Gender differences in psychiatric disorders and drug use are well known. Cannabis is the most widely used illegal drug among young people. In recent years, its use has been related to the development of psychiatric pathologies; however, few studies have incorporated the gender perspective as of yet. Men have a higher prevalence using cannabis; however, women show a faster transition from recreational use to compulsive use, higher levels of craving with more relapses, and higher prevalence of dual pathology. Clinical studies clearly show the existence of gender differences in psychiatric symptoms associated with cannabis use. Although these results are not conclusive, they seem to indicate a higher vulnerability of women in the development of psychosis and anxiety, while men seem to be more vulnerable to developing depressive symptoms with long-term cannabis misuses.
- cannabis
- gender differences
- psychotic disorders
1. Introduction
2. Dual Diagnoses in Cannabis Users
3. Gender Differences in the Development of Psychotic, Depressive and Anxious Symptoms Associated with Cannabis Use
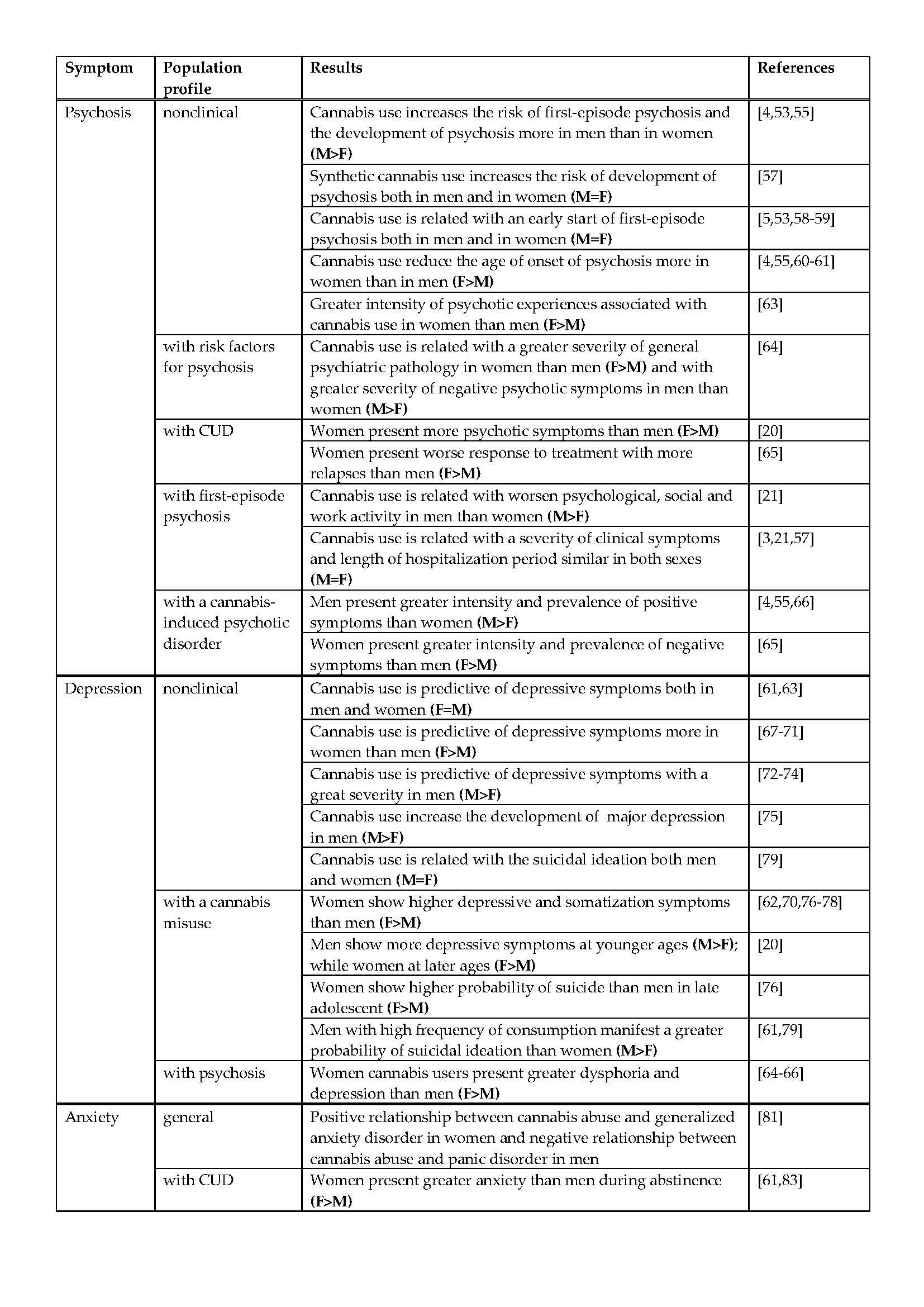
Finally, there are few studies that relate cannabis use to the development of anxious symptomatology, as most studies focus on assessing anxiety as a risk factor for its use. In general, women have the highest levels of anxiety and related disorders among adolescents [20][70], the general population [20][64][67][81], and psychiatric patients [76][66][77][78], with the biggest gender differences found in late adolescents [20]. Specifically, it has been described that the men and women with low stress tolerance are those who show the most problems related to cannabis use, and in particular women who use the drug as a stress-coping mechanism [82], in a manner similar to that previously commented upon [21][20]. Hence, a positive relationship has been found between cannabis abuse and generalized anxiety disorder in women in the general population, while men showed a negative relationship with panic disorder [81]. In addition, women manifest greater anxiety than men in the periods of abstinence [61][83]. As observed with depression, Foster et al. [76] found no relationship between the age of onset of CUD and anxiety problems.
In conclusion, the scientific evidence reveals the existence of gender differences in psychiatric symptoms associated with cannabis use, although the direction of such differences is not always clear [54]. A lack of information in studies about variables such as the THC level in the cannabis used, the frequency of use or the age of onset of cannabis use makes it difficult to know the causes for the conflicting results. Besides, few studies consider the specific characteristics of women diagnosed with dual pathology, although all the data indicate a higher prevalence of drug-associated pathologies and a worse prognosis in women [27]. For this reason, it is necessary to delve deeper into this issue and address gender differences to create more individualized prevention strategies and more effective treatment for dual disorders related with cannabis abuse.
References
- Hartung, C.M.; Lefler, E.K. Sex and gender in psychopathology: DSM–5 and beyond. Psychol. Bull. 2019, 145, 390–409.
- Riecher-Rössler, A. Sex and gender differences in mental disorders. Lancet Psychiatry 2016, 4, 8–9.
- González-Rodríguez, A.; Studerus, E.; Spitz, A.; Bugra, H.; Aston, J.; Borgwardt, S.; Rapp, C.; Riecher-Rossler, A. Gender differences in the psychopathology of emerging psychosis. Isr. J. Psychiatry Relat. Sci. 2014, 51, 85–93.
- Mendrek, A.; Fattore, L. Sex differences in drug-induced psychosis. Curr. Opin. Behav. Sci. 2017, 13, 152–157.
- Riecher-Rössler, A.; Butler, S.; Kulkarni, J. Sex and gender differences in schizophrenic psychoses—A critical review. Arch. Women’s Ment. Health 2018, 21, 627–648.
- Bangasser, D.A.; Cuarenta, A. Sex differences in anxiety and depression: Circuits and mechanisms. Nat. Rev. Neurosci. 2021, 22, 674–684.
- Eid, R.S.; Gobinath, A.R.; Galea, L.A. Sex differences in depression: Insights from clinical and preclinical studies. Prog. Neurobiol. 2019, 176, 86–102.
- Kuehner, C. Why is depression more common among women than among men? Lancet Psychiatry 2016, 4, 146–158.
- Li, S.H.; Graham, B.M. Why are women so vulnerable to anxiety, trauma-related and stress-related disorders? The potential role of sex hormones. Lancet Psychiatry 2016, 4, 73–82.
- Songtachalert, T.; Roomruangwong, C.; Carvalho, A.F.; Bourin, M.; Maes, M. Anxiety Disorders: Sex Differences in Serotonin and Tryptophan Metabolism. Curr. Top. Med. Chem. 2018, 18, 1704–1715.
- Ait-Daoud, N.; Blevins, D.; Khanna, S.; Sharma, S.; Holstege, C.P.; Amin, P. Women and Addiction: An Update. Med. Clin. N. Am. 2019, 103, 699–711.
- McHugh, R.K.; Votaw, V.R.; Sugarman, D.E.; Greenfield, S.F. Sex and gender differences in substance use disorders. Clin. Psychol. Rev. 2018, 66, 12–23.
- Quigley, J.A.; Logsdon, M.K.; Turner, C.A.; Gonzalez, I.L.; Leonardo, N.; Becker, J.B. Sex differences in vulnerability to addiction. Neuropharmacology 2021, 187, 108491.
- Riley, A.L.; Hempel, B.J.; Clasen, M.M. Sex as a biological variable: Drug use and abuse. Physiol. Behav. 2018, 187, 79–96.
- Teixidó-Compañó, E.; Espelt, A.; Sordo, L.; Bravo, M.J.; Sarasa-Renedo, A.; Indave, B.I.; Bosque-Prous, M.; Brugal, M.T. Differences between men and women in substance use: The role of educational level and employment status. Gac. Sanit. 2018, 32, 41–47.
- Observatorio Español de las Drogas y las Adicciones. Informe 2021. Alcohol, Tabaco y Drogas Ilegales en España. Madrid: Ministerio de Sanidad. Delegación del Gobierno Para el Plan Nacional Sobre Drogas, 2021, 243p. Available online: https://pnsd.sanidad.gob.es/profesionales/sistemasInformacion/informesEstadisticas/pdf/2021OEDA-INFORME.pdf (accessed on 24 January 2022).
- World Drug Report 2021 (United Nations Publication, Sales No. E.21.XI.8). Available online: https://www.unodc.org/res/wdr2021/field/WDR21_Booklet_3.pdf (accessed on 24 January 2022).
- European Monitoring Centre for Drugs and Drug Addiction. European Drug Report 2021: Trends and Developments; Publications Office of the European Union: Luxembourg. 2021. Available online: https://www.emcdda.europa.eu/system/files/publications/13838/TDAT21001ENN.pdf (accessed on 24 January 2022).
- Kerridge BT, Pickering R, Chou P, Saha TD, Hasin DS. DSM-5 cannabis use disorder in the National Epidemiologic Survey on Alcohol and Related Conditions-III: Gender-specific profiles. Addict Behav, 2018, 76(April 2017), 52–60. doi: 10.1016/j.addbeh.2017.07.012
- Leadbeater, B.; Ames, M.E.; Linden-Carmichael, A.N. Age-varying effects of cannabis use frequency and disorder on symptoms of psychosis, depression and anxiety in adolescents and adults. Addiction 2018, 114, 278–293.
- Arranz, S.; Mané, A.; Bergé, D.; Monserrat, C.; Cabezas, A.; Vilella, E.; Sanchez-Gistau, V. The impact of sex and cannabis on clinical features in first–admitted patients with psychosis. Eur. Neuropsychopharmacol. 2020, 36, 235–243.
- Compton, M.T.; Broussard, B.; Ramsay, C.E.; Stewart, T. Pre-illness cannabis use and the early course of nonaffective psychotic disorders: Associations with premorbid functioning, the prodrome, and mode of onset of psychosis. Schizophr. Res. 2011, 126, 71–76.
- Di Forti, M.; Sallis, H.; Allegri, F.; Trotta, A.; Ferraro, L.; Stilo, S.A.; Marconi, A.; La Cascia, C.; Reis Marques, T.; Pariante, C.; et al. Daily Use, Especially of High-Potency Cannabis, Drives the Earlier Onset of Psychosis in Cannabis Users. Schizophr. Bull. 2014, 40, 1509–1517.
- Hasin, D.; Walsh, C. Cannabis Use, Cannabis Use Disorder, and Comorbid Psychiatric Illness: A Narrative Review. J. Clin. Med. 2020, 10, 15.
- Krebs, M.; Kebir, O.; Jay, T.M. Exposure to cannabinoids can lead to persistent cognitive and psychiatric disorders. Eur. J. Pain 2019, 23, 1225–1233.
- Szerman, N.; Martinez-Raga, J. Dual disorders: Two different mental disorders? Adv. Dual. Diagn. 2015, 8, 2.
- Torrens-Melich, M.; Orengo, T.; de Fonseca, F.R.; Almodóvar, I.; Baquero, A.; Benito, A. Gender Perspective in Dual Diagnosis. Brain Sci. 2021, 11, 1101.
- NIDA. Addiction and Co-Occurring Mental Disorders. National Institute on Drug Abuse Website. 1 February 2007. Available online: https://archives.drugabuse.gov/news-events/nida-notes/2007/02/addiction-co-occurring-mental-disorders (accessed on 18 January 2022).
- Araos, P.; Vergara-moragues, E.; Pedraz, M.; Javier, F.; Rodríguez, F. Adicción a cannabis: Bases neurobiológicas y consecuencias médicas. Rev. Española Drogodepend 2014, 39, 9–30.
- Ferland, J.-M.; Hurd, Y.L. Deconstructing the neurobiology of cannabis use disorder. Nat. Neurosci. 2020, 23, 600–610.
- Cohen, K.; Weizman, A.; Weinstein, A. Positive and Negative Effects of Cannabis and Cannabinoids on Health. Clin. Pharmacol. Ther. 2019, 105, 1139–1147.
- De Aquino, J.; Sherif, M.; Radhakrishnan, R.; Cahill, J.D.; Ranganathan, M.; D’Souza, D.C. The Psychiatric Consequences of Cannabinoids. Clin. Ther. 2018, 40, 1448–1456.
- Fonseca-Pedrero, E.; Lucas-Molina, B.; Pérez-Albéniz, A.; Inchausti, F.; Ortuño-Sierra, J. Experiencias psicóticas atenuadas y consumo de cannabis en adolescentes de la población general. Adicciones 2019, 32, 41.
- Moore, T.H.; Zammit, S.; Lingford-Hughes, A.; Barnes, T.R.; Jones, P.B.; Burke, M.; Lewis, G. Cannabis use and risk of psychotic or affective mental health outcomes: A systematic review. Lancet 2007, 370, 319–328.
- Zammit, S.; Moore, T.H.M.; Lingford-Hughes, A.; Barnes, T.R.E.; Jones, P.B.; Burke, M.; Lewis, G. Effects of cannabis use on outcomes of psychotic disorders: Systematic review. Br. J. Psychiatry 2008, 193, 357–363.
- Blanco, C.; Hasin, D.S.; Wall, M.M.; Flórez-Salamanca, L.; Hoertel, N.; Wang, S.; Kerridge, B.T.; Olfson, M. Cannabis Use and Risk of Psychiatric Disorders: Prospective evidence from a US national longitudinal study. JAMA Psychiatry 2016, 73, 388–395.
- Feingold, D.; Weiser, M.; Rehm, J.; Lev-Ran, S. The association between cannabis use and mood disorders: A longitudinal study. J. Affect. Disord. 2015, 172, 211–218.
- Gallego-Landin, I.; García-Baos, A.; Castro-Zavala, A.; Valverde, O. Reviewing the Role of the Endocannabinoid System in the Pathophysiology of Depression. Front. Pharmacol. 2021, 12, 762738.
- Lowe, D.J.E.; Sasiadek, J.D.; Coles, A.S.; George, T.P. Cannabis and mental illness: A review. Eur. Arch. Psychiatry Clin. Neurosci. 2019, 176, 107–120.
- Hanna, R.C.; Perez, J.M.; Ghose, S. Cannabis and development of dual diagnoses: A literature review. Am. J. Drug Alcohol Abus. 2016, 43, 442–455.
- Fantuzzi, C.; Mezzina, R. Dual diagnosis: A systematic review of the organization of community health services. Int. J. Soc. Psychiatry 2020, 66, 300–310.
- Chan, Y.-F.; Dennis, M.L.; Funk, R.R. Prevalence and comorbidity of major internalizing and externalizing problems among adolescents and adults presenting to substance abuse treatment. J. Subst. Abus. Treat. 2008, 34, 14–24.
- Arias, F.; Szerman, N.; Vega, P.; Mesias, B.; Basurte, I.; Morant, C.; Ochoa, E.; Poyo, F.; Babín, F. Madrid study on the prevalence and characteristics of outpatients with dual pathology in community mental health and substance misuse services. Adicciones 2013, 25, 118–127.
- Serrano-Serrano, A.B.; Marquez-Arrico, J.E.; Navarro, J.F.; Martinez-Nicolas, A.; Adan, A. Circadian Characteristics in Patients under Treatment for Substance Use Disorders and Severe Mental Illness (Schizophrenia, Major Depression and Bipolar Disorder). J. Clin. Med. 2021, 10, 4388.
- Di Forti, M.; Quattrone, D.; Freeman, T.P.; Tripoli, G.; Gayer-Anderson, C.; Quigley, H.; Rodriguez, V.; Jongsma, H.E.; Ferraro, L.; La Cascia, C.; et al. The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): A multicentre case-control study. Lancet Psychiatry 2019, 6, 427–436.
- Hamilton, I.; Monaghan, M. Cannabis and Psychosis: Are We any Closer to Understanding the Relationship? Curr. Psychiatry Rep. 2019, 21, 48.
- Reid, S.; Bhattacharyya, S. Antipsychotic treatment failure in patients with psychosis and co-morbid cannabis use: A systematic review. Psychiatry Res. 2019, 280, 112523.
- Casajuana Kögel, C.; López-pelayo, H.; Oliveras, C.; Colom, J.; Gual, A.; Balcells-oliveró, M.M. The relationship between motivations for cannabis consumption and problematic use. Adicciones 2021, 33, 31–42.
- Leweke, F.M.; Koethe, D. Cannabis and psychiatric disorders: It is not only addiction. Addict. Biol. 2008, 13, 264–275.
- Koob, G.F.; Volkow, N.D. Neurobiology of addiction: A neurocircuitry analysis. Lancet Psychiatry 2016, 3, 760–773.
- Gobbi, G.; Atkin, T.; Zytynski, T.; Wang, S.; Askari, S.; Boruff, J.; Ware, M.; Marmorstein, N.; Cipriani, A.; Dendukuri, N.; et al. Association of Cannabis Use in Adolescence and Risk of Depression, Anxiety, and Suicidality in Young Adulthood. JAMA Psychiatry 2019, 76, 426–434.
- Satre, D.D.; Bahorik, A.; Zaman, T.; Ramo, D. Psychiatric Disorders and Comorbid Cannabis Use. J. Clin. Psychiatry 2018, 79, 79–81.
- Crocker, C.E.; Tibbo, P.G. The interaction of gender and cannabis in early phase psychosis. Schizophr. Res. 2017, 194, 18–25.
- Prieto-Arenas, L.; Díaz Fernando-Alonso, I. Diferencias de género en el desarrollo de sintomatología psicótica, depresiva y ansiosa asociada al consumo de cannabis. Bachelor’s Thesis, Universidad Católica de Valencia, Valencia, Spain, 2021.
- Hamilton, I.; Galdas, P.; Essex, H. Cannabis psychosis, gender matters. Adv. Dual. Diagn. 2015, 8, 153–162.
- Arranz, B.; Safont, G.; Corripio, I.; Ramirez, N.; Dueñas, R.M.; Pérez, V.; Álvarez, E.; San, L.; San, L. Substance Use in Patients with First-Episode Psychosis: Is Gender Relevant? J. Dual Diagn. 2015, 11, 153–160.
- Nia, A.B.; Mann, C.L.; Spriggs, S.; DeFrancisco, D.R.; Carbonaro, S.; Parvez, L.; Galynker, I.I.; Perkel, C.A.; Hurd, Y.L. The Relevance of Sex in the Association of Synthetic Cannabinoid Use with Psychosis and Agitation in an Inpatient Population. J. Clin. Psychiatry 2019, 80, 19424.
- Dekker, N.; Meijer, J.; Koeter, M.; van den Brink, W.; van Beveren, N.; GROUP Investigators; Kahn, R.S.; Linszen, D.H.; van Os, J.; Wiersma, D.; et al. Age at onset of non-affective psychosis in relation to cannabis use, other drug use and gender. Psychol. Med. 2012, 42, 1903–1911.
- Donoghue, K.; Doody, G.; Murray, R.; Jones, P.; Morgan, C.; Dazzan, P.; Hart, J.; Mazzoncini, R.; MacCabe, J.H. Cannabis use, gender and age of onset of schizophrenia: Data from the ÆSOP study. Psychiatry Res. 2014, 215, 528–532.
- Allegri, F.; Murri, M.B.; Paparelli, A.; Marcacci, T.; Braca, M.; Menchetti, M.; Michetti, R.; Berardi, D.; Tarricone, I. Current cannabis use and age of psychosis onset: A gender-mediated relationship? Results from an 8-year FEP incidence study in Bologna. Psychiatry Res. 2013, 210, 368–370.
- Calakos, K.C.; Bhatt, S.; Foster, D.W.; Cosgrove, K.P. Mechanisms Underlying Sex Differences in Cannabis Use. Curr. Addict. Rep. 2017, 4, 439–453.
- Fernández-Artamendi, S.; Martínez-Loredo, V.; López-Núñez, C. Sex Differences in Comorbidity Between Substance Use and Mental Health in Adolescents: Two Sides of the Same Coin. Psicothema 2021, 33, 36–43.
- Verdoux, H.; Sorbara, F.; Gindre, C.; Swendsen, J.D.; van Os, J. Cannabis use and dimensions of psychosis in a nonclinical population of female subjects. Schizophr. Res. 2001, 59, 77–84.
- Menghini-Müller, S.; Studerus, E.; Ittig, S.; Heitz, U.; Egloff, L.; Andreou, C.; Valmaggia, L.R.; Kempton, M.J.; van der Gaag, M.; De Haan, L.; et al. Gender differences of patients at-risk for psychosis regarding symptomatology, drug use, comorbidity and functioning—Results from the EU-GEI study. Eur. Psychiatry 2019, 59, 52–59.
- Lange, E.H.; Nesvåg, R.; Ringen, P.A.; Hartberg, C.B.; Haukvik, U.K.; Andreassen, O.A.; Melle, I.; Agartz, I. One year follow-up of alcohol and illicit substance use in first-episode psychosis: Does gender matter? Compr. Psychiatry 2014, 55, 274–282.
- Bachetti, M.C.; Lanzi, R.; Menculini, G.; Scopetta, F.; Tortorella, A.; Moretti, P. Cannabinoid-induced psychosis: A cross-sectional gender study. Psychiatr. Danub. 2020, 32, 200–206.
- Fattore, L.; Fratta, W. How important are sex differences in cannabinoid action? J. Cereb. Blood Flow Metab. 2010, 160, 544–548.
- Poulin, C.; Hand, D.; Boudreau, B.; Santor, D. Gender differences in the association between substance use and elevated depressive symptoms in a general adolescent population. Addiction 2005, 100, 525–535.
- Schuler, M.S.; Vasilenko, S.A.; Lanza, S.T. Age-varying associations between substance use behaviors and depressive symptoms during adolescence and young adulthood. Drug Alcohol Depend. 2015, 157, 75–82.
- Patton, G.C.; Coffey, C.; Carlin, J.; Degenhardt, L.; Lynskey, M.; Hall, W. Cannabis use and mental health in young people: Cohort study. BMJ 2002, 325, 1195–1198.
- Halladay, J.E.; Boyle, M.H.; Munn, C.; Jack, S.M.; Georgiades, K. Sex Differences in the Association Between Cannabis Use and Suicidal Ideation and Attempts, Depression, and Psychological Distress Among Canadians. Can. J. Psychiatry 2018, 64, 345–350.
- Crane, N.A.; Langenecker, S.; Mermelstein, R.J. Gender differences in the associations among marijuana use, cigarette use, and symptoms of depression during adolescence and young adulthood. Addict. Behav. 2015, 49, 33–39.
- Assari, S.; Mistry, R.; Caldwell, C.H.; Zimmerman, M.A. Marijuana Use and Depressive Symptoms; Gender Differences in African American Adolescents. Front. Psychol. 2018, 9, 2135.
- Crane, N.; Schuster, R.M.; Fusar-Poli, P.; Gonzalez, R. Effects of Cannabis on Neurocognitive Functioning: Recent Advances, Neurodevelopmental Influences, and Sex Differences. Neuropsychol. Rev. 2012, 23, 117–137.
- Park, J.-Y.; Wu, L.-T. Differences in behavioral health disorders and unmet treatment needs between medical marijuana users and recreational marijuana users: Results from a national adult sample. Drug Alcohol Depend. 2017, 180, 311–318.
- Foster, K.T.; Li, N.; McClure, E.A.; Sonne, S.C.; Gray, K.M. Gender Differences in Internalizing Symptoms and Suicide Risk Among Men and Women Seeking Treatment for Cannabis Use Disorder from Late Adolescence to Middle Adulthood. J. Subst. Abus. Treat. 2016, 66, 16–22.
- Khan, S.S.; Secades-Villa, R.; Okuda, M.; Wang, S.; Pérez-Fuentes, G.; Kerridge, B.; Blanco, C. Gender differences in cannabis use disorders: Results from the National Epidemiologic Survey of Alcohol and Related Conditions. Drug Alcohol Depend. 2012, 130, 101–108.
- Sherman, B.J.; McRae-Clark, A.L.; Ms, N.L.B.; Sonne, S.C.; Killeen, T.K.; Cloud, K.; Gray, K.M. Gender differences among treatment-seeking adults with cannabis use disorder: Clinical profiles of women and men enrolled in the achieving cannabis cessation-evaluating N-acetylcysteine treatment (ACCENT) study HHS Public Access. Am. J. Addict. 2017, 26, 136–144.
- Naji, L.; Rosic, T.; Dennis, B.; Bhatt, M.; Sanger, N.; Hudson, J.; Mouravska, N.; Thabane, L.; Samaan, Z. The association between cannabis use and suicidal behavior in patients with psychiatric disorders: An analysis of sex differences. Biol. Sex Differ. 2018, 9, 22.
- Waterreus A, Di Prinzio P, Badcock JC, Martin-Iverson M, Jablensky A, Morgan VA. Is cannabis a risk factor for suicide attempts in men and women with psychotic illness? Psychopharmacology (Berl), 2018, 235, 2275–85. doi: 10.1007/s00213-018-4924-6
- Goldstein RB, Dawson DA, Patricia Chou S, Grant BF. Sex differences in prevalence and comorbidity of alcohol and drug use disorders: Results from wave 2 of the national epidemiologic survey on alcohol and related conditions. J Stud Alcohol Drugs, 2012, 73(6), 938–50. doi: 10.15288/jsad.2012.73.938
- Bujarski SJ, Norberg MM, Copeland J. The association between distress tolerance and cannabis use-related problems: the mediating and moderating roles of coping motives and gender. Addict Behav, 2012, 37, 1181–4. doi: 10.1016/j.addbeh.2012.05.014
- Cuttler C, Mischley LK, Sexton M. Sex Differences in Cannabis Use and Effects: A Cross-Sectional Survey of Cannabis Users. Cannabis Cannabinoid Res, 2016, 1(1), 166–75. doi: 10.1089/can.2016.0010