1. The Need of Synthetic Biomaterials in Bone Regeneration
Bone regeneration remains an important challenge in orthopedic surgery [
4,
5,
6]. In this regard, bone tissue engineering aims to promote the self-regeneration of bone tissue injury [
7]. This can be performed by using a wide range of biocompatible materials combined or not with osteogenic cells, which provide physical support and suitable biochemical signals for promoting bone healing [
8,
9,
10]. These bioactive materials are paramount in this regard to repair osteoporotic bone exhibiting low bone mineral density and bone fragility, which hampers the use of more rigid metal-based implants. These materials are commonly fabricated as a three-dimensional structure, termed “scaffold” exhibiting high porosity and pore interconnectivity to host various osteogenic agents to promote osteoblastic growth and function [
11,
12].
During the last decades, a variety of biomaterials as synthetic bone graft substitutes have been synthesized. In this respect, glass-ceramics such as silica-based glasses containing Si, Ca and P are particularly interesting for their ability to form a calcium phosphate layer that enables binding to bone and prevents the formation of a fibrous layer around the material used as an implant. An early fixation and well osseointegration of the implant is highly demanded during surgical practices since implant instability increases the risk of aseptic loosening. Ca and P are the main components of bone apatite (Ca
10(PO
4,CO
3)
6(OH)
2), and thus they have a key role in bone remodeling [
13,
14]. Both Si and Ca ions can improve osteogenesis by upregulating the expression of osteogenic genes, and are associated with bone tissue mineralization [
15,
16,
17,
18]. These bioactive ceramics also induce vascularization [
19,
20], and can interact and act in concert with osteogenic cells to promote bone formation, and as such are recognized for their excellent biocompatibility and osteoconductivity, as well as for their antimicrobial properties [
21,
22]. They can be manufactured (e.g., as the inorganic component in organic–inorganic hybrid materials) with improved mechanical properties to provide suitable physical support during bone healing [
7,
23,
24].
2. The Three Families of Bioactive Glasses
In the 1970s, it was discovered that some glass compositions as implants failed to elicit a foreign body reaction [
28]. Accordingly, these glasses, currently denoted as bioactive glasses (BGs), were not found to be surrounded by a fibrous capsule, but integrated into the host by forming a mechanically strong bond with the adjacent living tissue. This finding opened new avenues in the design of biomaterials mainly in Orthopedics and Dentistry [
29]. Since the early stages of BGs development, it was evidenced that those with the faster bioactive response have a capacity to bind to a variety of soft tissues; justifying their current increasing interest for clinical applications beyond the skeletal system [
30].
However, melt-prepared BGs (MPGs), found only rather few clinical applications, namely in the dental field, for replacing the middle ear chain ossicles, or as particulates in bone grafts, in the last twenty years [
29]. For this reason, in the 1990s, a new family of BGs, the so-called bioactive sol-gel glasses (SGGs), was obtained by wet chemistry methods, exhibiting high porosity and specific surface area [
31]. These interesting textural properties led to the assumption that SGGs could be used as matrices in drug delivery systems. Furthermore, the sol-gel method allowed processing BGs as coatings or fibers, which are shapes difficult to obtain with the traditional quenching of a melt method. However, SGGs did not meet all the initial expectations for clinical applications because their bioactive response was analogous to MPGs and because due to their large pore size dispersion they did not allow efficient control of the release of biologically active substances
. Indeed, in SGGs the bioactivity window was expanded because they were coated by an apatite-like layer after soaking in a Simulated Body Fluid (SBF), even for silica contents of 90%; while such response was limited to a maximum content of 60% for MPGs. These findings led to the assumption that SGGs might present a quicker bioactive response in SBF than MPGs. However, this was not the case; a similar period of time (2 to 7 days) was necessary to form the apatite-like layer in both types of glasses [
25]. In the 1990s, while SGGs were developed
, in the field of catalysis, mesoporous silica materials were designed to obtain materials with homogeneous pore sizes larger than that of zeolites. They were obtained in the presence of a surfactant, producing an ordered mesoporous arrangement with a very narrow pore size distribution [
32]. The very high specific surface areas and pore volumes together with high uniformity in pore size make these materials ideal materials for the controlled release of biomolecules and drugs, as it was proposed by Vallet-Regí et al. for pure silica mesoporous materials [
1]. This spurred the development of newly designed BGs, early named glasses with template glasses (TGs) and later mesoporous bioactive glasses (MBGs).
MBGs exhibit intermediate properties between SGGs and pure silica mesoporous materials. Indeed, the synthesis process of the MBGs is based on sol-gel processing similar to that of SGGs, but including a surfactant acting as a structure-directing agent as is used to obtain pure silica mesoporous materials such as MCM-41 or SBA-15. Unlike mesoporous SiO
2-based materials, however, MBGs also contain other oxides such as CaO, or P
2O
5. The initial attempts to obtain MBGs composed of silicon, calcium and phosphorus oxides by the synthesis method of silica mesoporous materials failed because the procedure is performed at a pH that provokes calcium precipitation as calcium hydroxide. However, such synthesis can be carried out by using a method proposed by Brinker et al. [
33], the so-called evaporation induced self-assembly (EISA) method, where the solvent evaporation produces the required increase in the surfactant concentration until reaching the critical micellar concentration where the ordered mesophase is formed. In this way, the research groups led by Zhao [
34] and Vallet-Regí [
35], independently, opened a new avenue for the synthesis and characterization of this exciting family of BGs.
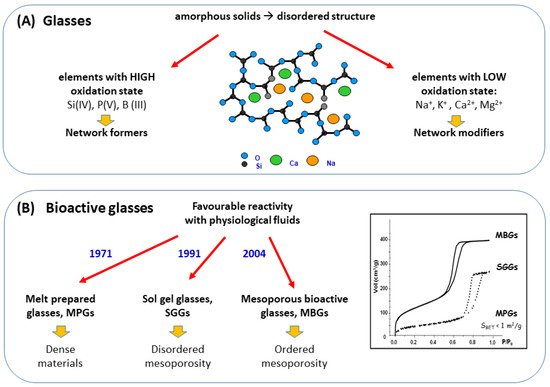
Figure 1A shows the main features of glasses which are amorphous materials with disordered structures at the atomic scale. As observed, glasses are formed by two types of oxides: elements with high oxidation state, such as Si (IV), P(V) or B(III), as the network formers; and elements with low oxidation state, such as alkaline (Na+, K+) and alkaline-earth (Ca2+, Mg2+) as network modifiers. These formers give glass stability under atmospheric conditions, confer specific properties and decrease the temperature of the synthesis process. Figure 1B, shows the most distinctive features of three families of BGs including the year of their initial synthesis.
Figure 1. Main features of: (A) glasses and (B) the three families of bioactive glasses.
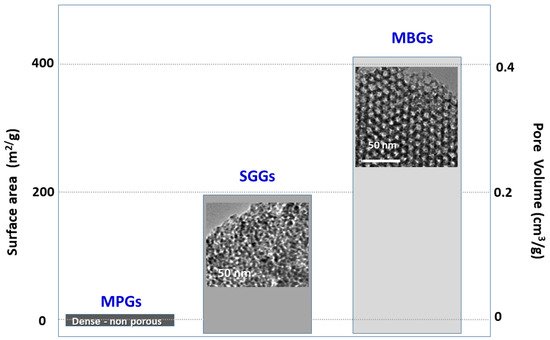
The textural properties, i.e., surface area and pore volume, of the three families of glasses, MPG, SGG and MBG, are compared in
Figure 2. As observed, MPGs are dense, non-porous materials with a minimum value of the surface area. On the other hand, SGGs and MBGs are both porous materials, but in the latter material, the mesopores are all of the same diameters and appear ordered. Moreover, the textural properties (surface area and pore volume) of MBGs are roughly twice those of SGGs. This feature is considered to be responsible for the greater bioactive kinetics of MBGs compared to SGGs and MPGs [
36]. TEM images of the SGG and of the MBG shown in the figure correspond both to glasses of the SiO
2–CaO–P
2O
5 system. The difference obtained lies in the synthesis method, the former was performed by the classical sol-gel method and the latter in the presence of a surfactant using the solvent evaporation induced self-assembly (EISA) method. As shown in the figure, mesopores of the SGG are disordered and exhibit different sizes. In contrast, an ordered arrangement of pores of the same size is observed in the MBG micrograph.
Figure 2. Textural properties of the three families of bioactive glasses. Transmission Electron Micrographs of the porous SGG and MBG are also included.
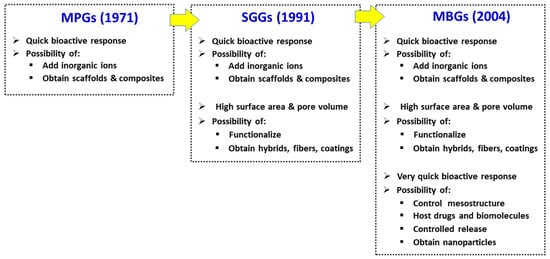
Figure 3 shows how the timeline development of the new families of BG has improved their properties for use in bone regeneration. MPG are excellent biomaterials for bone graft substitution due to their quick bioactive response, the capacity of hosting therapeutic inorganic ions and the possibility of their processing to obtain scaffolds and composites. In addition to the latter properties, SGGs offer other interesting features arising from their wet chemistry processing methods at low temperatures. First, the bioactivity improvement by including SiO
2 (up to 90 mol-%) as a result of their excellent textural properties. Wet chemistry methods were introduced in search of a surface richer in silanol groups but also resulted in glasses with high specific surface area and porosity. Furthermore, SGGs can be functionalized and biocompatible polymers can be added during their synthesis to obtain organic–inorganic hybrid materials (nanocomposites) [
37,
38,
39] with the desired mechanical or degradation properties. Additionally, by selecting the appropriate time during the sol to gel transition, it is possible to obtain coatings or fiber meshes of SGGs.
Figure 3. Main properties of the three families of BGs for bone regeneration applications.
MBGs, which can be considered an improvement of SGGs, have all the characteristics of MPGs and SGGs, but present other new features as a result of their synthesis in the presence of surfactants, producing a greater control of their mesostructure. This process produces advantageous textural properties as well as a much faster in vitro bioactive response than that of the other BGs family members [
11]. The large volume of monodisperse pores makes MBGs ideal candidates for hosting different molecules, which is essential for their putative applications in bone tissue engineering. However, the previously mentioned EISA method for MBG synthesis yields powders with limited biomedical applications, mainly as bone fillers, and other biomaterials of natural or synthetic origin are currently available as bone grafts in this regard. In contrast, processing MBG as 3D porous scaffolds with hierarchical porosity of different size scales has more interest for possible applications in regenerative medicine. Moreover, one of the currently most active areas of MBGs research concerns their use as nanocarriers of biologically active ions and therapeutic biomolecules [
40,
41]. This requires their synthesis as nanoparticles of variable size between 20 and 800 nm, and with a pore size tailored in the range 5–20 nm. However, this kind of MBG form still needs a great deal of research before it could be materialized into a clinical application. Indeed, there is still scarce preclinical research in animal models with MBGs. The current results are very promising, but several aspects still need to be elucidated before considering their putative clinical use: the ideal composition of the glass, the optimal resorption rate, the type and amount of therapeutic ions included, or the addition of different bioactive drugs presenting osteogenic, bactericidal, angiogenic, anticancer, anti-inflammatory, antioxidant and/or antiviral properties.
3. Bioactive Glasses in Bone Regeneration
In the 1980s, BGs based on the SiO
2–CaO–P
2O
5–Na
2O system were approved by the FDA for several maxillofacial and dental applications [
42]. Later on, their applications were extended to Orthopaedics as bone grafts in non-load bearing sites. Recent developments in the performance of these materials rely on new methods of synthesis to obtain materials specifically depicting an ordered mesoporosity, as described above [
34,
35]. Of interest in this respect, the structural and bioactive properties of MBGs provide their ability for loading a variety of osteogenic agents to improve their use as scaffolds in bone regeneration [
43,
44,
45]. Increasing evidence indicates that ionic dissolution from these glasses is key in their osteogenic behavior [
46]. Indeed, a variety of trace elements (Sr, Cu, Zn) present in the human body have anabolic bone activity [
47,
48]. Accordingly, MBGs based on SiO
2–CaO–P
2O
5 and containing distinct cations were designed according to the required clinical applications [
29,
49,
50]; this includes a recently reported P
2O
5-free borate glass porous scaffold with a high Ca content which shows both osteogenic and antimicrobial features [
12].
Sr is one of the various cations incorporated into ceramic biomaterials due to its well-characterized osteogenic properties: it has a dual role in inducing osteoblastogenesis by stimulating the osteogenic differentiation program while inhibiting adipogenesis from the common mesenchymal progenitor cell and decreasing osteoblast apoptosis in vitro. This is of particular interest when considering the high adiposity often observed in osteoporotic bone. In fact, strontium ranelate—an approved osteoporosis therapy—was shown to improve trabecular bone structure and prevent fracture in postmenopausal women [
51,
52,
53]. This cation appears to act, at least in part, through the CaSR in osteoblasts [
43]. Nanohydroxyapatites co-substituted with foreign ions such as Mg
2+ and CO
32− to mimic the composition of bone HA, and also Sr
2+ as an osteogenic signal and porous Sr-substituted calcium silicate ceramic scaffolds were developed as biomaterials to regenerate osteoporotic bone [
54,
55]. Moreover, using a canine gap model, incorporation of 5% Sr to an HA bone graft favored its fixation followed by healing of the gap possibly related to the anabolic and anticatabolic effects of the cation [
56]. In addition, adding Sr to either MBG scaffolds fabricated using a 3D printing method or bioactive glass/polycaprolactone (a resorbable polymer widely used in bone tissue engineering) composite scaffolds enhanced the osteogenic activity of the respective biomaterial without the cation [
57,
58]. Additionally of note, the incorporation of Sr to borate glass improved its bone growing action [
59]. Sr-stabilized bulk glass ceramics as the implant was shown to improve the healing of a bone defect in a rabbit model [
60]. Thus, Sr is being extensively used to dope various biomaterials including bioactive BGs as bone tissue engineering strategies for bone healing.
Cu is an essential element whose deficit produces osteopenia in humans [
61,
62]. This was related in part to the well-known role of Cu on the activity of antioxidant enzymes involved in the cross-linking of bone collagen fibers [
63]. Moreover, Cu has antimicrobial activity [
64,
65]. Recently, MBGs containing 2.5–5% CuO, synthesized using HNO
3 as catalyst and calcium and copper nitrates as CaO and CuO precursors, respectively, showed a rapid bioactive response (formation of an apatite-like layer) in simulated body fluid in vitro; an activity often related to the in vivo mineralization process [
66,
67]. Moreover, the capacity of these modified MBGs to release supraphysiological amounts of Ca
2+ and Cu
2+ ions and to host osteogenic agents in their pores make them interesting biomaterials for bone regeneration.
Zn is known to have angiogenic, osteogenic and bactericidal properties [
68,
69,
70]. Recently, MBGs of composition 80–x%SiO
2–15%CaO–5%P
2O
5 with 4–5% ZnO and manufactured as disks, were evaluated in pre-osteoblastic MC3T3-E1 cell cultures. Some of these materials were also loaded with the osteoinductive peptide osteostatin, a C-terminal peptide from parathyroid hormone-related protein [PTHrP (107–111)] [
7]. Interestingly, the simultaneous presence of Zn
2+ and osteostatin in these MBGs was found to potentiate their capacity to increase MC3T3-E1 cell growth and osteoblastic differentiation [
71]. Additional studies were subsequently carried out to further explore the suitability of this approach in bone regeneration. Thus, MBGs of the same composition were fabricated as 3D scaffolds, which showed optimal hierarchical porosity (from mesopores to macrospores), specific surface area and in vitro bioactivity for putative use as bone substitutes [
72]. Impregnation of these scaffolds with osteostatin enhanced their osteogenic capacity by promoting human mesenchymal cell (hMSC) colonization and proliferation. Furthermore, as observed with these materials as disks in MC3T3-E1 cell cultures, Zn
2+ and osteostatin together in the scaffolds induced several osteoblast differentiation genes and mineralization in hMSCs without the addition of other osteogenic differentiation-promoting factors [
72]. Therefore, osteostatin was confirmed to enhance the osteogenic capacity of Zn
2+-enriched MBGs.
As a preclinical approach, similar scaffolds [with composition (mol %) 82.2SiO
2–10.3CaO–3.3P
2O
5–4.2ZnO were coated with gelatin that facilitates both their handling and the release of inorganic ions and peptides, and were then evaluated as implants in two rabbit models of bone regeneration. These scaffolds, containing or not osteostatin and hMSCs, were implanted into bone defects (7.5 mm diameter, 12 mm depth) drilled in the distal femoral epiphysis of New Zealand rabbits [
73]. Three months thereafter, the presence of osteostatin and hMSCs in the implanted scaffold significantly improved bone healing by inducing implant degradation, reducing the fibrous cup observed with the raw scaffolds and increasing trabecular bone volume density [
73]. These recent findings give credence to the notion that these functionalized MBG scaffolds might be considered as a new interesting approach in bone tissue engineering.