Among risk factors for mental health problems, there are individual, familiar, social, and healthcare factors. Individual factors include childhood adversities, which show gender differences in distribution rates. However, existing childhood abuse prevention programs are not gender-specific. Familiar factors for mental health problems include maternity issues and intimate partner violence, and for both, some gender-specific preventive interventions are available. Social risk factors for mental health problems are related to education, employment, discrimination, and relationships. They all display gender differences, but these differences are rarely taken into account in mental health prevention programs. Lastly, despite gender differences in mental health service use being widely known, mental health services appear to be slow in developing strategies that guarantee equal access to care for all individuals.
1. Introduction
Mental disorders represent the fifth most common cause of disability worldwide [
1]. Available treatment options do not result in a
restitutio ad integrum for most mental conditions. Instead, investing efforts in mental health promotion, prevention, and early intervention may produce the best results [
2]. The World Health Organization (WHO) recommends all neuropsychiatric interventions to be oriented towards promoting positive mental health at the population level, to enhance individuals’ abilities to monitor their mental health and its determinants [
3]. On the other hand, prevention strategies aim to intervene in the pre-pathogenesis stage to prevent such conditions from arising whenever possible (primary prevention), promote early detection, screening, prompt treatment of disease, and limitation of disability (secondary prevention), and to sustain recovery, rehabilitation, and the restoration of functioning at the later stages of the disease (tertiary prevention) [
4]. Thus, depending on the need of the individuals presenting at different stages in a continuum between mental health and disease [
5], promotion and early intervention strategies aim at supporting the continuity of mental health care to achieve the best possible outcome in terms of wellbeing. Most prevention strategies so far have focused on psychosis, by applying an at-risk mental state (ARMS) concept implying the possibility to hamper the progression to full-blown disorder [
6]. However, more recent evidence begins to support the possibility of widening the clinical area of intervention beyond psychosis, including common psychiatric disorders such as depression, anxiety, substance abuse, and eating disorders [
7]. In this regard, an updated and more comprehensive clinical staging model has been proposed, the clinical high-risk mental state (CHARMS), which incorporates a trans-diagnostic paradigm [
6]. A recent reappraisal of the literature suggests the importance of reorienting such interventions towards the youth population [
8,
9].
Oncology is one of the health sectors where prevention, early detection, multidisciplinary, and personalized strategies have led to tremendous advances, reshaping cancer care [
10]. Lessons learnt from oncological research indicate that common risk factors for cancer diseases, such as alcohol, smoking, being overweight and physically inactive, have pro-cancer effects as a function of gender, with men and women being differentially exposed to the joint and multiplicative effects of risk factors [
11]. Thus, despite all things being equal, loss of health is not equal among male and female individuals, urging the adoption of a gendered perspective for more effective public health interventions.
Mental health is no exception. When developing preventive strategies for mental health, an important aspect to be considered is represented by gender, defined as socio-cultural constructs encompassing norms, rules, behaviors, and attitudes associated with being girls/women or boys/men, along with sex, which instead refers to a set of biological and physiological characteristics [
12]. Gender interacts with differences between the sexes but represents a broader-spectrum dimension and may combine with other social factors, potentially resulting in a differential exacerbation of biological susceptibilities. Considering their differential and interacting impact on mental health, both gender- and sex-related differences should always be taken into consideration, starting from the implementation of promotion of the adoption of screening strategies to identify those people at risk of developing mental health problems, to prevent their onset or at least allow action before they worsen [
8]. Furthermore, unique challenges, specific health issues, and health disparities may be faced by people with non-conforming gender, and a recent review of the literature highlights the importance of promoting gender diversity, to avoid a negative impact on mental health [
13].
Several risk factors mapping on a pluripotent pathological trajectory for mental disorders have been identified [
8]. They exert most of their influence on mental health from the prenatal period to early adulthood, with a less relevant modulation occurring until old age [
14]. Additionally, pregnancy, parenthood, childhood care, behaviors exhibited in a relationship, and socio-occupational environments are privileged areas for interventions [
14,
15,
16,
17,
18]. Research studies suggest a different response to life events as a function of gender [
19,
20].
2. Gender-Oriented Mental Health Prevention
Inter-individual differences in mental health are known and there is an agreement that mental health risk trajectories may sensibly differ as a function of gender- (e.g., social role) and sex-related (e.g., hormonal) effects [
12]. There is a limited availability of mental health prevention strategies that are specifically designed to consider gender- and sex-based differences and needs. This is a result of the paucity of high-quality trials and longitudinal studies informing on the best strategies to sustain mental health and prevent adverse outcomes, based on the psychosocial and neurobiological differences between men and women.
Early childhood represents one of the more important and most investigated areas for mental health prevention, which stems from the evidence that the neurodevelopmental period offers the greatest chances to positively shape an individual’s future at multiple levels [
18]. Conversely, in the presence of genetic and environmental affronts during childhood, several non-specific psychosocial disturbances may occur, compromising the child’s wellbeing and leading to the manifestation of a frank mental condition between early adolescence and early adult years [
168]. Mental disorders and related conditions account for 45% of the global burden of disease across the 0–25 year old age span [
168]. Results from an international survey conducted among 51,945 adults indicate that eradicating childhood adversities would reduce the occurrence of any mental disorder by one-third [
169]. Consistent, mental health preservation strategies during childhood are mainly focused on childhood abuse, however, they do not consider gender differences in childhood abuse rates and effects.
Most sex-specific preventive strategies are focused on pregnancy and post-partum as well as related familial issues, and mainly address depressive symptoms. About twice as many women as men experience depression [
170]. Risk factors increasing women’s risk of depression include psychobiological changes that occur during puberty, premenstrual problems, pregnancy, perimenopause, menopause, and life circumstances and cultural stressors [
171]. Hormonal fluxes occurring in the perinatal period, along with the psychosocial changes surrounding pregnancy, are windows to pay attention to when implementing sex-based preventive interventions. In a wider perspective, research evidence converges on the importance of promoting a positive social climate within the family to sustain individuals’ wellbeing [
172].
Regarding social factors, employment is an area contributing to shaping life and identity. Despite evidence of gender-related differences, inequalities, and discrimination in the workplace [
173], there are limited gender-specific mental health prevention programs for working and employment conditions. Some strategies have been developed for men in male-dominated industries, focusing on stress reduction. Concerning relationships, marriage is not unequivocally associated with positive or negative effects for mental health. Possibly, marital relationships confer both resources and strains, with effects in terms of the couple’s mental health that depend on the balance between these factors [
158]. It is much clearer that marriage disruption may have detrimental consequences, especially for women’s mental health and coping strategies. There are some gendered mental health preventive strategies to support healthy marriages. It is known that men are more reluctant than women to access mental health services, however, limited efforts have been put in developing strategies that guarantee equal access to care. It is worth mentioning that people with non-conforming gender may suffer from psychobiological distress [
174,
175,
176] possibly due to barriers to healthcare access [
13]. It is imperative to try and personalize access to care depending on the individual’s intrinsic needs.
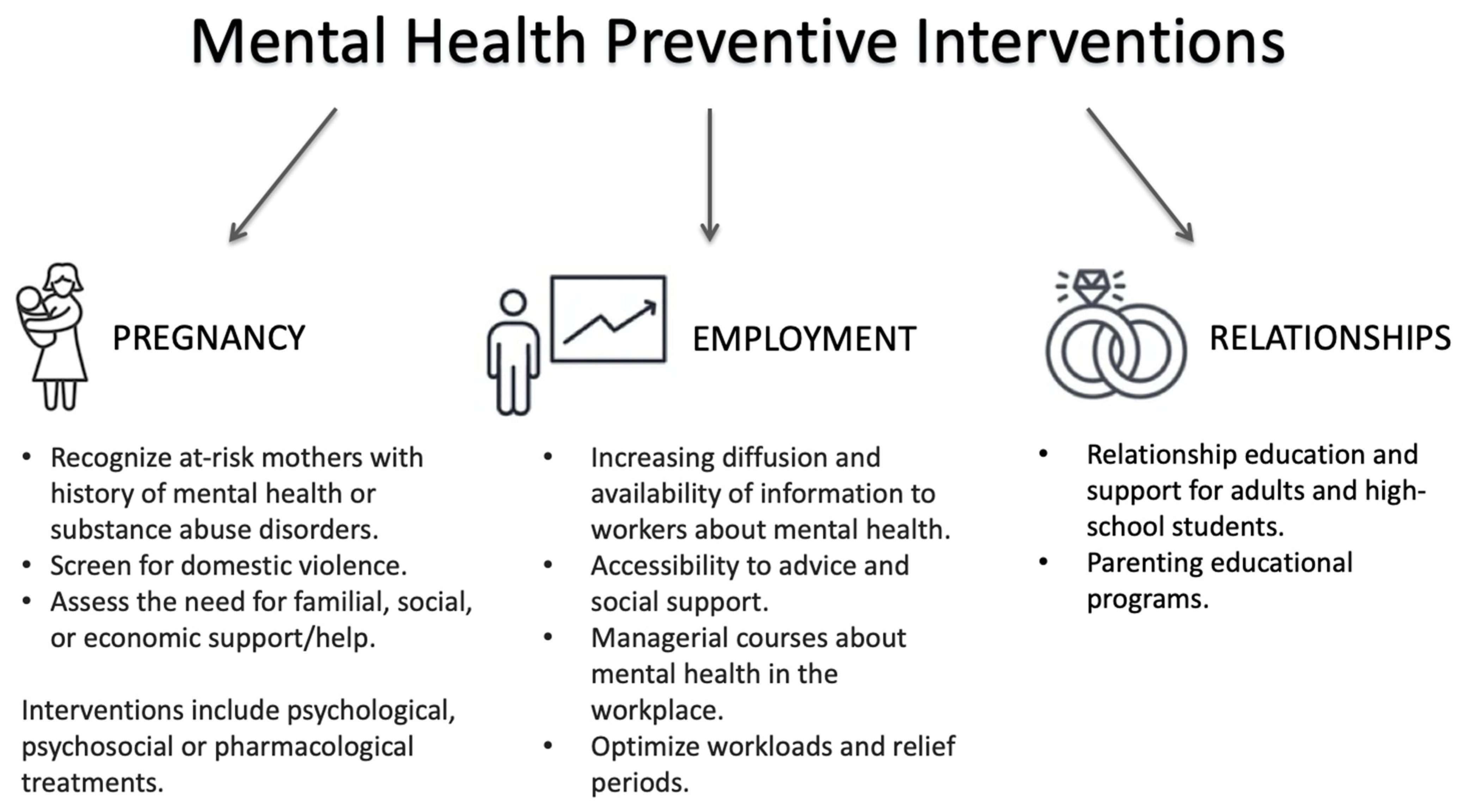
Herein offers a reappraisal of evidence on the role of gender and biological sex in mental health prevention (graphically synthesized in Figure 2).
Figure 2. Summary of available mental health preventive interventions.
3. Conclusions
Prevention and screening strategies can have a remarkable impact on individuals’ mental health and general wellbeing. Their implementation should not fail to consider that risk factors for mental health-related conditions display gender/sex differences. Such gender/sex differences have rarely been considered and included in mental health preventive programs. Most evidence comes from studies in adult populations (e.g., postpartum depression), while research on the early phases of life is lacking. More research is needed on how gender differences interact with biological and physiological characteristics in influencing mental health needs, the risk of developing a mental condition, mental health service access and utilization, and responses to pharmacological and non-pharmacological treatments.
This entry is adapted from the peer-reviewed paper 10.3390/ijerph19031493