Ultrasound is a widely available, approachable, and relatively inexpensive imaging modality that allows for real-time evaluation of a suspected renal mass without the drawbacks of ionizing radiation and the risk of an MRI. CEUS has several advantages over traditional grayscale ultrasound in the characterization of indeterminate renal masses. It has a distinct value in the characterization of cystic renal masses and has the potential to differentiate benign from malignant renal masses to some extent. Ultrasound molecular imaging could potentially be an extension of the use of CEUS for serial disease monitoring and longitudinal assessment of treatment response, though it remains in preclinical stages of development at this time. While emerging micro-Doppler techniques and elastography have shown some encouraging applications, current evidence is limited, and neither is ready for widespread clinical use.
1. Contrast-Enhanced Ultrasound
Contrast-enhanced ultrasound (CEUS) is an emerging technique that addresses some of the limitations of non-enhanced grayscale and traditional Doppler ultrasound for the detection of vascularization within soft tissues. Intravenously administered ultrasound contrast agents consist of small particles: gas-filled cores encapsulated within biodegradable shells. These microbubbles, approximately the size of red blood cells, resonate non-linearly when insonnated by ultrasound. The unique signals from microbubbles can be separated from background tissues, allowing for the specific detection of blood flow within perfused tissues. CEUS can definitively confirm simple cysts via the lack of enhancement and may help to characterize solid renal lesions based on differences in lesional versus renal cortical perfusion [
17,
18].
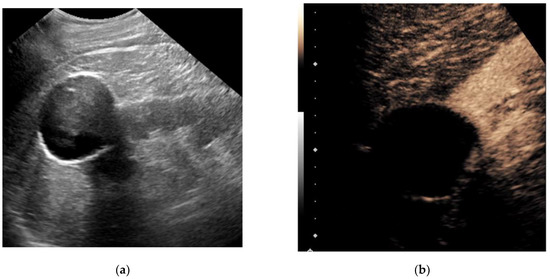
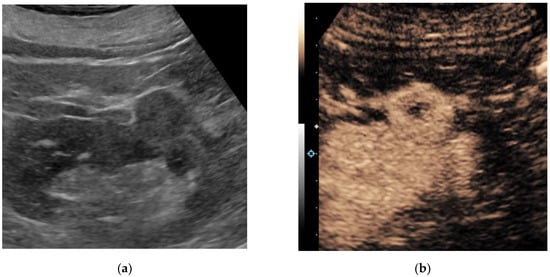
Figure 1 and
Figure 2 illustrate the performance of CEUS compared with traditional grayscale ultrasound by identifying enhancement within a renal mass. Despite the lack of radiation, low cost and highly favorable safety profile of ultrasound contrast agents, operator dependency and other technical factors may limit reproducibility [
19,
20].
Figure 1. A 79-year-old man with a history of bladder cancer undergoing evaluation for hydronephrosis. Grayscale ultrasound image of the left kidney in the longitudinal orientation (a) shows an exophytic hypoechoic mass containing internal low-level echos. Following an intravenous injection of 1.8 cc Lumason ultrasound contrast, a contrast-enhanced ultrasound image focused at the upper pole (b) revealed the mass was completely non-enhancing (devoid of signal), which is diagnostic for a simple cyst. No further follow-up was necessary.
Figure 2. A 67-year-old man with multiple renal lesions, status post SBRT one year prior for contra-lateral RCC. Grayscale ultrasound image of the left kidney in longitudinal orientation (a) shows an isoechoic exophytic nodule. Following the intravenous administration of 1.0 cc Lumason ultrasound contrast, a contrast-enhanced ultrasound image (b) shows the nodule demonstrating predominantly solid avid enhancement relative to the adjacent renal cortex. A partial nephrectomy revealed clear cell renal cell carcinoma, grade 2.
CEUS has a distinct value in characterizing septations and mural nodules within cystic renal masses based on the presence or lack of enhancement, which is of specific interest for the equivocal Bosniak IIF and III cystic renal masses. However, specific definitions for CEUS imaging findings to predict the gradual increase in the risk of malignancy (i.e., equivalent to the Bosniak classification) are currently lacking [
15]. According to several reports, the sensitivity and specificity of CEUS for malignancy in a cystic renal mass was comparable to CECT and MRI [
19,
21,
22,
23,
24,
25,
26,
27,
28]. Additionally, CEUS was reported to perform at least as well as, if not better than, CECT and contrast-enhanced MRI (CEMR) in the classification of benign versus malignant renal masses [
17,
22,
23,
24,
29,
30,
31]. Furrer et al. performed a meta-analysis on 1290 patients harboring 1342 cystic or solid renal masses, comparing the performance of CEUS to CECT and CEMR in the detection of benign versus malignant histology. They reported pooled sensitivity and specificity values for CEUS, CECT and CEMR of 96%, 90% and 96%, and 78%, 77% and 75%, respectively [
17]. Their findings were in line with the findings of meta-analyses by Zhang et al., who compared CEUS to CECT in solid renal masses, and Zhou et al., who compared CEUS to CEMR in CRMs [
22,
31]. However, a low prevalence of certain benign tumor types (e.g., only 1% of renal masses were oncocytomas) likely reflects a considerable selection bias in these studies. Furthermore, it is unclear how many renal masses in these studies were excluded due to macroscopic fat seen during CT or MRI, which is virtually diagnostic of AML. They concluded that CEUS could be a valuable alternative to CECT in the evaluation of both solid as well as cystic renal masses, despite the heterogeneity across studies and the overall level of evidence being low [
17].
Although quantitative CEUS features, such as the analysis of time–intensity curves, were shown to partially aid in the distinction of clear cell RCC (ccRCC), papillary RCC (papRCC) and chromophobe RCC (chrRCC) between each other and typical AML from RCCs, there is considerable overlap between imaging features of these renal tumor subtypes [
32,
33,
34].
Moreover, both fat-poor AMLs (fpAML) and oncocytomas cannot be reliably distinguished from RCC on CEUS due to non-differing sonomorphological imaging features [
23,
32,
35,
36,
37]. Therefore, CEUS is likely inadequate for subtyping all solid renal masses at this time.
2. Ultrasound Molecular Imaging
A highly innovative approach to ultrasound imaging involves the targeting and real-time, in vivo visualization of physiologic processes with molecular-specific imaging. Molecular-targeted microbubbles have been developed as an extension of CEUS [
38,
39]. This could be of particular interest in the metastatic setting, where the response to systemic therapy is currently determined by the change in tumor volume. However, changes in tumor physiology occur sooner than measurable tumor volume changes, which might allow for earlier assessment of tumor progression, response to systemic therapy and, ultimately, therapeutic decision making. Moreover, the use of molecular imaging techniques might better characterize features relating to intrinsic disease biology, such as angiogenesis, potentially leading to more individualized treatment decision making [
40,
41]. In a recent report, Rojas et al. studied ccRCC in a xenograft model of immunodeficient mice treated with the anti-angiogenic vascular endothelial growth factor receptor (VEGFR) tyrosine kinase inhibitor sunitinib [
39]. They administered a microbubble contrast agent targeted to VEGFR-2 and subsequently imaged the tumors with CEUS after 1 week of treatment. They reported changes in VEGFR-2 expression at that time, as determined on ultrasound molecular imaging in the sunitinib-treated group, as opposed to changes in tumor volume, which only became apparent after 3 weeks. Moreover, after 1 week, response to therapy was detected in 92% of cases with ultrasound molecular imaging, whereas the detection rate was only 40% with volume measurements. Likewise, Ingels et al. studied the potential of ultrasound molecular imaging to track the response to sunitinib in a ccRCC mice xenograft model [
38]. These mice, harboring ccRCC, were randomized between treatment with sunitinib and control and were injected with both non-targeted microbubbles and microbubbles targeting VEGFR-1 and follicle-stimulating hormone receptor (FSHR). Both the VEGFR-1 and FSHR signal enhancement were significantly lower in the sunitinib group at all times of treatment, while there was no significant difference between the two groups for the non-targeted microbubble ultrasound signal. Thus, they confirmed the potential of ultrasound molecular imaging for the longitudinal assessment of treatment response to sunitinib. However, despite its potential for serial monitoring of disease, as well as longitudinal assessment of disease response to systemic therapy, ultrasound molecular imaging is still in the very early phases of development and further research endeavors will determine whether these techniques can provide additional value in clinical practice.
3. Elastography
Equivalent to the use of palpation during physical examination, ultrasound elastography measures changes in tissue stiffness, which are often seen with diffuse parenchymal diseases and the associated changes in tissue architecture [
42]. Strain elastography provides a qualitative or semi-quantitative assessment of tissue elasticity using external compression–decompression cycles from the ultrasound transducer. Shear-wave elastography (SWE) involves a quantitative assessment of tissue stiffness by measuring the propagation speed of generated shear waves through tissues. This technique does not require external compression by a transducer, relying instead on a high-amplitude push pulse (also known as acoustic radiation force impulse or ARFI), thus making it less operator dependent [
43]. Strain elastography was shown to aid in the distinction of benign vs. malignant lesions, the distinction of RCC from AML and the distinction of RCC from transitional cell carcinoma [
42,
44,
45]. SWE had potential value in the differentiation of ccRCC versus oncocytoma, ccRCC versus chrRCC or papRCC and pseudotumor from ccRCC or AML, though failed to differentiate between ccRCC and AML [
43,
46]. However, few studies have been conducted and these results lack validation, rendering clinical applications for renal mass characterization limited at this time.
4. Micro-Doppler Techniques
The presence of blood flow within a renal mass indicates solid tissue, as opposed to a renal cyst. The pattern of vascularity may help characterize indeterminate renal masses, such as differentiating malignancy from pseudomasses. Many companies are releasing novel micro-Doppler techniques with advanced clutter suppression. Some of these include Superb Micro-Vascular Imaging (Canon Medical Systems, Tochigi, Japan), Micro Vascular Imaging (GE Healthcare, Waukesha, WI, USA), Micro-Flow Imaging (Philips Healthcare, Bothell, WA, USA) and Micro Vascular Flow (Samsung Medison, Seoul, Korea). These techniques appear to improve the detection of slower flow within smaller vessels, increasing the ability to detect subtle vascularity within indeterminate renal masses that were previously below the detection threshold for traditional color and power Doppler techniques.
Leong et al. recently imaged 41 patients harboring 50 renal masses with Superb Micro-Vascular Imaging (SMI). They found that SMI had a higher diagnostic accuracy than standard color Doppler imaging and power Doppler imaging for the detection of vascularity within solid renal masses [
47]. They concluded that SMI might have potential in the detection of microvascularity within indeterminate solid renal masses. Subsequently, Mao et al. showed that SMI could distinguish significantly different patterns of vascularization between pathologically proven malignant and benign renal masses in a study on 53 patients [
48]. Conversely, conventional Doppler flow imaging could not discern these differences in vascularization.
Although the benefit of these micro-Doppler techniques includes intravenous contrast not being required, there has not been a direct comparison to CEUS for the detection of malignancy, which limits the current applications of these techniques. Future endeavors should specifically study whether the addition of these techniques to CEUS could improve the diagnostic accuracy and could potentially be a useful addition to current techniques in terms of characterizing indeterminate renal masses.
This entry is adapted from the peer-reviewed paper 10.3390/jcm11041112