From the start of the COVID-19 pandemic, new SARS-CoV-2 variants have emerged that potentially affect transmissibility, severity, and immune evasion in infected individuals. Conclusions: SARS-CoV-2 variants can potentially have an impact on clinical outcomes.
- SARS-CoV-2 variants
- mutations
- clinical outcomes
1. Introduction
2. SARS-CoV-2 Variants and Clinical Outcomes
2.1. SARS-CoV-2 Variants
| Changes | Location | Sources |
|---|---|---|
|
Spike protein (S) | [6,21,23,24,25,26,27,28,30,31,32,33,34,35,36,39,40,41,42,43,44] |
|
Nucleocapsid phosphoprotein (N protein) | [22,24,28,30,33,35,36,43,44] |
|
ORF1a | [22,27,32] |
|
NSP1 | [44] |
|
NSP2 | [30,33,39,44] |
|
NSP3 | [22,24,33,39,41,42,44] |
|
NSP4 | [24,33,35,39,41,44] |
|
NSP7 | [44] |
|
NSP8 | [33,44] |
|
NSP9 | [33] |
|
NSP12 | [22,28,41] |
|
NSP13 | [33,39,41,44] |
|
NSP14 | [39,41] |
|
NSP15 | [33] |
|
NSP16 | [33] |
|
ORF3a | [22,24,28,30,33,35,36,39,42,43,44,45] |
|
ORF6 | [24,43] |
|
ORF7b | [43] |
|
ORF8 | [23,24,35,36,39,41,45,46] |
|
RdRp | [22,23,24,25,27,30,33,35,36,39,42,43,44,47] |
|
3C-like protease | [44] |
2.2. SARS-CoV-2 Variants and Clinical Outcomes
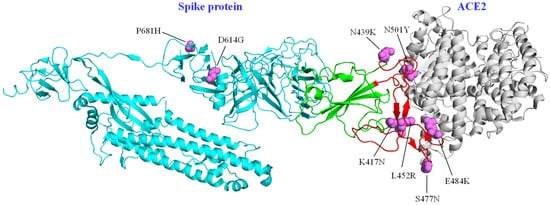
Prior to the reporting of Variants of Interest (VOI) and Variants of Concern (VOC), changes in the SARS-CoV-2 sequence that could have an impact on clinical outcomes had been determined [6]. The D614G variant in the spike protein was initially considered to be related to a higher rate of hospitalizations and moderate to severe clinical outcomes [6,23]; however, analyses in different cohorts showed no relationship with disease severity; this change increases the adaptability of the virus in human populations, without necessarily causing more severe disease [25,43]. The same scenario was visualized for the N439K variant in the spike protein, which was also not found to have a direct effect on clinical outcomes, compared to the original virus. However, it was reported that this substitution had emerged in different clades independently and that it increased affinity for ACE2 and resistance against various neutralizing monoclonal antibodies [31].
2.3. Rise and Spread of Variants of Concern
2.4. Other Variants Related with Clinical Outcomes
3. Conclusions
This entry is adapted from the peer-reviewed paper 10.3390/life12020170