The coronavirus disease 2019 (COVID-19) pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has had a widespread impact on health, including a substantial mortality among patients with various pre-existing health conditions. Patients with cardiovascular disease (CVD) are more susceptible to the development of severe COVID-19 infection. The incidence of mechanical complications of acute coronary syndrome (ACS) increased fivefold after the declaration of a state of emergency in Japan. Therefore, vaccination against SARS-CoV-2 is generally recommended in patients with CVD, as is vaccination against other infectious agents. The BNT162b2 mRNA COVID-19 vaccine has shown promising efficacy and safety, mainly in people without apparent pre-existing comorbidities. A nationwide mass vaccination study focused on the estimated vaccine effectiveness of patients with various comorbidities such as heart disease. No data, however, are available regarding the vaccine effectiveness in patients with CVD alone. So it's necessary to investigate the humoral response of patients with CVD to the BNT162b2 mRNA COVID-19 vaccine compared to that in healthcare workers (HCWs).
1. Analysis on Results
1.1. Baseline Characteristics of the Study Participants
The demographics and clinical characteristics of the participants are summarized in Table 1. A total of 264 participants were enrolled in this study: 85 patients with CVD (median (interquartile range) age, 74 (68–77) years; 67 men) and 179 HCWs (49 (41–55) years; 58 men). Among patients, the most common diagnosis was coronary artery disease (53 patients (63%)), followed by arrhythmia (9 patients (11%)) and hypertensive heart disease (10 patients (12%)). Intervals between the first and second dose of vaccinations and serum sampling were comparable between patients (14.7 ± 1.9, 14.9 ± 1.7 days) and HCWs (14.7 ± 1.7, 14.3 ± 1.6 days).
Table 1. Baseline characteristics of the study participants.
| |
Patients (n = 85) |
HCWs (n = 179) |
| Age, y |
74 (68–77) |
49 (41–55) |
| Male |
67 (79) |
58 (32) |
| Hypertension |
56 (66) |
16 (9) |
| Dyslipidemia |
58 (68) |
5 (3) |
| Diabetes |
26 (31) |
1 (1) |
| Allergic disease |
8 (9) |
86 (48) |
| Diagnosis |
| Coronary artery disease |
53 (63) |
NA |
| Arrhythmia |
9 (11) |
| Hypertensive heart disease |
10 (12) |
| Cardiomyopathy |
6 (7) |
| Aortic dissection or aneurysm |
4 (5) |
| Valvular disease |
3 (4) |
| Previous myocardial infarction |
26 (31) |
| Previous coronary revascularization |
38 (45) |
| Paroxysmal or persistent AF |
12 (14) |
| Medications |
| RAAS inhibitors |
41 (48) |
NA |
| Beta-blockers |
34 (40) |
| Diuretics |
8 (9) |
| Statins |
46 (54) |
| Antiplatelet drugs |
37 (44) |
| Anticoagulant drugs |
16 (19) |
| Intervals between the first vaccination and sampling, day |
14.7 ± 1.9 |
14.7 ± 1.7 |
| Intervals between the second vaccination and sampling, day |
14.9 ± 1.7 |
14.3 ± 1.6 |
1.2. Seropositivity after Vaccination
Among all participants, 188 (71%) were seropositive for RBD−IgG (>0.86 U/mL) at 14 days after the prime dose. The prevalence of seropositivity in patients with CVD after the prime dose was significantly lower compared to that of HCWs (21% vs. 95%, p < 0.001). After adjusting for covariables, patients with CVD (compared to HCWs) were associated with a low positive serological response (Table 2). All participants had developed a positive antibody response by 14 days after the booster dose.
Table 2. Multivariable logistic analysis of seropositive status after first vaccination.
| Variables |
Univariable Analysis |
Multivariable Analysis |
| |
Odds Ratio |
95% CI |
p Value |
Odds Ratio |
95% CI |
p Value |
| Patients with CVD (vs. HCWs) |
0.01 |
0.01 to 0.03 |
<0.001 |
0.08 |
0.02 to 0.33 |
<0.001 |
| Age (per 1 year increment) |
0.86 |
0.82 to 0.89 |
<0.001 |
0.95 |
0.90 to 0.99 |
0.02 |
| Male |
0.19 |
0.10 to 0.34 |
<0.001 |
0.78 |
0.30 to 2.00 |
0.61 |
| Allergic disease |
5.33 |
2.58 to 11.0 |
<0.001 |
1.16 |
0.39 to 3.45 |
0.79 |
| Hypertension |
0.09 |
0.05 to 0.16 |
<0.001 |
0.60 |
0.21 to 1.74 |
0.35 |
| Dyslipidemia |
0.05 |
0.03 to 0.10 |
<0.001 |
0.88 |
0.26 to 2.95 |
0.84 |
| Diabetes |
0.07 |
0.02 to 0.19 |
<0.001 |
0.63 |
0.19 to 2.10 |
0.45 |
1.3. Antibody Titers after Vaccination
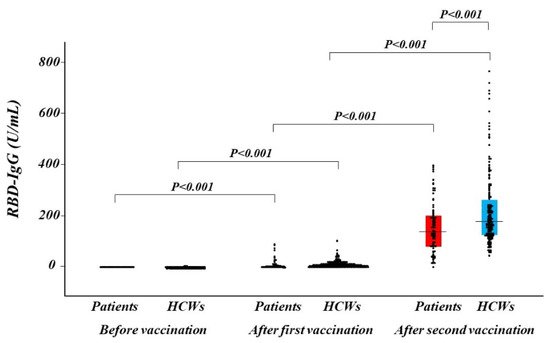
RBD−IgG titers at 14 days after the prime and booster doses increased compared with pre-vaccination and dramatically increased after the booster dose in both the patient and HCW groups (Figure 1). Median RBD−IgG titers at 14 days after the booster were significantly lower in patients with CVD than in HCWs (137.2 U/mL (80.6–200.4 U/mL) vs. 176.2 U/mL (123.9–260.0 U/mL), p < 0.001). In a multivariable regression analysis, there was a significant association between patients with CVD (compared to HCWs) and low RBD−IgG titers after the booster dose (Table 3).
Figure 1. Distribution of antibody titer. Humoral quantitative IgG against SARS-CoV-2 spike RBD response at before vaccination, after the first and the second of vaccination in patients with CVD (red box) and in HCWs (blue box). The dots depict antibody levels. A box represents interquartile range and a horizontal line in a box represents the median. CVD, cardiovascular disease; HCWs, healthcare workers; RBD, receptor-binding domain; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Table 3. Multivariable regression analysis of RBD−IgG titers after a complete cycle of vaccination.
| Variables |
Univariable Analysis |
Multivariable Analysis |
| |
β Coefficient |
95% CI |
p Value |
β Coefficient |
95% CI |
p Value |
| Patients with CVD (vs. HCWs) |
−0.22 |
−0.34 to −0.10 |
<0.001 |
−0.32 |
−0.60 to −0.04 |
0.02 |
| Age (per 1 year increment) |
−0.14 |
−0.27 to −0.02 |
0.03 |
0.12 |
−0.08 to 0.31 |
0.25 |
| Male |
−0.22 |
−0.34 to −0.10 |
<0.001 |
−0.17 |
−0.30 to −0.03 |
0.02 |
| Hypertension |
−0.21 |
−0.33 to −0.08 |
0.001 |
−0.17 |
−0.34 to 0.01 |
0.06 |
| Dyslipidemia |
−0.14 |
−0.26 to −0.01 |
0.03 |
0.17 |
−0.03 to 0.38 |
0.10 |
| Diabetes |
−0.14 |
−0.26 to −0.01 |
0.03 |
−0.04 |
−0.18 to 0.10 |
0.60 |
2. Current Insights on BNT162b2 mRNA COVID-19 Vaccine
Impaired immunogenicity of the BNT162b2 mRNA COVID-19 vaccine has been reported in immunocompromised patients treated for solid tumors [
8] and with solid organ transplantation [
9,
10,
11]. However, the efficacy of the BNT162b2 mRNA COVID-19 vaccine in patients with heart disease has never been investigated. To the best of our knowledge, this is the first study to document a blunt response after a complete cycle of the BNT162b2 mRNA COVID-19 vaccine in patients with CVD.
COVID-19 vaccines demonstrate excellent efficacy in clinical trials [
4,
5] and effectiveness in real-world data [
6], but some individuals still become infected with SARS-CoV-2 after vaccination. A recent study demonstrated that in older adults (≥60 years) who had received their first vaccine dose but not their second, heart disease was associated with post-vaccination infection [
12]. Our data showed an inferior serological response to the COVID-19 vaccine after the first vaccine dose, which may be associated with susceptibility to COVID-19 infection after vaccination in patients with heart disease. Therefore, these patients may be highly recommended to receive the complete cycle of the COVID-19 vaccine. Hall et al. reported an increment in the immunogenicity of the COVID-19 vaccine with administration of a third dose in transplant recipients [
13]. Our results demonstrated that patients with CVD had lower antibody levels after a booster dose compared to HCWs, suggesting that these patients should be prioritized to receive the third dose of vaccination.
In this study, differences in age and gender were observed between CVD patients and HCWs. Older age has been repeatedly reported to associate with reduced antibody responses after COVID-19 vaccination [
14,
15,
16]. Female gender has also been shown to correlate with antibody responses to COVID-19 vaccination to various degrees [
17]. These differences may make it difficult to evaluate the humoral response to COVID-19 vaccination in patients with CVD. In multivariate analyses, however, CVD was independently associated with seropositivity after the first vaccination and RBD−IgG titers after the second vaccination. Furthermore, when we performed multivariate analyses in a subgroup of 16 HCWs over 60 years (median age 65 years; male, 63%) and patients with CVD, similar results were obtained (data not shown). Consequently, we believe that these factors did not significantly affect our results. The mechanisms that emphasize the association between CVD and a poor humoral response to the BNT162b2 mRNA COVID-19 vaccine are still unclear. It is possible that the medications used may be associated with poorer humoral response in patients with CVD. In the present study, there were no significant differences in humoral response according to their medications, such as renin–angiotensin–aldosterone system inhibitors, beta-blockers, and statins. Further investigations are required to clarify this issue.
To date, some COVID-19 vaccines have been approved for emergency use. Diverse platforms have been used to deliver the recombinant SARS-CoV-2 spike, such as mRNA-encapsulating liposomes, adenovirus vectors, and micelle-attached spikes [
18]. The humoral response may be different according to the type of vaccine. A notable loss of vaccine efficacy against SARS-CoV-2 variants is reported, likely caused by spike mutations in the RBD, N-terminal domain, and other regions [
19,
20]. It may be necessary to investigate the neutralizing antibody against variants of SARS-CoV-2.
This entry is adapted from the peer-reviewed paper 10.3390/jcm10235498