Orthodontic mini-implants (MIs), also called temporary anchorage devices (TADs), have been considered to be effective tools for intraoral anchorage reinforcement for many years. Their main advantages are their easy application, the possibility to use them at various stages of treatment and the predictability of biomechanical effects.
- guided insertion
- surgical guide
- orthodontics
- mini-implant
1. Introduction
Optimal positioning of the screw, taking into account root proximity [7], bone support as well as soft tissue thickness and quality, intends to avoid most complications [8]. For this purpose, surgical templates were introduced. In the glossary of prosthodontic terms, a surgical template is defined as a guide used to assist in the proper surgical placement and angulation of dental implants [9]. The main purpose of the surgical template is to direct drilling and ensure accurate implant placement according to the treatment plan. In order to accurately transfer the implant directly the surgical site, custom surgical templates based on radiological diagnostics have become the treatment of choice [10]. Miniscrew insertion using a surgical guide aims to avoid possible adverse effects or complications. A significant reduction of the failure rate was noticed when using detailed radiological diagnostics of the insertion site, nevertheless a two-dimensional X-ray is considered as sufficient for routine procedures [11]. However, some authors are of the opinion that it is necessary to perform CBCT on or before placing TADs in patients with severe space deficiency, significant tooth crowding, or extraordinary root position on panoramic radiographs [12]. At the turn of the century, wire guides, based on a periapical X-ray gained popularity [13], and they have been used successfully until now by many clinicians, especially if advanced diagnostic tools are unavailable [14]. With the higher availability of both 3D imaging and printing, 3D surgical guides, for which the effectiveness has been well documented in implantology, they have been used more frequently [15,16]. For many clinicians, they seem to present a new avenue, and are even seen as a new remedy for possible complications that may occur during MI insertion. However, they do not take into account key factors such as lack of operator experience, manufacturing costs of template fabrication, the influences of which have already been examined in the case of prosthetic dental implants [17,18]. Therefore, it seems justified to examine the validity of surgical-templates use, which may contribute a discussion on other aspects of guided insertion of temporary anchorage in orthodontics.
2. Meta-Analysis
- (a)
-
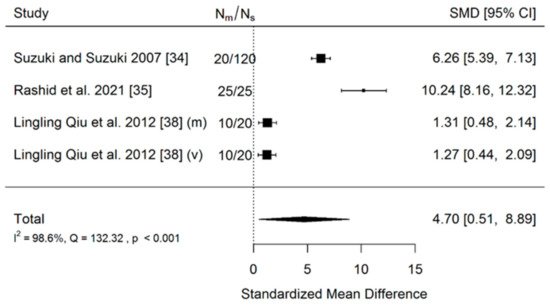
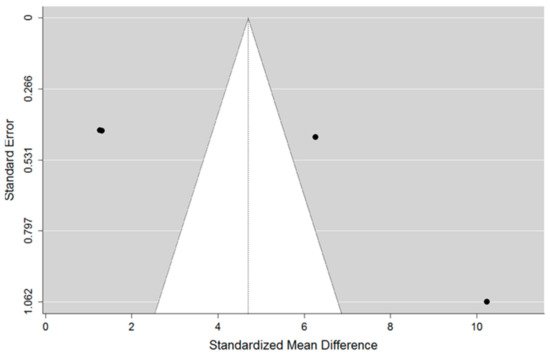
Accuracy of insertion of mini-implants using a 3D surgical guide to these inserted manually (no-guide). Three studies were included in the meta-analysis. The total sample size of all included studies was 220 implants.
- (b)
-
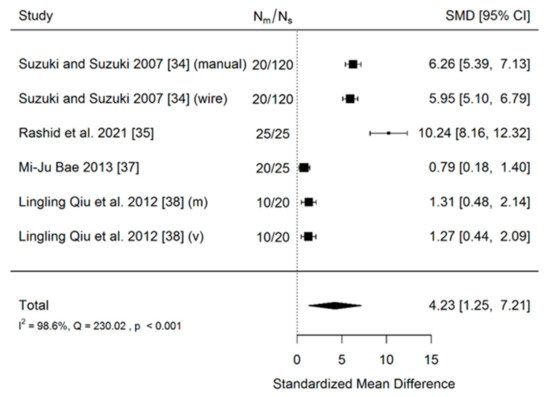
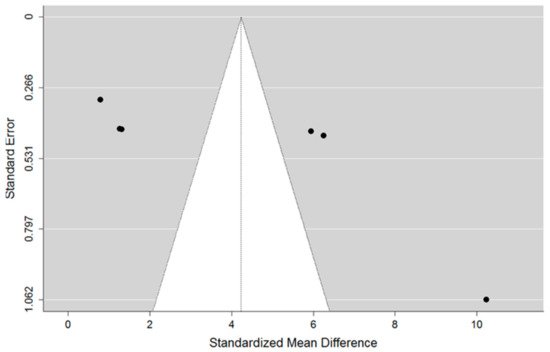
Accuracy of insertion of mini-implants using a 3D surgical guide in comparison to those inserted using a less-advanced method (manually and wire guides combined). There were four included studies in meta-analysis. The total sample size of all included studies was 285 implants.
- (c)
-
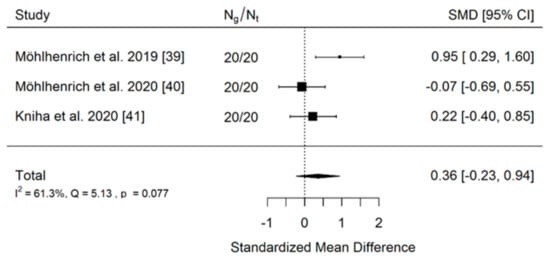
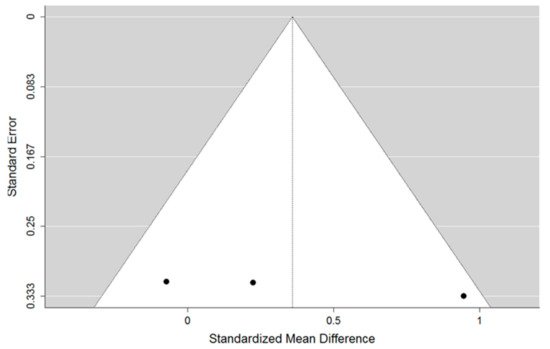
Accuracy of insertion of mini-implants using a tooth-borne 3D surgical guide to these inserted using mucosa-borne ones. Three studies were included in the meta-analysis. The total sample size of all included studies was 120 implants.
| Author and Year | Deviation in the Group with the Use of Surgical Guide | Deviation in the Group Where Implant Was Inserted Manually | ||
|---|---|---|---|---|
| No. of Implants | Values in mm | No. of Implants | Values in mm | |
| Suzuki and Suzuki, 2007 [34] | 120 | 2.0 ± 0.4 mm | 20 | 10.5 ± 3.5 mm |
| Rashid et al., 2021 [35] | 25 | 0.69 ± 0.02 mm | 25 | 1.44 ± 0.10 mm |
| Lingling Qiu et al., 2012 [38] | 20 | 0.28 ± 0.23 mm (mesiodistal) 0.33 ± 0.25 mm (vertical) |
10 | 0.81 ± 0.61 mm (mesiodistal) 0.78 ± 0.49 mm (vertical) |
| Author and Year | Deviation in the Group with the Use of Surgical Guide | Deviation in the Group Where Implant Was Inserted Manually or with Wire Guide | ||
|---|---|---|---|---|
| No. of Implants | Values in mm/Root Contact Rate | No. of Implants | Values in mm/Root Contact Rate | |
| Suzuki and Suzuki, 2007 [34] | 120 | 2.0 ± 0.4 mm | 20 | 10.5 ± 3.5 mm |
| Suzuki and Suzuki, 2007 [34] | 120 | 2.0 ± 0.4 mm | 20 | 5.3 ± 1.1 mm |
| Rashid et al., 2021 [35] | 25 | 0.69 ± 0.02 mm | 25 | 1.44 ± 0.10 mm |
| Mi-Ju Bae, 2013 [37] | 25 | 0.73 mm (0.24–2.07) | 20 | 1.28 mm (0.26–3.81) |
| Lingling Qiu et al., 2012 [38] | 20 | 0.28 ± 0.23 mm (mesiodistal) 0.33 ± 0.25 mm (vertical) |
10 | 0.81 ± 0.61 mm (mesiodistal) 0.78 ± 0.49 mm (vertical) |
| Author and Year | Deviation in the Group with a Tooth-Borne Surgical Guide | Deviation in the Group with a Mucosa-Borne Surgical Guide | ||
|---|---|---|---|---|
| No. of Implants | Values in Linear Deviation in mm | No. of Implants | Values in Linear Deviation in mm | |
| Möhlhenrich et al. 2019 [39] | 20 | 0.88 ±0.46 mm | 20 | 1.65 ± 1.03 mm |
| Möhlhenrich et al. 2020 [40] | 20 | 1.7 ± 1.2 mm | 20 | 1.6 ± 1.5 mm |
| Kniha et al. 2020 [41] | 20 | 0.10 ± 0.46 mm | 20 | 0.22 ± 0.58 mm |
- (a)
-
The first comparison
- (b)
-
The second comparison
- (c)
-
The third comparison
This entry is adapted from the peer-reviewed paper 10.3390/coatings11121488