According to the American Cancer Society, approximately 53,000 new cases of thyroid cancer were diagnosed and more than 2200 people died from the disease in 2020. New developments in molecular imaging are significantly improving thyroid cancer diagnostics and therapy. Continuous research in molecular imaging techniques additionally contributes to an understanding of a variety of diseases and enables more efficient care of thyroid cancer patients. Molecular imaging-based personalized therapy has been a fascinating concept for individualized therapeutic strategy, which is able to attain the highest efficacy and reduce adverse effects in certain patients. Theragnostics, which integrates diagnostic testing to detect molecular targets for particular therapeutic modalities, is one of the key technologies that contributes to the success of personalized medicine.
- molecular imaging
- theragnostics
- thyroid cancer
1. Diagnosis of Differentiated Thyroid Cancers
1.1. Molecular Imaging of Thyroid Nodules
1.1.1. [99mTc]Tc-MIBI Thyroid Scintigraphy
1.1.2. [18F]FDG Positron Emission Tomography/Computed Tomography
| Method | Tracer | Indication | Pattern | Action |
|---|---|---|---|---|
| Scintigraphy | Na[99mTc]TcO4 | nodules-low TSH | AFTNs | Avoid FNA |
| Scintigraphy | Na[123I]I | nodules-low TSH | AFTNs | Avoid FNA |
| Scintigraphy | [99mTc]Tc-MIBI | nodules-CI | [99mTc]Tc-MIBI- | Avoid surgery |
| PET/CT | [18F]FDG | nodules-CI | [18F]FDG- | Avoid surgery |
2. Differentiated Thyroid Cancers
2.1. Surgical Treatment for DTC and Preoperative Staging
2.2. Postoperative 131I Therapy
-
Remnant ablation to eliminate normal thyroid tissue remnants in low risk patients, thereby ensuring undetectable or minimal serum Tg levels (in the absence of neoplastic tissue), which facilitates follow-up.
-
Adjuvant treatment to irradiate suspected but unproven sites of neoplastic cells in low-intermediate and intermediate risk patients, as determined by histopathologic features, thereby reducing the risk of disease recurrence.
-
Treatment of known disease to treat persistent or recurrent disease in patients with demonstrated metastatic disease.
2.3. The Role of Functional Imaging in Managing Radioiodine Therapy
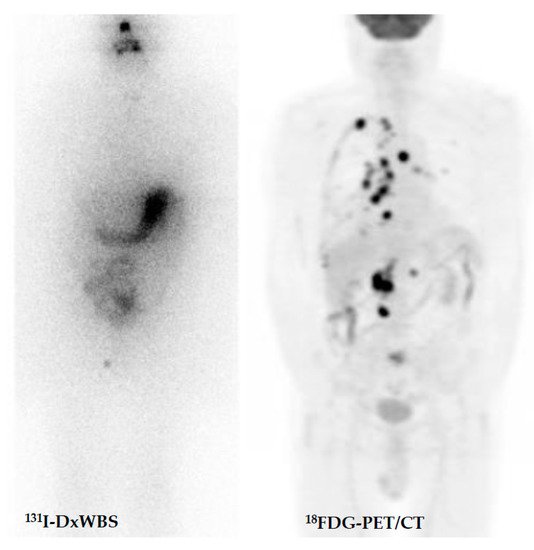
2.3.1. Post-Therapy Whole-Body Scintigraphy (TxWBS)
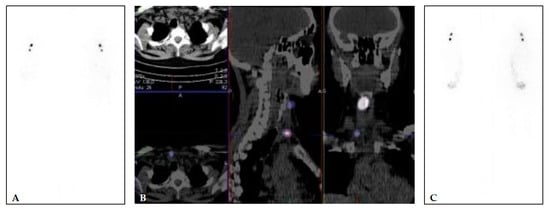
2.3.2. Postoperative Diagnostic Whole-Body Scintigraphy (DxWBS)
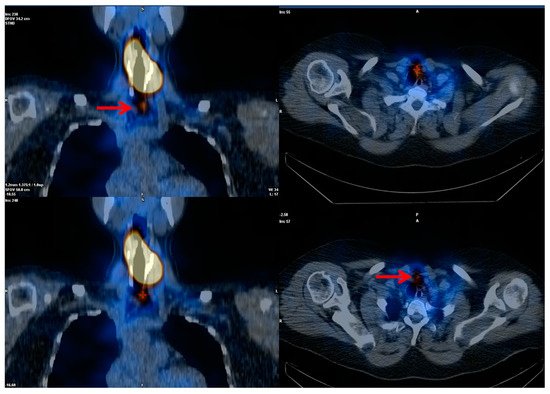

2.3.3. [18F]FDG Positron Emission Tomography/Computed Tomography (PET/CT)
2.4. The Role of Functional Imaging in Response Assessment and Disease Monitoring
2.4.1. Radiodine Whole Body Scintigraphy
2.4.2. Positron Emission Tomography
This entry is adapted from the peer-reviewed paper 10.3390/cancers14051272