2. Cannabis, Flos
To date, a monograph of the drug “Cannabis, flos” is not available in the European Pharmacopoeia but it is largely followed by the one in German Pharmacopoeia, where it is defined as “dried shoot apices of female Cannabis sativa L. (Cannabaceae) plants. The drug contains not less than 90.0 and not more than 110.0 percent of cannabinoid quantities indicated in the label, such as ∆9-tetrahydrocannabinol and cannabidiol, as well as cannabinoid-carbon acids, such as ∆9-tetrahydrocannabinolic acid and cannabidiolic acid, calculated as ∆9-tetrahydrocannabinol (C21H30O2; Mr 314.5) and cannabidiol (C21H30O2; Mr 314.5), referenced to dried drug”
[10].
Cannabis is a dioecious annual plant
[3] (p. 304) that belongs to the Cannabaceae family, which includes about 170 species
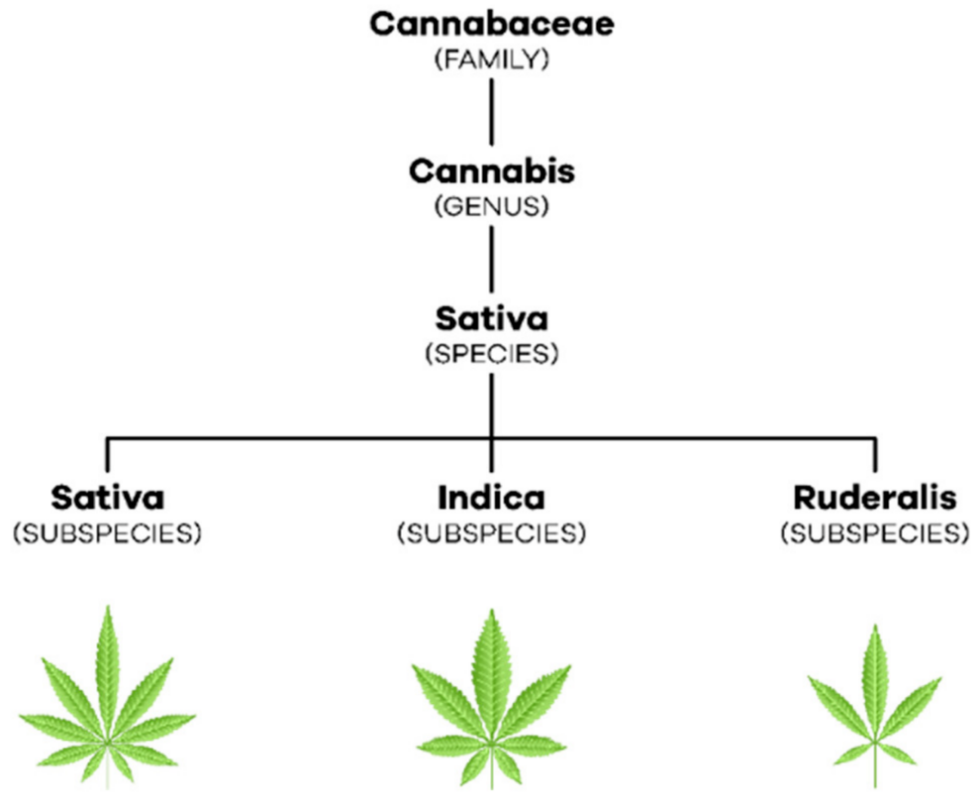
[11] (pp. 203–204). With regard to taxonomy, in 1753, Linnaeus began by describing only one species of this plant, Cannabis sativa. Later, in 1785, Lamarck considered the existence of two species of cannabis, Cannabis sativa, which came from the West, and Cannabis indica, which came from India, Southeast Asia, and Southern Africa (
[2][11] (p. 236), (pp. 207–208)). Only in the 19th century emerged the reference to a new species of cannabis, Cannabis ruderalis
[2] (p. 236). Currently, most authors consider that there is only one species,
C. sativa L., which comprises three subspecies,
C. sativa subsp. sativa,
C. sativa subsp.
indica and
C. sativa subsp.
ruderalis [12] (p. 3) (
Figure 1). C. sativa subsp. sativa is a tall, branched plant that can reach more than five meters in height, it produces a large amount of THC relative to CBD and its terpenoid profile gives it a sweet smell. Furthermore,
C. sativa subsp. indica, which has wider leaves, only reaches one to two meters in height, produces a similar amount of THC and CBD and its terpenoid profile causes it to have a bitter odor.
C. sativa subsp.
ruderalis is the smallest plant reaching only one meter in height and producing the least amount of cannabinoids (
[11][13] (p. 208), (p. S2)).
Figure 1. Taxonomic organization of C. sativa L.
The drug consists of the flowers of
C. sativa L. female plants, because they have more glandular trichomes that accumulate in their interior secondary metabolites responsible for the studied bioactivities, namely phytocannabinoids and terpenoids (
[1][3] (p. 413), (p. 304)). The content of these compounds is influenced by environmental conditions like temperature, humidity, presence of pests, and soil composition. Terpenoids are responsible for the characteristic smell of the plant, while phytocannabinoids are defense agents and responsible for the interaction with other species, whether animal or plant
[3] (p. 305). However, for medicinal use, the plant’s growing conditions comply with specific guidelines covered by the current legislation in order to produce plants always with the same characteristics and totally free of contaminants, from the soil and from the environment
[14] (pp. 1–11).
3. Endocannabinoid System
The endocannabinoid system is involved in the organism’s homeostasis
[1] (p.413) through the modulation of multiple organs comprising the cardiovascular (CVS), central nervous (CNS), peripheral nervous (PNS), endocrine, reproductive, immune and digestive systems (
[15][16] (p. 2) (p. 554)).
3.1. Cannabinoid Receptors
The two main receptors of the endocannabinoid system are the cannabinoid receptor type 1 (CB1), encoded by the CNR1 gene which is made with 472 amino acids, and the cannabinoid receptor type 2 (CB2), encoded by the CNR2 gel and composed of 360 amino acids
[17] (p. 2). Both are G protein-coupled metabotropic receptors (
[18][19] (p. 2), (p. 3)) and their expression varies depending on the body region
[16] (p. 559).
The CB1 receptor is found mainly in CNS neurons with high expression density in the basal ganglia, cerebral cortex, hippocampus, and cerebellum
[17] (p. 5). Thus, it is involved in motor control, cognitive functions, movement coordination, learning, and memory. It is also expressed in PNS and peripheral tissues, namely, in sympathetic nerve terminals, gastrointestinal tract, lungs, musculoskeletal tissue, reproductive and immune system, among others
[16] (p. 559). Furthermore, its hepatic and cardiovascular expression increases in the presence of pathological conditions
[17] (p. 5).
In turn, the CB2 receptor is mostly found in peripheral cells of the immune system
[20] (p. 1140) such as the spleen, tonsils, and thymus
[16] (p. 559). It is also expressed in lower concentrations in the pancreas, liver, bone marrow, bones, and skin
[21] (p. 3). At the cerebral level, it is found in low amounts, however, in inflammatory states, its expression increases both in microglia and in other glial cells
[3] (p. 309).
3.2. Endocannabinoids
The most studied endocannabinoids are N-arachidonylethanolamine or anandamide (AEA) and 2-arachidonylglycerol (2-AG)
[3] (p. 308). AEA is known to be a high-affinity partial agonist for the CB1 receptor and with very low affinity for the CB2 receptor, while 2-AG is a full agonist with low to moderate affinity for the two cannabinoid receptors
[17] (p. 2).
Neurotransmission in the postsynaptic neuron leads to an increase in intracellular calcium and, consequently, to the production of endocannabinoids from their lipid precursors
[22] (p. 4). AEA is produced from N-acyl-phosphatidylethanolamine (NAPE) by N-acyl-phosphatidylethanolamine-specific phospholipase D (NAPE-PLD) while 2-AG is formed from diacylglycerol (DAG) by diacylglycerol lipase (DAGL)
[19] (p. 3). As lipid molecules, they are able to cross the plasma membrane and travel in a retrograde direction to the presynaptic terminals
[17] (p. 4). There, the endocannabinoids bind and activate cannabinoid receptors, which, in turn, inhibit the adenylate cyclase (AC) enzyme, decreasing the formation of cyclic adenosine monophosphate (cAMP) and the activation of protein kinase A (PKA)
[18] (pp. 2–3). Thus, hyperpolarization occurs by opening potassium channels, the consequent closure of calcium channels, and the release of neurotransmitters ceases
[22] (p. 4). The endocannabinoids get retaken by the membrane transporter of endocannabinoids and then hydrolyzed by the respective enzymes
[23] (pp. 2–3). AEA is catabolized by fatty acid amide hydrolase (FAAH), giving rise to AA and ethanolamine while 2-AG is catabolized by monoacylglycerol lipase (MAGL) giving rise to AA and glycerol (
[3][22] (p. 308), (p. 4)) (
Figure 2).
Figure 2. Endocannabinoid signaling.
Moreover, the activation of cannabinoid receptors increases the activity of mitogen-activated protein kinase (MAPK) associated with the control of synaptic plasticity, cell migration, and neuronal growth. Additionally, within intracellular compartments, researchers find cannabinoid receptors, such as in mitochondria, which, when activated, are capable of modifying levels of reactive oxygen species, calcium, and adenosine triphosphate (ATP)
[22] (p. 4).
3.3. Phytocannabinoids
Phytocannabinoids are biosynthesized in
C. sativa L. and, currently, there are more than 100 phytocannabinoids identified among the more than 500 compounds discovered in this plant. Its distribution is variable but phytocannabinoids accumulate, in large quantities, in the trichomes present in female flowers as previously referred to in this text
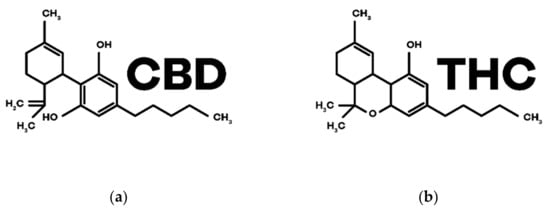
[3] (p. 305). Among them, THC and CBD are the most studied ones. The structures are in
Figure 3.
Figure 3. Chemical structures of the main phytocannabinoids in Cannabis sativa L.: (a) CBD; (b) THC.
CBD was the first phytocannabinoid to be isolated in its pure form, in 1899, by Thomas Hill Easterfild.
[24] (p. 922). Even though it does not have psychoactive properties, it has shown potential for various therapeutic effects and has been extensively investigated for the treatment of various pathologies
[25] (pp. 8–13). It is a negative allosteric modulator of CB1 and CB2 receptors and has the ability to inhibit the reuptake and degradation of the endocannabinoid AEA (
[3][4] (p. 306), (p. 6)). In addition, CBD interacts with other non-cannabinoid receptors such as serotonin (5-HT) receptors, orphan G protein-coupled receptors (GPCRs), adenosine A1 receptors, nuclear receptors activated by peroxisome proliferators type γ (PPARγs), transient receptors potential cation channel subfamily V member 1 (TRPV1s) and also α1 and α3 glycine receptors (
[26][27] (p. 4), (p. 1)).
THC, in turn, is the main component of the female flowers of
C. sativa L.
[28] (p. 1), being a partial agonist of the receptors CB1 (responsible for the psychoactive effects) and CB2 intervening in the immunological and anti-inflammatory effects
[3] (p. 307).
4. Physiological and Therapeutic Effects of Cannabinoids
The endocannabinoid system is associated with the balance of homeostasis and, as cannabinoids interact with this system, they have been studied, in recent decades, for the treatment of various pathologies (
Table 1) (
[29][30] (pp. 4–10), (pp. 183–186)). THC has greater bioactivity, although it is also known for the effects of euphoria, relaxation, and changes in sensory and temporal perception. In the case of CBD, and due to the pharmacological effects detailed above, it has been shown to be effective as an anticonvulsant, antipsychotic, anti-inflammatory, antioxidant, neuroprotective, and anxiolytic
[4] (p. 5).
Table 1. Summary of the therapeutic potential of cannabinoids in different diseases and symptoms.
| Diseases and Symptoms |
Therapeutic Potential of Cannabinoids |
| Alzheimer’s Disease |
Anti-inflammatory
Neuroprotector
Antioxidant |
| Parkinson’s Disease |
| Huntington’s Disease |
| Multiple Sclerosis |
Antispastic
Analgesic |
| Epilepsy |
Anticonvulsant |
| Tourette’s Syndrome |
Improvement of symptomatology |
| Cancer |
Analgesic
Antiemetic
Appetite stimulator
Antitumor |
| Glaucoma |
Intraocular pression reduction |
| Inflammatory Bowel Diseases |
Anti-inflammatory
Healing |
| Schizophrenia |
Antipsychotic |
| Sleep Disorders |
Decrease sleep latency and nocturnal awakenings
Sedative |
| Pain |
Analgesic |
| Post-Traumatic Stress Disorder |
Anxiolytic |
| Nausea and Vomiting |
Antiemetic |
| Anorexia |
Appetite stimulator |
These bioactivities lead, among the possible therapeutic applications, those involving neurodegenerative diseases characterized by a loss of neurons, which leads to a decline in motor and cognitive capacity. All this information is also associated with inflammation with a major role in the progression of the disease. Therefore, the properties that CBD exhibits at the level of neurodegeneration, inflammation, and antioxidation may come to be very important in the treatment and stabilization of these diseases, such as, for example, Alzheimer’s, Parkinson and Huntington’s
[25] (pp. 8–9).
Another complex pathology that benefits from the bioactivity of these compounds are multiple sclerosis, which is an autoimmune disease characterized by demyelination that occurs in CNS
[20] (p. 1143), leading to characteristic symptoms such as spasticity that causes severe pain and difficulty sleeping
[31] (p. 18). Cannabinoids are able to alleviate these symptoms through interaction with the CB1 receptor, reducing the massive release of glutamate, which leads to reduced spasticity, producing analgesic effects
[32] (p. 10).
The potential adjuvant therapy with cannabinoids, mainly with CBD, is also studied in epilepsy, but the mechanism of action is not yet fully understood
[33] (p. 397). However, the regulation of T-type calcium channels, as well as of PPARs by CBD, may be a possible mechanism, since both are associated with seizures
[22] (p. 5).
Moreover, in Tourette’s syndrome, which is a chronic neurological disease characterized by the presence of motor and vocal tics, there were improvements with the administration of cannabinoids
[31] (p. 22).
Another area that is much discussed is oncology, but it is more associated with supportive therapy, specifically to reduce some chemotherapy side effects. Effectively, there is already validation of efficacy and safety in pain relief, reduction of nausea and vomiting, and appetite stimulation, associated with chemotherapy and palliative care. THC is able to centrally antagonize 5-HT3 receptors, mediating an anti-emetic effect. It also can activate CB1 receptors, suspending the emetic effects triggered by serotonin and dopamine
[31] (pp. 19–20). THC has the ability to stimulate appetite through the activation of CB1 receptors located at the level of the hypothalamus and which are responsible for regulating the energy balance (
[32][34] (pp. 9–10), (p. 140)).
There is evidence that these compounds mediate antitumor effects by inhibiting cell proliferation, inducing autophagy-mediated apoptosis, and intervening in the migration, invasion, and metastasis of cancer cells. Thus, in the near future, can lead to the development of new drugs based on these cannabinoid structures, for instance, on CBD, which is an antagonist of GPCR 55 in various types of cancer (
[17][25][32] (pp. 11–12), (pp. 10–13), (p. 11)).
Another potential therapeutic application, for example for THC, is the treatment of increased pressure in the eyeball caused by glaucoma, which is an optic neuropathic disease, which leads to irreversible loss of vision
[28] (p. 1690).
With regard to inflammatory bowel diseases, such as Crohn’s disease and ulcerative colitis, it is known that CBD has the ability to slow down their progression and improve symptoms such as abdominal pain, diarrhea, and anorexia (
[31][34] (p. 21), (pp. 2–4)). In these situations, cannabinoids are able to promote an anti-inflammatory action by acting on CB2 receptors and wound healing acting on CB1 receptors
[3] (p. 310).
Another pathology very much associated with cannabinoids is schizophrenia. In this disease, changes occur at the level of the endocannabinoid system, increasing the expression of CB1 receptors. Here, CBD may have important antipsychotic potential as opposed to THC which induces psychosis
[31] (pp. 22–23).
With regard to sleep disorders, it is known that THC decreases sleep latency time as well as nocturnal awakenings. In turn, CBD in medium to high doses has a sedative effect, showing potential for the treatment of insomnia
[35] (pp. 9–10). Since CBD acts at the level of 5-HT1A receptors through which it plays anxiolytic and antidepressant effects, it can also contribute to stabilizing the sleep cycle
[33] (p. 397).
Finally, it is known that the endocannabinoid system is associated with pain control
[31] (p. 20). Thus, cannabinoids perform their analgesic effects through the activation of CB1 receptors
[3] (pp. 309–310).