2. Neurological Consequences due to hRSV Infection
The hRSV-infection not only affects the respiratory tract but can also develop neurological manifestations, which might lead in some cases to long-term neurological sequels [
19]. Since the infection with hRSV promotes a more severe disease in infants, the neurological complications that this virus can produce are generally studied in this population [
6,
19]. In this section, it will be discussed the consequences related to the infection with hRSV on the CNS.
The neurological complications in infants infected by hRSV were firstly reported during a study performed on febrile infants in 1970 [
77]. Among these infants, the patients infected with hRSV presented facial palsy and hemiplegia [
77]. To date, several reports indicate that the infection with hRSV on infants can lead to the development of ataxia, febrile or epileptic state, encephalitis, and encephalopathies, among other symptoms [
19,
78,
79,
80,
81]. Among these patients with neurological symptoms, the genetic material of hRSV was found on the cerebrospinal fluid (CSF) and presented elevated cytokines [
82,
83]. The percentage of acute encephalitis or encephalopathy cases in infants due to the infection with hRSV can reach up to 6.5% [
84]. Unfortunately, not all children can recover entirely from the neurological symptoms, and even 7% of the cases result in the death of the patient [
84]. Recently, a rare manifestation that contributes to neurological symptoms due to the infection with hRSV was reported [
85]. In this report, the two-month-old infant infected by hRSV developed seizures, encephalopathy, and the syndrome of inappropriate antidiuretic hormone secretion (SIADH) [
85]. The follow-up performed ten months after the onset of the symptoms showed problems in the patient regarding neuromotor development, mobility, and visual functions [
85].
The neuropathologies caused by a viral agent can lead to long-term sequels, such as cognitive and psychiatric disorders, even after the infection has been cleared [
86]. In the case of hRSV, patients infected with the virus might develop neuromotor impairment, as previously mentioned, or present learning impairment [
85,
87]. Among the learning complications reported for hRSV positive cases, a study evaluated the difficulties in learning the native language of infants that suffered from a severe infection within their first six-month-old [
87]. During this study, it was observed that patients with severe hRSV-infection under six months of age lead to poor differentiation between native and non-native phonetic, associating the lack of ability to learn the language with memory impairments [
87]. Even more, this phenotype lasted up to twelve-month-old and was associated with a detrimental development of communication abilities [
87]. A possible explanation for these cognitive consequences comes from a case of an infant infected with hRSV who showed abnormal magnetic resonance imaging (MRI) regarding the hippocampus, which is a zone of the brain that plays a significant role in long-term memory. Its damage contributes to long-term memory impairments [
88,
89]. Since the ability to learn a language and phonetics is performed through short- and long-term memory [
90], it can be suggested that hRSV could have infected the cells located in the hippocampus, which affected the long-term memory, leading to learning language impairment.
Based on what was previously described, it has been suggested that the hippocampus might be involved in developing long-term neurologic consequences due to the infection with hRSV, and in vivo studies were able to demonstrate it [
91]. This in vivo study showed that hRSV could reach the brain and be detected in several brain zones, such as the olfactory bulb, cortex, hippocampus, and ventromedial hypothalamic nucleus [
91]. The evaluation of the long-term learning impairment was through the Morris water maze (MWM), which demonstrated that 30 days post-infection with hRSV, the rats developed difficulties in spatial learning capacities [
91]. It was also shown that the rats infected with hRSV presented a defective long-term potentiation (LTP) response, which is a process that potentiates the long-lasting signaling between the CA
3 and CA
1 neurons in the hippocampus [
91,
92]. This finding provided valuable information regarding the brain region that might be responsible for the long-term memory consequence of the infection with hRSV [
91].
Additionally, in vivo studies evaluated the behavioral impairment through the Marble Burying test (MB), which measures the spontaneous and natural behavior of the mice related to the ventral hippocampus function [
17,
91]. These studies demonstrated that behavioral impairment in the infected mice could be present from 30 to 60 days post-infection with hRSV [
17,
91]. However, at 90 days post-infection, the mice infected with hRSV showed similar behavior to the control [
17,
91]. Interestingly, the infection with hRSV modifies the permeability of the blood-brain barrier (BBB) of the mice, which leads to the infiltration of immune cells into the brain and an increased level of pro-inflammatory cytokines, possibly contributing to the behavioral alterations on the mice infected with hRSV [
17].
Since it has been established that hRSV is capable of infecting different types of cells from the placenta of pregnant women and cells of the fetus, such as Hofbauer cells [
42], it can be suggested that the infection can be passed on to the fetus and cause detrimental development of the CNS from the fetus. These problems in the development of the CNS might make the infants more susceptible to developing neurological symptoms and long-term neurological sequels after infection with hRSV, such as memory and behavioral impairment (
Figure 2) [
19,
87]. Therefore, this option needs to be further evaluated.
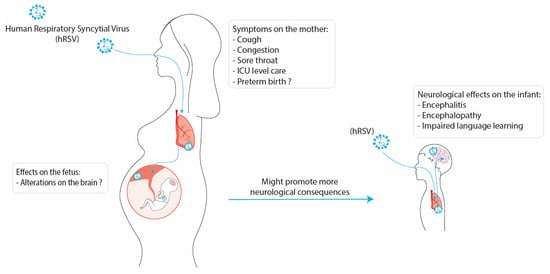
Figure 2. Possible consequences of the infection with hRSV during pregnancy on the fetus and infant. The infection with hRSV on a pregnant woman can develop mild symptoms such as cough, congestion, and in the more severe cases, the mother might need ICU-level care. Additionally, the infection with hRSV has been associated with preterm birth. This infection might cause alterations in the development of the fetus and promote more cases of neurological consequences on the infants, which can develop encephalitis, encephalopathy, and impaired language learning.
3. Conclusions
Respiratory infections are a public health problem that causes high rates of hospitalization worldwide every winter season. According to this, hRSV is responsible for ALTRI leading to morbidity and mortality principally in infants and the elderly [
1,
2]. Besides the knowledge about the hRSV infection in the risk population usually studied, pregnant women have shown that they can suffer a severe respiratory illness caused by hRSV with poorly studied consequences [
22,
34,
93].
Importantly, recent evidence shows that hRSV can infect placental cells, cross the placental barrier, and, therein, be vertically transmitted to the fetus [
18,
24,
40]. One of the unknown relevant issues is the MIA effect on hRSV infection, which is essential since MIA has been associated with cognitive and behavioral impairment and neuropsychiatric illnesses such as SCZ and ASD [
32,
53,
57,
94]. The critical information about the harmful effect of MIA on the neurodevelopment of the fetus with neurological consequences in adulthood came from the Poly: IC model, which provides valuable evidence of the alteration of neurotransmitters pathways and cytokines expression that affect brain development [
95,
96]. However, this model cannot be extrapolated to a specific viral infection in humans. What is known is that the Influenza virus, which infects pregnant women and impacts the fetus principally in the second and third trimester of pregnancy, can trigger MIA in animal models [
69,
97]. Accordingly, prenatal Influenza virus infections increase maternal cytokines promoting an imbalance in the fetus cytokines that alter the normal neurodevelopment and neurotransmitters signaling, as was observed in SCZ and ASD [
31,
50].
Regarding the role of MIA in hRSV infection and its impact on the fetus, no studies have been performed. The current knowledge about the hRSV and neurological alterations came from reports showing that patients with hRSV infection have seizures, encephalitis, and encephalopathies [
19,
98,
99]. Besides, elevated cytokines and viral RNA were found in CSF from patients with neurological manifestations [
82,
83]. In this context, evaluations of the neurological effects of hRSV infection in animal models showed that viral RNA and proteins could be detected in the brain of infected animals [
91]. Additionally, the hRSV infection induces an increase in the BBB permeability, allowing the infiltration of immune cells and increased levels of cytokines in the brain of infected animals [
17]. Cognitive and behavioral impairments were observed 30 to 60 days post-infection, which could be explained by the possible hRSV effect on infected CNS cells [
17]. Due to these results, the first study regarding the possible neurological effects of the hRSV infection was conducted in infants was impairment of language acquisition impairment was found [
87]. All these data showed the potential harm that the hRSV infection could be for normal brain development, but there is not enough research in this field.
Importantly, antibodies generated against a virus can be passed towards the offspring, and by doing so, they can confer neurological protection to the fetus [
99]. This neuroprotection is achieved since the antibodies can reach the placenta and spread via the umbilical cord to the CNS on the fetus, accumulating these antibodies on the neural tissue [
99]. Based on this, the possibility of immunizing women during pregnancy is an area that needs to be evaluated as a possible solution to avoid possible neurological consequences on the infant.