achieve diffraction-limited imaging from the ground. Subsequently, AO has been rapidly developed and applied in the military, astronomy, industrial, civil and medical fields. AO in ophthalmology started in the early 1990s [
5], and was mainly employed in three imaging modalities, including FC, SLO and OCT. Since then, it has achieved huge progress in the last ~25 years. Like the atmosphere, the human eye is optically imperfect: it suffers from wavefront aberrations whose pattern and amount differ between individuals. In ophthalmic medicine, AO is used to measure and correct the wavefront aberrations in the human eyes and optical systems through a closed-loop control (detection–control–correction), improving the lateral optical resolution from 10–15 μm to ~2 μm, enabling retinal imaging with cellular-level resolution [
6,
7,
8,
9,
10]. These improved images can help doctors to detect early retinopathy and fundus lesions, determine the cause and course of eye disease, and evaluate the subsequent treatment. The combination of AO and retinal imaging devices is of great significance and has the potential to become a general tool for the early and clinical detection and diagnosis of some retinal diseases.
2. Principles and Methods
2.1. Wavefront Aberration in Human Eyes
The human eye is mainly composed of the cornea, the anterior chamber, the lens, the vitreous body, the retina, etc. The retina is a light-sensitive layer with a sophisticated structure that lines the inner surface of the eye. This layer receives images coming through the eye’s lens and sends the processed signals along the optic nerve to the brain. Human eyes are not ideal refractive systems, and they are sensitive to the wavelength and intensity of light. When light enters the human eye, it produces chromatic and monochromatic aberrations. Chromatic aberrations can be overcome by using a single-wavelength light source. However, monochromatic aberrations are wavelength-independent and are affected by many complex factors, including variations in the shape of the tear film, cornea, and lens [
11]. Monochromatic aberrations are commonly divided into low-order and high-order aberrations. Low-order aberrations can be corrected using spherical and cylindrical lenses; but higher-order aberrations can significantly reduce lateral resolution and degrade retinal image quality with increasing pupil size of the human eye [
12,
13]. In daily life, people can see objects clearly because the human eye can limit the effect of aberration on vision by adjusting the size of the pupils. These wavefront aberrations usually limit the resolution of human eyes to ~10–15 μm, far from the theoretical lateral resolution of ~2 μm according to the diffraction limit formula,
r = 0.61
λ/
NA (
r is the resolution,
λ is the imaging wavelength, and
NA is the numerical aperture).
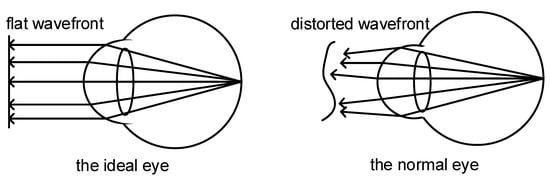
A comparison of wavefront shape between an ideal eye and a normal eye is shown in
Figure 1. In the ideal eye, the light reflected from the fundus forms a flat wavefront after passing through the normal refractive medium. The aberration in the normal eye causes the reflected light from the fundus to form a distorted wavefront, which limits the resolution of the conventional fundus imaging techniques [
6].
Figure 1. Schematic of wavefront shapes of ideal eye and normal eye.
2.2. Basic Principles of Adaptive Optics
The AO system is an automatic control system that typically comprises a wavefront sensor, a wavefront controller, and a wavefront corrector. By detecting, controlling, and correcting the optical wavefront in real time, the AO system can actively adapt to the changes of external condition and maintain a good working state [
14]. Modern AO retinal imaging systems can be divided into two types according to their different wavefront detection methods. One is based on geometric optics, wherein it uses wavefront sensors to directly measure the distorted wavefront, also known as the direct method. The corresponding AO system is referred to as hardware AO (HAO), which is usually composed of a wavefront sensor such as Shack-Hartmann wavefront sensor (SHWS), a compensator such as deformation mirror (DM) or liquid crystal spatial light modulator (LC-SLM), and the closed-loop control software between them. The direct method has the merits of high correction speed and detection accuracy, but it suffers from hardware complexity and high cost, relatively low spatial resolution, and limited dynamic range; moreover, a good “guide star” is necessary for the samples. The other is based on the iterative algorithm to indirectly deduce the wavefront through a series of images, also known as the indirect method, including sensorless AO (SAO) and computational AO (CAO) [
8]. The indirect methods do not need an additional wavefront sensor, so the optical system is greatly simplified; their major disadvantage is their low speed (seconds to minutes) due to the collection of many images [
15], leading to at least 10× slower speed compared to direct method (milliseconds).
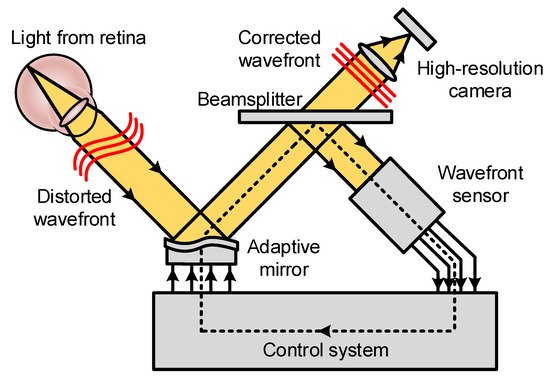
Figure 2 shows the schematic diagram of a sensor-based AO system for retinal imaging [
7,
16]. Light focuses on the retina after passing through the cornea, lens, vitreous body, and other eyeball tissues. The reflected light from the retina passes through the cornea again and forms a distorted wavefront. A wavefront sensor is used to record the ocular wavefront aberrations and calculate the distortion degree. Then, the wavefront aberration is transmitted to the wavefront controller and converted to a control signal. This signal drives the adaptive mirror to produce the corresponding deformation for the correction of distorted wavefront. Finally, the corrected flat wavefront is acquired, and the high-resolution image is acquired by a CCD camera. Sensor-based AO is optimized for a single depth within the sample and is sensitive to system misalignment, irregularly shaped pupils, cloudy corneas, or other ocular opacities may obscure the detection of the ocular aberrations.
Figure 2. Schematic diagram of a sensor-based AO system for retinal imaging (Adapted with permission from Ref. [
16]. Copyright 2011, Association for Research in Vision and Ophthalmology).
2.3. Sensorless AO and Computational AO
Compared with HAO, which uses a wavefront sensor and wavefront shaping device for wavefront aberrations correction, SAO eliminates a wavefront sensor and uses the properties of the image itself to estimate the wavefront quality [
17,
18,
19,
20,
21]; CAO eliminates both the wavefront sensor and wavefront shaping, further omits the need to iterate a control algorithm while imaging, and modifies the phase of the data to correct optical aberrations [
22,
23,
24,
25]. Both SAO and CAO exploit optimization algorithms for aberration correction, which reduces the complexity and cost of the AO system and offers versatility at the expense of wavefront correction speed. Meanwhile, they require image stability or phase stability during the collection time.
Many SAO control algorithms and image quality metrics have been described and evaluated [
18,
26,
27,
28,
29,
30,
31]. They can mainly be divided into two categories according to operating principle. One is to seek the optimum solution (control voltages or aberration modes) in line with desired system metrics from the numerous solutions (mostly random); the other is to seek the analytic relation between system metrics and the aberrations to attain the approximate solutions [
18]. A stochastic parallel gradient descent (SPGD) algorithm was used in SAO-SLO for retinal imaging [
17]. Moreover, a lot of retinal tracking and image registration algorithms were applied in the AO-SLO (see
Section 3.2.5). SAO-OCT retinal imaging was demonstrated by the implementations of SPGD [
20], coordinated search (CS) algorithm [
19,
32], hill climbing algorithm [
33], and data-based online nonlinear extremum-seeker (DONE) algorithm [
34], etc. Recently, some deep learning methods [
35], such as deep reinforcement learning [
36,
37] and convolutional neural networks (CNNs) [
38,
39], have been applied in SAO systems in combination with SLO or OCT. Many of these features and aberration correction algorithms used in SAO could be implemented in CAO [
40]. For example, an SPGD algorithm was introduced into CAO-OCT for automated fast computational aberration correction [
40].
This entry is adapted from the peer-reviewed paper 10.3390/photonics9050288