Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Subjects:
Oncology
Colorectal cancer (CRC) is a common cause of cancer and cancer-related death. Surgery is the only curative modality. Fluorescence-enhanced visualization of CRC with targeted fluorescent probes that can delineate boundaries and target tumor-specific biomarkers can increase rates of curative resection. Approaches to enhancing visualization of the tumor-to-normal tissue interface are active areas of investigation.
- tumor-specific antibodies
- fluorescent dyes
- tumor-specific labeling
- fluorescence-guided surgery
1. Introduction
Colorectal cancer (CRC) is a common cause of cancer and cancer-related death. Surgery is the only curative modality. Traditional approaches to localize and confirm complete resection during surgery are: preoperative cross-sectional imaging, identification of anatomic boundaries, palpation of the lesion, clinical judgment, and frozen sections if the degree of suspicion is high. However, this traditional approach can be subject to detection and sampling errors, which can leave behind positive margins. These traditional approaches become even more challenging in the setting of neoadjuvant chemotherapy and radiation, as scarring and fibrosis can mask viable tumors. Fluorescence imaging can enhance the delineation of the tumor-to-normal tissue interface. Tumor-specific antibodies tagged with fluorophores can provide real-time in situ imaging. These adjuncts to traditional approaches during surgery can further enhance detection and potentially increase rates of curative resection.
2. Impact of Margin Positivity on Colorectal Cancer and the Potential of Fluorescence Guidance
CRC is one of the most commonly diagnosed cancers. With 1.9 million new cases of colorectal cancer in 2020 causing 940,000 deaths, it is the second most common cause of cancer-related deaths worldwide [1]. In the United States, it is the third most common cause of cancer and cancer-related death [2]. While advances in systemic therapies have improved outcomes for patients with advanced colorectal cancer, surgery remains the mainstay of curative-intent treatment in early stages.
Complete resection with negative margins is the primary aim of oncologic surgery. For colon cancer, this involves removal of the colon segment containing the tumor, its affected vascular pedicle, and the lymphatic drainage basin of the affected segment [3]. However, this remains challenging, as the traditional intraoperative methods of visual inspection and palpation to assess margin negativity are highly subjective. Further assessments via intraoperative pathologic frozen sections are time-consuming and can be affected by sampling error, as there is a large surface area to sample from. This can be further exacerbated by the trend towards minimally invasive resections for colorectal cancer and the trend towards total neoadjuvant therapy. While the minimally invasive approach can enhance visualization with magnification, it is a narrower field of view, and the approach limits the traditional approach of palpation and assessment relies primarily on visual cues. With neoadjuvant therapies, areas of scarring and fibrosis can be indistinguishable from cancer. Viewing with the naked eye under white light is often insufficient to detect contrast between cancer and normal tissue, especially because tumors can often have similar color and texture to those of adjacent tissue.
Positive margins and early recurrence rates are indicators that residual tumor was left behind at the time of surgery. In a population analysis of 1.2 million patients from the National Cancer Database, Orosco et al. reported that up to 83,241 patients (6.8%) had positive surgical margins [4]. The rate is even higher for rectal cancer. Even after adopting the total mesorectal excision (TME) approach along with effective multimodal therapies, the rates of positive margins were still as high, from 17–22% [5,6,7]. Patients with positive surgical margins had a local recurrence rate of 22%, compared with 4% of those with negative margins [8]. In a large meta-analysis examining over 17,000 patients with rectal cancer, Quirke et al. showed that positive or close circumferential margins (less than 1 mm) were strong predictors of local recurrence (HR 6.3, 95% CI 3.7–16.7 with no neoadjuvant therapy and HR 2.0, 95% CI 1.4–2.9), distant metastases (HR 2.8, 95% CI 1.9–4.3), and survival (HR 1.7, 95% CI 1.3–2.3) [9]. Additionally, when neoadjuvant therapy was used, positive margins had an even greater association with recurrence (HR 6.3, 95% CI 3.7–16.7), indicating the lack of reliability using bright-light visualization and palpation in a pretreated field.
In metastatic CRC, margins matter even more. Liver metastases from CRC (CLM) are seen in one-third of patients, and margin-negative resection is still the only potentially curative option [10]. Vandeweyer et al. showed that in patients with stage 4 CRC with isolated liver metastases amenable to resection, there was a difference in the 5-year overall survival of 25% vs. 43% (p < 0.04) when resection margins were less than 1 mm compared to resection margins greater than 1 mm [11].
Fluorescence labeling of tumors allows surgeons to better delineate anatomic structures in real time, as there is immediate feedback while the tissue is being manipulated. Fluorescence-guided surgery (FGS) does not use ionizing radiation or bulky specialized equipment (i.e., intraoperative ultrasound, CT or MRI), and has direct visual concordance with the surgical field. Additionally, in oncologic surgeries, a targeted probe can provide additional information on the molecular characteristics of the tumor. FGS can potentially be used during all colorectal surgeries, especially for deep or locally-aggressive colon cancers, rectal cancers, cancers after neoadjuvant treatment, and cancers where an organ-sparing approach is being utilized (i.e., submucosal or full-thickness resections). The technology can be focused on the primary tumor, lymph node spread, detection of peritoneal disease, liver metastases, or surveillance of the resection bed or on identifying areas where further microscopic pathologic analysis is necessary.
Intraoperatively, fluorescence imaging can be performed as a diagnostic laparoscopy to detect the primary tumor and or peritoneal/liver metastases. Once the surgery is underway, fluorescence imaging can be utilized periodically to better define the location of the tumor in relation to surrounding tissue and anatomic structures. This can be performed in a minimally invasive fashion with fluorescence-capable laparoscopes or in a traditional open laparotomy with hand-held devices. Fluorescence imaging can potentially be used to detect lymphatic drainage, although this can be impaired due to the depth of overlying tissue in patients with obesity and thickened fatty mesentery. After the specimen is removed, fluorescence imaging can be performed on both the surgical bed and the specimen to ensure complete tumor removal and an adequate rim of normal tissue or mesorectal envelope.
Fluorescence labeling to improve cancer detection can also be applicable to endoscopy, the primary prevention strategy for reducing overall mortality from CRC. Along with the increased availability of fluorescence-enabled laparoscopes, endoscopes with fluorescence capabilities are being developed. Similar to surgery, endoscopy faces the challenges of detecting a lesion from a large surface area and limited contrast with standard white light. Tandem colonoscopy, a method in which two same-day colonoscopies are performed on a patient, is the most reliable approach for investigating the adenoma miss rate (AMR). Tandem studies have shown that the miss rate of total polyps is as high as 22%, indicating an additional field in which fluorescence can improve disease detection in CRC [12]. Fluorescence can improve the detection rate of CRC from adenomas and provide further information to care for patients in whom a watch-and-wait approach is being used after neoadjuvant treatment.
3. Principles of Fluorescence and Intraoperative Fluorescence Imaging
The use of fluorescence to highlight cancer can potentially mitigate the miss rate of CRC in both colonoscopies and surgery. Fluorescence occurs when a molecule that has absorbed light of a shorter wavelength (higher photon energy) and emits light of a longer wavelength (lower photon energy) [13]. This fluorescence can occur endogenously or be administered exogenously with a fluorescent dye or targeted probe.
Endogenous fluorescence naturally occurring within the tissue by molecules such as heme, porphyrins, NADH, FAD, collagen, or elastin. These molecules emit signals in the visible spectrum (400–700 nm) [14]. Attempts to distinguish between tumor and normal tissue using endogenous tissue autofluorescence have been successful in parathyroid surgery, and this is an active area of study in fluorescence-guided endocrine surgery [15]. With regard to CRC and other solid GI malignancies, endogenous fluorescence signals for tissue discrimination between normal tissue and cancer have been explored, but have not been incorporated into routine clinical use [14].
Administration of exogenous fluorescence contrast can further enhance the difference between abnormal tissue such that the signal is feasible for use in surgical navigation. When using exogenous fluorescence agents, a near-infrared wavelength (NIR) in the 700–900 nm range has been preferred since overlapping nonspecific fluorescence from endogenous fluorophores is eliminated and light scattering or tissue quenching of the desired signal is decreased [16]. Using wavelengths in the NIR range allows for increased tissue depth penetration and an improved signal-to-noise ratio compared to fluorophores in the visible spectrum [17].
4. Non-Targeted Fluorescence Agents
Exogenous fluorescence agents can be targeted or non-targeted. Non-targeted NIR agents include dyes such as 5-aminolevulinic acid (5-ALA), methylene blue, and indocyanine green (ICG), all of which are FDA approved. It is hypothesized that there is preferential tumor accumulation of these nonspecific dyes through an enhanced permeability and retention effect [18,19]. These dyes are localized and retained in tumors due to defects in their endothelium rather than tumor-specific ligand–receptor-mediated mechanisms [20].
5-ALA is a semi-selective dye, as its metabolite, protoporphyrin IX, is preferentially retained in cancer cells due to their deficient ferrochelatase activity [21]. It is orally administered and has been widely used in neurosurgery [22]. It was evaluated during diagnostic laparoscopy to detect peritoneal disease by Kondo et al., and a fluorescence signal was seen in peritoneal surface lesions in 8 of 12 patients (66.7%) [23]. 5-ALA was evaluated in a larger trial for the identification of metastatic CRC in lymph nodes during surgery, but it had limited ability to demonstrate fluorescence in the primary tumor (35.3% in cohort 1 and 33.3% in cohort 2) with poor sensitivity and limited specificity for the detection of lymph nodes (sensitivity cohort 1 = 11.1%, cohort 2 = 0%) (specificity cohort 1 = 75%, cohort 2 = 75%) [24].
Methylene blue is commonly used as a visually-detectable dye for sentinel lymph node detection [25], but when delivered at lower doses and imaged with an NIR system, methylene blue emits fluorescence in the 660 nm range. As the molecule is renally eliminated, it has been used to image ureters during colorectal surgeries [26,27]. As a direct tumor-labeling agent, it has been explored for use in breast cancer but not for the direct labeling of CRC [28,29].
Indocyanine green (ICG) is a nonspecific, hepatically-metabolized dye that was initially developed in the 1950s for retinal angiography, cardiac function, and hepatic function testing [30]. It is now the most commonly used molecule in the field of fluorescence-guided surgery and has gained widespread popularity for a wide variety of NIR fluorescence applications. ICG has been used at varying doses and schedules to image a wide array of anatomic structures: the biliary tree, soft tissue flaps, blood vessels, ureters, lymphatic vessels, lymph nodes, and tumors [31]. Within colorectal surgery, ICG has most frequently been used to evaluate the perfusion of anastomoses, and meta-analyses showed that the use of fluorescence angiography decreased anastomotic leaks, especially in lower rectal anastomoses [32,33,34].
ICG is less commonly used to label tumors since a specific molecular target is preferred, but several studies have evaluated ICG tumor-labeling. ICG is FDA approved, in contrast to other molecularly targeted agents, which are only available through clinical trials. Several Japanese groups have reported case series with direct endoscopic injection of ICG in the CRC prior to intraoperative imaging, with reasonable success at visualizing the tumor [35,36,37]. The limitations of this approach, beyond the need for a separate endoscopy for injection, are that mucosal injections of ICG may not be visible from the serosal side during surgery, especially if there is a high degree of intraabdominal obesity, and that there tends to be local diffusion of the molecule and a lack of contrast between the surrounding tissue and the primary lesion.
Systemic administration of ICG over time leads to preferential ICG accumulation in not just the primary tumor but also any peritoneal metastases. Cao et al. evaluated a series of 11 patients undergoing surgery for CRC who received 25 mg of ICG intravenously, and they evaluated the fluorescence signal at the tumor at a variety of time points [38]. There were 10/11 (91%) tumors with positive fluorescence and an optimal tumor-to-background ratio (TBR) of 1.9–2.2 at 2–4 h after injection. There was fluorescence in 38/40 (95%) lymph nodes evaluated. In one patient, additional nodules were detected only by ICG fluorescence. ICG has been used to evaluate peritoneal carcinomatosis from CRC by three groups. Liberale and Lieto et al. both used a weight-based dose of 0.25 mg/kg of ICG during surgery and showed fluorescence positivity in malignant nodules with a good sensitivity of 87.5–96.9% and specificity of 75–100% [39,40]. Barabino et al. used a similar dose in patients with peritoneal carcinomatosis 24 h prior to surgery and found lower sensitivity and specificity of 72.4% and 60.0%, respectively which suggests that 24 h after a lower dose of ICG may be insufficient for optimal fluorescence enhancement. This is in comparison to the “second window” use of ICG, where larger amounts of the dye (5 mg/kg) are administered intravenously and imaged after 24 h. This approach has been useful for delineating a number of tumors including tumors in the pancreas [41], lung [41,42], brain [43,44], and prostate [45]. High dose ICG labeling was reported as feasible in one case report of a patient with pulmonary CRC metastasis, but this approach has not been used for direct labeling of CRC [46].
5. Targeted Fluorescence Agents
While these non-targeted dyes are easily accessible because they are FDA approved, tumor-specific agents are appealing due to their ability to tailor the probe to specific targets and their ability to provide additional information on the molecular characteristics of the tumor. Molecular specificity can be conferred through several different classes of tumor-targeting probes such as antibodies, antibody fragments, and nanobodies (Figure 1) [47]. Other probes include protein scaffolds, aptamers, peptides, small molecules, and nanoparticles.
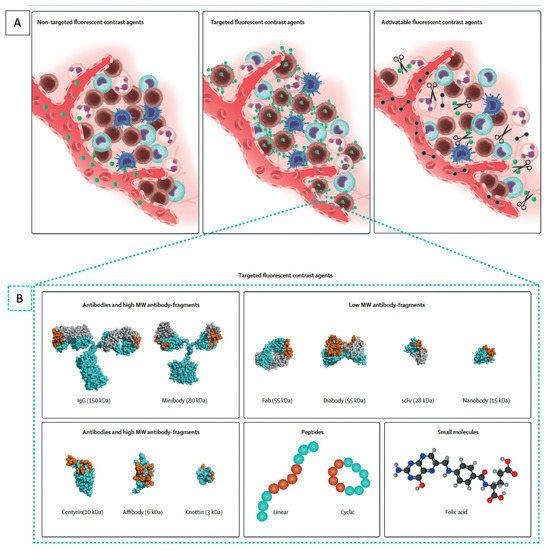
Figure 1. Molecular fluorescent contrast agents and targeting moieties used for intraoperative imaging during cancer surgery. (A) Schematic representation of the mode of action of the different types of fluorescent contrast agents. Non-targeted fluorescent contrast agents such as indocyanine green passively accumulate in tumor tissue via the enhanced permeability and retention effect. Targeted fluorescent contrast agents, consisting of a fluorescent dye conjugated to a targeting moiety, actively accumulate in tumor tissue by recognizing a specific biomarker expressed by tumor cells or tumor-associated stromal cells. Imaging is performed once unbound tracers have been cleared sufficiently. Activatable fluorescent contrast agents remain optically silent until fluorescent dyes are released by enzymatic digestion of their backbone. (B) Schematic representation of the different classes and subclasses of targeting moieties used for the design of targeted fluorescent contrast agents: antibodies, antibody fragments, protein scaffolds, peptides, and small molecules. Representative space-filling images of an antibody (1IGT), Fab fragment (6B9Z), diabody (1MOE), scFv (1P4I), nanobody (5MY6), centyrin (5L2H), affibody (2KZJ), and knottin (2N8B) were obtained from the RCSB protein bank and prepared using PyMOL. The space-filling minibody model is an interpretation created using PyMOL; antigen-binding regions are highlighted in orange. Adapted from Hernot et al. [48].
Antibodies are the traditional and most commonly used approach for tumor targeting since they have been developed against a wide variety of targets, are easily modifiable, and can be produced in large amounts. Antibodies are the focus of a long and broad body of literature, including clinical studies for drug delivery and radionuclide studies [49]. They can easily be conjugated to fluorophores to act as molecular tracers for intraoperative imaging. Antibodies can be fragmented into smaller molecules that maintain their antigen-binding properties, such as diabodies or minibodies, but they have not gained popularity for clinical use, as the fragments were unstable and difficult to optimize for larger production [50,51,52]. Smaller molecules can be advantageous, as they are able to provide higher contrast at earlier time points compared to intact antibodies. This avoids the need for patients to have a separate clinical visit to receive the tracers, and the molecule can be administered on the same day of surgery. However, the disadvantage with smaller molecules is that they can have a decreased overall tumor signal due to rapid renal elimination and the decreased number of overall fluorophores that can be conjugated. Molecules smaller than 60 kDa are renally filtered, resulting in more rapid blood clearance and leaving decreased time for target binding. A newer class of biological targeting molecules for FGS are the monomeric antigen-binding domains of heavy-chain-only antibodies, also known as single-domain antibodies (sdAbs) or nanobodies [53]. They are advantageous because they can be produced in animal, yeast, or bacterial cells and have high thermal and chemical stability for molecular conjugations and are promising for FGS [54].
Non-antibody-based platforms for conferring tumor specificity include protein scaffolds. This class of molecules, also known as antibody mimetics, can bind antigens but are not structurally related to antibodies [55]. Molecules in this class have similar backbone structures, have high protein folding stability, and can be easily and cost-effectively produced in bacterial hosts. They include molecules such as affibodies, adnectins, DARPins (designed ankyrin repeat proteins), centyrins, and knottins, among many others [56]. Identification of binding partners occurs via high-throughput screening against a peptide library [57]. While many are being actively explored for therapeutic uses, relatively few studies have been performed for intraoperative molecular imaging. Other drawbacks are the same as those of other small molecules: rapid renal clearance and limited fluorophore conjugation. Antibody mimetics have promising potential as therapeutic agents, and there is increasing interest in using these molecules as probes for FGS [58].
Aptamers are single-strand nucleotide-based molecules with a three-dimensional structure that enables specific target binding. Similar to protein scaffolds, binding partners are identified through an iterative selection process termed systematic evolution of ligands by exponential enrichment (SELEX) [59]. These molecules are generated with efficiency using a solid-phase oligonucleotide synthesis, have excellent biochemical stability, and are internalized by target cells. The limitations of aptamers are similar to those of other small molecules, but an additional major limitation is that aptamers are degraded in-vivo by endogenous nucleases and immune detection by toll-like receptors [60]. Chemical modifications are being investigated to overcome these limitations, and aptamers are also beginning to be investigated for FGS.
Other classes of tumor-targeting molecules are peptides and nanoparticles. These molecules form a heterogeneous group, as their structures and biochemical properties are variable, and they do not share a common backbone. These include protease-activatable peptides that contain a quencher that is cleaved off upon activation with proteases, which are upregulated in tumors [61]. Other peptides bind to naturally occurring motifs on molecules upregulated in cancer, such as integrins or folate receptors [47]. Nanoparticles are very small molecules, usually 1–100 nanometers in diameter, with efficient cell penetration. They have highly versatile structures for encapsulating fluorescent molecules and can be linked with tumor-targeting moieties for FGS [62].
6. Molecular Targets for CRC
There are a large number of molecular targets suitable for therapeutic targeting of CRC and drug development, but biomarkers appropriate for tumor-specific imaging have slightly different characteristics.
Biomarkers suitable for tumor targeting were systematically described by van Oosten et al. in 2011 by the Target Selection Criteria (TASC) scoring system [63]. Potential molecular targets are ranked for tumor-specific imaging by the following characteristics, which make them ideal for FGS. The most important features are as follows: (1) The target must be present on the cell surface or be in close proximity to the tumor cell, making it accessible to the fluorescent probe. (2) The target must be upregulated by most cancer cells within the tumor. (3) Expression of the target should be minimal in normal tissue such that the tumor-to-normal ratio is greater than 10. (4) The target is present at a high frequency in the population of patients with CRC. Other characteristics, such as the previous use of this biomarker for in vivo imaging studies, the presence of enzymatic activity in and around the tumor, and the presence of internalization of the probe-target complex, are other features that were also ranked.
Using this system, the group identified the following targets for optimal development in FGS of CRC: human carcinoembryonic antigen (CEA), CXC chemokine receptor 4 (CXCR4), epidermal growth factor receptor (EGFR), epithelial cell adhesion molecule (EpCAM), matrix metalloproteases 1, 2, 3, 7, and 9 (MMPs), Muc 1, and vascular epithelial growth factor-A (VEGF-A). Targets such as CEA, EGFR, EpCAM, MUC1, and VEGF were also highlighted as promising tumor-associated targets by the National Cancer Institute [64].
This entry is adapted from the peer-reviewed paper 10.3390/cells11020249
This entry is offline, you can click here to edit this entry!