According to the NIH, depression is a prevalent mental disorder and can occur due to genetic, biological, environmental, and psychological factors or a combination of these factors. Treatments include a form of psychotherapy such as electroconvulsive therapy (ECT) and antidepressants [
96]. The complications associated with depression include weight gain, social isolation, self-mutilation, pain, alcohol and drug abuse [
97]. Essential oils that can use for mood improvement and symptom alleviation of depression include:
This essential oil consists of approximately 150 identified compounds. However, the mood adjustment and relaxation effect provided have been attributed to β-caryophyllene, benzyl benzoate, linalool, and benzyl alcohol in the oil [
23,
24]. In 2013, the impact of ylang-ylang EO was studied on 15 healthy men wherein three drops of the oil were added to a warm water lamp maintained at 90 °C in an enclosed space. After 60 min of exposure, the subjects’ heart rate and blood pressure levels decreased along with a simultaneous decline in the activation of the autonomic nervous system (ANS) [
25]. In 2018, a study showed that inhalation of ylang ylang essential oil by anxious mice caused a decline in CREB and Fos-c in the hippocampus, decreased plasma corticosterone, and altered blood serotonin metabolism [
26]. In 2016, the mechanism behind the anxiolytic and mood adjusting effect was identified to occur through effects on the serotoninergic (5-HT) and dopaminergic pathways (DA) and was attributed to the presence of benzyl benzoate in the oil [
24]. Moreover, its major constituent, β-caryophyllene, is also associated with anti-inflammatory, anticancer, neuroprotective, antioxidant, and mood-adjusting effects [
98,
99,
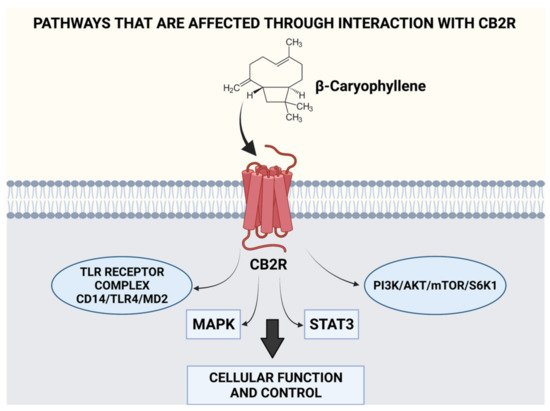
100]. Studies have indicated that the mood adjusting effects of ylang ylang oil occur due to the direct binding of β-caryophyllene to CB2R receptors located on several organs, which cause the modulation of ECS activity, thereby controlling responses (both cognitive and emotional) to stressors through ECS interactions [
28]. The ability of β-caryophyllene to modulate various pathways and possess multiple benefits through the CB2R receptor has been illustrated in
Figure 2. β-caryophyllene has been found to hinder metastasis, cause a reduction in oncogene and protein expression of cancer cells while upregulating genes and proteins that destroy cancer cells through the modulation of pathways such as MAPK, PI3K, AKT, mTOR, S6K1, and STAT3. Therefore, its use is suggested for kidney, lung, oral, liver, lymphoma, and neuroblastoma cancers due to its chemo preventive activity [
93]. β-caryophyllene when administered orally, has been found to inhibit CD14/TLR4/MD2 toll-like receptor complex that is responsible for the production of pro-inflammatory cytokines, such as IL-1β, IL-8, IL-6, and TNF-α, while also causing the synergy of μ-opioid receptor pathways [
101,
102]. Moreover, it has also been attributed to modulating pain signaling pathways in a synergistic manner with other analgesic substances [
103].
Figure 2 illustrates the various pathways affected through interaction with the ECS.
The oil consists of 15 identified compounds, and the principal component (65–85%) is trans-cinnamaldehyde which is responsible for the mood adjustment effect of the oil. Antidepressant effects in albino male mice were observed following intraperitoneal (i.p) injection (3 in 24 h/1 per day for 14 days) using doses of 0.5, 1, and 2 mg/kg [
29]. The mechanism of this effect remains unknown. However, in 2016, another group of researchers suggested the downregulation of nitric oxide synthase, cyclo-oxygenase 2 (COX-2), and TNF-α, and suppressing neuroinflammation and NF-κB and p53 in activated B-cells was responsible for the antidepressant effect observed [
30]. In contrast, Iwasaki et al. (2008) showed that intravenous (IV) administration of TCAs caused an upregulation of adrenaline secretion through adrenal sympathetic nerves along with the activation of sensory nerves that express thermosensitive transient receptor potential channels A1, thus being beneficial in monoamine-associated depressive disorders where a decline in adrenaline level is observed [
31]. Therefore, further research to determine the mechanism by which cinnamon oil exerts its antidepressant effect is needed.