Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Subjects:
Urology & Nephrology
Urological cancers, namely prostate, bladder, kidney, testicular, and penile cancers, are common conditions that constitute almost one-quarter of all malignant diseases in men. Urological cancers tend to affect older individuals, and their development is influenced by modifiable metabolic, behavioral, and environmental risk factors. Carotenoids may have cancer-fighting properties and protect against cancer development, slow its spread, and reduce the risk of cancer deaths in humans.
- prostate cancer
- carotenoids
1. Prostate Cancer
PCa is a common malignancy among men worldwide. In 2018, PCa was reported as the second most common noncutaneous cancer in men worldwide (an estimated 1.3 million new cases) and the fifth most common cause of cancer death in men. There is wide geographical diversity in its prevalence, with age-standardized rates (ASR) per 100,000 of 97.2 in the United States and less than 20 in Asia and developing countries [11]. The most common pathological type of PCa is acinar adenocarcinoma, which accounts for more than 99% of all prostate tumors [12]. Family history of PCa, older age, and race are the only undisputed risk factors for PCa development. Asian men have low PCa risk compared with men from the Western world. However, when Japanese men moved from Japan to California, their risk of PCa rose, approaching that of American men, which implied a role of dietary or environmental factors, possibly including dietary carotenoid intake as a contributing factor [13]. There have been a few proposed mechanisms through which carotenoids may act to reduce cancer development, as shown in Figure 1.
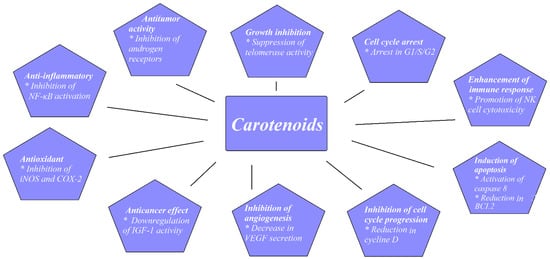
Figure 1. Proposed mechanisms for carotenoids preventing cancer development. Based on figures from Milani et al. [14].
1.1. Experimental Studies
The inhibition of PCa cell growth has been the subject of a number of experimental studies performed on the PCa cell cultures LNCap, DU145, and PC-3. The LNCaP cell line comes from a lymph node metastasis of human PCa; DU145 cells are derived from a brain metastasis of primary PCa; and the PC-3 cell line was established from a PCa bone metastasis from a 62-year-old male Caucasian. The growth-inhibitory effect of lycopene was compared with that of one of the main chemotherapeutic agents used to treat metastatic PCa, docetaxel. PCa cell growth was inhibited by 19–54% with docetaxel and by 5–24% with lycopene. A synergic effect of 78% growth reduction was also shown when combining docetaxel with lycopene [15,16]. A dose-dependent reduction in PCa cellular growth was shown with rising lycopene concentrations of up to 10 µM [17,18]. It may be suggested that the efficacy of lycopene depends on its source of origin. Lycopene extracts from algae (marine Chlorella) and from tomatoes were compared at concentrations of 20 and 50 µM. PCa cells’ viability was 10–18% lower after treatment with algae lycopene than after treatment with tomato lycopene at the same concentration, showing the better antiproliferative and apoptotic effect of algal lycopene [19]. Similarly, extracts from tomato paste, tomato sauce, ketchup, and tomato extract were compared on PCa cells that were obtained and cultured from prostates of patients submitted to radical prostatectomy. Cell growth reduction was highest for tomato paste, and then for ketchup, tomato sauce, and extract, with reductions in cellular growth of 54%, 51%, 47%, and 44%, respectively [20]. One must be cautious when interpreting cell-culture-based studies because there are differences between the concentrations of carotenoids in the body and those used in cell culture, with the latter usually being significantly higher. Concentrations of 1 µM and 0.5 µM of lycopene reduced cell proliferation of LNCaP cells; however, there was no effect observed at 0.25 µM [21]. Other studies have suggested that higher lycopene concentrations of around 1–1.25 µM lycopene are necessary for the antiproliferative effect [22]. Postmortem human studies showed that carotenoid concentrations in serum and individual organs were similar and that there was a correlation between intake and tissue/blood levels of carotenoids. The serum concentration of lycopene in plasma was around 740 nmol/kg, and that in prostate tissue was around 700 nmol/kg. These physiological concentrations may be at the edge of those that showed an antiproliferative effect in experimental studies.
Palozza et al. showed in an in vitro study on PCa cells that β-carotene acted as a growth-inhibitory agent by inhibiting AKT phosphorylation, which led to the increased expression of c-MYC and the activity of caspases. In the end, apoptosis was stimulated [23].
Furthermore, in another experimental animal study, Yang et al. subcutaneously implanted androgen-independent PCa (PC-3) cells in mice. Both lycopene and β-carotene, when supplemented to the mice, significantly inhibited tumor growth [24].
There have been few interesting studies, however, that have examined the impact of lycopene on PCa cells’ ability to spread and metastasize. Using PC3 and DU145 PCa cell lines, Elgass et al. showed that the adhesion of PCa cells to a basement membrane was significantly reduced at lycopene concentrations higher than 1.15 µM. There was also a reduction in PCa cellular motility and migration of 40% and 58% for PC3 cells and DU145 cells, respectively [25]. Some proteins known to be responsible for controlling the adhesion and migration of PC (namely intercellular adherence molecule 1 (ICAM1) and MMP9) were downregulated in PC-3 cell lines treated with tomato extract. These results indicate the ability of LC to diminish PCa’s metastatic abilities to some degree. The expression of proteins such as intracellular ICAM 1 and MMP9 was influenced by tomato extract and downregulated in PC3 cell lines [26]. This may suggest the potential ability of lycopene to reduce PCa spread.
1.2. Epidemiological Studies
It has been suggested that saturated fat consumption is linked to not only PCa incidence but PCa progression and mortality risk [27]. One of the key oncogenes in PCa tumorigenesis is c-MYC. It has been shown that increased fat consumption results in amplifying the MYC-dependent transcriptional cascade [28]. Blood lipids, and especially high lipoprotein A concentrations, seem to be associated with increased PCa risk and advanced disease [29], and lipoprotein A is known to promote inflammation. On the other hand, high levels of chronic inflammatory markers are associated with high-risk, aggressive PCa [30]. The well-established role of carotenoids as scavengers of reactive oxygen species and anti-inflammatory agents might contribute to PCa risk reduction [31].
High concentrations of carotenoids were identified in some vegetables consumed as part of a traditional Mediterranean diet [32]. There have been a few prospective cohort studies that found no protective association between Mediterranean diet prior to diagnosis and incidence of lethal or advanced PCa. However, an interesting observation was made that greater adherence to Mediterranean diet after the diagnosis of nonmetastatic PCa lead to 22% post-treatment reduction in overall mortality [33].
Hoang et al., in a case–control study with 652 participants, showed that PCa patients consumed significantly lower levels of carotenoids than controls (p < 0.05). In comparison with the highest versus the lowest tertile of lycopene or carrot and tomato intake, the odds ratios for PCa were 0.46 and 0.39, respectively. These correlations were true for low-, medium-, and high-grade PCa [34].
Antwi et al. found that higher dietary lycopene intake was associated with a decreased risk of having aggressive PCa. The odds ratio (OR) was 0.55 in the highest versus the lowest tertile after adjustment for multiple covariates. There were three groups of PCa defined in the study: highly aggressive PCa (Gleason sum ≥ 8 or PSA > 20 ng/mL or Gleason sum ≥ 7 and clinical stages T3–T4), low aggressive (Gleason sum < 7 and clinical stages T1–T2 and PSA < 10 ng/mL), and intermediate aggressive (all others). They also found that African-Americans, but not European-Americans, with higher β-cryptoxanthin dietary intake had 45% lower odds of aggressive PCa [4].
Because up to 80% of people develop some form of indolent PCa in their lives, it is more important for the urological community to look for factors associated with high-grade, clinically significant disease than to concentrate on any PCa. Cases are dominated by low-grade Gleason 6, mostly clinically nonsignificant disease. It seems that studies that included PCa patients diagnosed before the PSA-era with less indolent cancers reported more pronounced associations between carotenoid intake and PCa risk.
There seems to be more consistent evidence for a modest protective role for carotenoids against PCa progression than general incidence or initiation of the disease itself [35,36,37].
In general, the most robust evidence in the literature regarding the role of carotenoids in PCa has been associated with lycopene as a potent antioxidant. There have been three meta-analyses published in the literature on this topic, which are summarized in Table 1.
Table 1. Characteristics of meta-analyses assessing carotenoids’ effect on prostate cancer risk.
| Author | Number of Studies | Measure | Results |
|---|---|---|---|
| Chen et al., 2013 [38] | 17 studies; 6 cohort, 11 NCC | Effect of: Lycopene intake on risk of PCa Serum lycopene on risk of PCa Lycopene intake on risk of advanced PCa Serum lycopene on risk of advanced PCa |
Not significant Not significant Not significant Not significant |
| Wang et al., 2015 [39] | 34 studies; 10 cohort 11 NCC 13 CC |
Effect of: α-carotene, β-carotene, lycopene intake on PCa α-carotene, β-carotene, lycopene blood concentrations on PCa |
Significant inverse association between dietary α-carotene intake and PCa (RR: 0.81; CI: 0.76–0.99). No difference for β-carotene and lycopene intake. Only blood levels of lycopene were significantly associated with reduced PCa risk (RR: 0.81; CI: 0.69–0.96) |
| Rowles et al., 2017 [40] | 42 studies; 19 CC 13 NCC 8 cohort 2 case-cohort |
Effect of: Lycopene intake on PCa Lycopene circulating concentrations on PCa |
Dietary intake (RR = 0.88, CI: 0.78–0.98) and circulating concentrations (RR = 0.88, CI: 0.79–0.98) of lycopene were significantly associated with reduced PCa risk |
CC, case–control study; NCC, nested case–control study; CI, confidence interval; RR, relative risk.
2. Kidney Cancer
Kidney cancer is a broad term used to describe a heterogeneous group of tumors from a histological point of view. Kidney cancer can develop from renal parenchyma or the renal collecting system. Renal cell carcinoma (RCC) arises from renal parenchyma epithelial cells and accounts for approximately 90% of kidney cancer cases. RCC accounts for around 3% of all cancers, with the highest incidence reported in Western countries [11]. The most common histological type of RCC is clear cell RCC, which represents ~80% of RCCs. Among the other histological subtypes of kidney cancer, papillary (~10%) and chromophobe (~5%) are the most common. Clear cell and papillary RCCs stem from the epithelial cells of the proximal tubule. Chromophobe RCC is thought to arise from the epithelium of the collecting tubule [69]. Well-established risk factors include smoking, obesity, hypertension, and diabetes [70]. Carotenoids, as potent antioxidants, may influence RCC risk.
Recently, Sahin et al. conducted a very interesting experimental study to examine the role of a lycopene-rich diet in the development of RCC in the tuberous sclerosis 2 (TSC2) mutant Eker rat model. Eker rats develop spontaneous renal tumors and leiomyoma, which may be due to tuberous sclerosis 2 (TSC2) mutation resulting in the activation of the mammalian target of the rapamycin (mTOR) pathway. Eker rats received 0, 100, or 200 mg/kg of lycopene as part of their diet. After 18 months, the mean numbers of renal carcinomas were statistically significantly decreased in the lycopene-treated rats (p < 0.008) when compared with the untreated controls. Tumor numbers decreased linearly as the daily lycopene increased from 0 to 200, suggesting a role of lycopene in the prevention of RCC [71].
Bock et al. recently published the results of the U.S. Kidney Cancer Study, which was a population-based case–control study. Clear, significant inverse associations with RCC risk were found for α-carotene, β-carotene, lutein, zeaxanthin, and lycopene after adjusting for all variables [72].
In another case–control study conducted on 1138 histologically confirmed cases of RCC, Hu et al. showed a significant reduction in RCC risk, with ORs of 0.74 and 0.77 for the highest versus the lowest quartiles for β-carotene and lutein/zeaxanthin. This relationship was more pronounced in women, obese, and ever smoking individuals [73]. Two other case–control studies supported a significant protective influence of carotenoids on RCC risk [74,75]. However, a case–control study by Bosetti et al. did not show any protective impact of carotenoid intake and RCC risk [76].
The Women’s Health Initiative (WHI) was a prospective cohort study that included 96,196 postmenopausal women who were followed for up to 12 years.
There were 240 cases of RCC diagnosed during follow-up. Lycopene intake was inversely correlated with RCC risk. Individuals with the highest quartile of intake had a 39% lower risk of RCC compared with those in the lowest quartile. Interestingly, none of the other evaluated carotenoids (dietary β-carotene, α-carotene, β-cryptoxanthin, and lutein plus zeaxanthin) showed any significant association [77].
On the other hand, a prospective cohort study with 88,759 women and 47,828 men did not show a significant influence of lycopene on RCC risk, although it did find significant correlations for β-carotene, α-carotene, β-cryptoxanthin, and lutein plus zeaxanthin [78]. It was shown in the ATBC prospective study that neither lycopene nor other carotenoid intake was correlated with RCC risk [79], and this confirmed other cohort studies that showed null associations between carotenoids and RCC [80,81].
In 2009, Lee published a pooled cohort analysis of 13 prospective studies that included 1478 cases of RCC among 530,469 women and 244,483 men, who were followed for up to 7 to 20 years. It showed that increased vegetable and fruit consumption was associated with a decreased risk of RCC. Among the specific carotenoids they observed, there was an 18% lower risk of RCC when comparing the highest and lowest quintiles of β-carotene intake. There was a similar trend for other carotenoids (α-carotene, β-cryptoxanthin, and lutein/zeaxanthin) [82].
Zhang et al. recently published a meta-analysis that encompassed 19 observational studies (5 cohort and 14 case–control) with 10,215 RCC cases, summarizing current evidence from epidemiological data on the topic of fruit and vegetables and RCC risk. Although they did not examine carotenoid intake in their work, they found significant reductions in RCC risk for the highest versus the lowest intake of vegetables and fruit (RR = 0.73 and 0.86 respectively) [83]. It can only be speculated that carotenoids were at least partially responsible for the observed effect.
This entry is adapted from the peer-reviewed paper 10.3390/nu14071367
This entry is offline, you can click here to edit this entry!