The use of interpreters in medical education as part of the curriculum is scarce, but students have been trained in how to work with interpreters when interviewing patients to fully develop their skills. This entry discusses about the relevant literature on the use of interpreters in medical and healthcare education.
- interpreters
- medical education
- educational and health outcomes
- cultural competence
1. Introduction
Medical doctors practice medicine in multicultural societies and are expected to exercise cultural competence, such as working with interpreters in order to provide the best quality of care to their patients [1][2][3][4]. There are many definitions of cultural competence, although it generally refers to knowledge regarding social and cultural factors that affect health and illness and to actions necessary for the provision of quality and accessible care [1][2]. The need for cultural competence has been recognized in literature as it may reduce health disparities [2], and doctors can improve their skills and knowledge in this area of practice [5]. Research has shown that cultural competence is associated with increased patient satisfaction and adherence to therapy [1][6] and has helped physicians enhance their cultural sensitivity [7].
Despite these findings, the integration of cultural competence in medical curricula has been underdeveloped [4][8]. Alizadeh and Chavan [1] found 18 models of cultural competence, with many training paradigms for medical practitioners revealing a link between cultural competence and enhanced patient satisfaction and adherence to therapy. However, none of these models were specifically tailored for education purposes. [9] also highlighted the importance of cultural issues and the need to integrate cultural competence in medical curricula.
One aspect of cultural competence is to work effectively with people with limited command of the language spoken by health care professionals and to recruit interpreters to assist with this task. However, Himmelstein, Wright, and Wiederman [10] explained that there is negligible evidence about medical students working with interpreters within the medical curricula. Third, are undergraduate medical/health care students provided with training on how to use interpreters in health care consultations when they graduate? However, one might say that if students are taught how to use professional interpreters when interviewing patients, they might be able to use the knowledge and skills when they are provided with interpreters at their clinical placements.
Based on a gap identified by Wright and Wiederman [10] and on the questions above, this study focuses on understanding the extent of interpreter utilization in medical education as part of the curriculum and its effects on educational and health outcomes.
2. Two Overarching Themes
2.1. Use of Interpreters during Undergraduate Medical/Health Care Curricula
-
The trainee asked the patient one question at a time.
-
The trainee presented information at a pace that was easy to follow for both patient and interpreter—that is, information was given in digestible chunks
-
The trainee addressed the patient as “you” and not as “he” or “she.”
-
The trainee appropriately closed the encounter: at a minimum, asked the patient if he or she had any questions.
-
Asked patient one question at a time
-
Addressed patient directly
-
Maintained direct eye contact with patient
-
Listened to interpreter without unnecessary interruption
-
Asked interpreter questions about incomplete interpretations
-
Spoke in short, simple sentences with pauses for interpretation
2.2. Developing Students’ Skills through Training in How to Use Interpreters in Health Care Interviews or Consultations
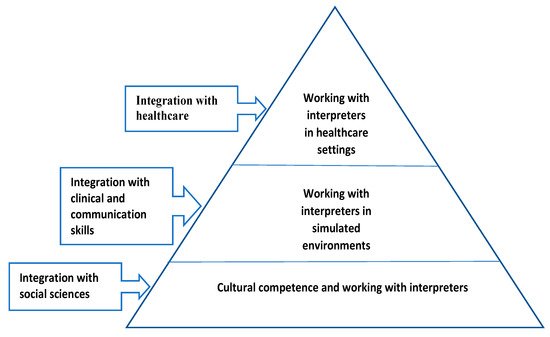
3. Framework for Integrating Interpreting Services in Medical Education
This entry is adapted from the peer-reviewed paper 10.3390/soc11030070
References
- Alizadeh, S.; Chavan, M. Cultural competence dimensions and outcomes: A systematic review of the literature. Health Soc. Care Community 2016, 24, 117–130.
- Betancourt, J.; Green, A.R.; Carrillo, J.E.; Ananeh-Firempong, O. Defining cultural competence: A practical framework for addressing racial/ethnic disparities in health and health care. Public Health Rep. 2003, 118, 293–302.
- Constantinou, C.S.; Papageorgiou, A.; Andreou, P.; McCrorie, P. How to integrate cultural competence in medical curricula: Learning from a new medical programme. MedEdPublish 2020, 9.
- Constantinou, C.S.; Papageorgiou, A.; Samoutis, G.; McCrorie, P. Acquire, apply, and activate knowledge: A pyramid model for teaching and integrating cultural competence in medical curricula. Patient Educ. Couns. 2018, 101, 1147–1151.
- Borrell-Carrió, F.; Suchman, A.L.; Epstein, R.M. The Biopsychosocial Model 25 Years Later: Principles, Practice, and Scientific Inquiry. Ann. Fam. Med. 2004, 2, 576–582.
- Horvat, L.; Horey, D.; Romios, P.; Kis-Rigo, J. Cultural competence education for health professionals. Cochrane Database Syst. Rev. 2014, CD009405.
- Renzaho, A.M.N.; Romios, P.; Crock, C.; Sonderlund, A.L. The effectiveness of cultural competence programs in ethnic minority patient-centered health care--a systematic review of the literature. Int. J. Qual. Health Care 2013, 25, 261–269.
- Hudelson, P.; Dogra, N.; Hendrickx, K.; Verdonk, P.; Essink-Bot, M.-L.; Suurmond, J. The challenges of integrating cultural competence into undergraduate medical curricula across Europe: Experience from the C2ME “Culturally competent in medical education” project. MedEdPublish 2016, 5.
- Sorensen, J.; Jervelund, S.S.; Norredam, M.; Kristiansen, M.; Krasnik, A. Cultural competence in medical education: A questionnaire study of Danish medical teachers’ perceptions of and preparedness to teach cultural competence. Scand. J. Public Health 2017, 45, 153–160.
- Himmelstein, J.; Wright, W.S.; Wiederman, M.W. U.S. medical school curricula on working with medical interpreters and/or patients with limited English proficiency. Adv. Med. Educ. Pract. 2018, 9, 729–733.
- Itaya, L.E.; Glassman, P.; Gregorczyk, S.; Bailit, H.L. Dental School Patients with Limited English Proficiency: The California Experience. J. Dent. Educ. 2009, 73, 1055–1064.
- Simon, L.; Hum, L.; Nalliah, R. Training to care for limited English proficient patients and provision of interpreter services at US dental school clinics. J. Dent. Educ. 2017, 81, 169–177.
- Omoruyi, E.A.; Dunkle, J.; Dendy, C.; McHugh, E.; Barratt, M.S. Cross Talk: Evaluation of a Curriculum to Teach Medical Students How to Use Telephone Interpreter Services. Acad. Pediatr. 2018, 18, 214–219.
- Mazori, A.; Maron, M.; Osterbur, M.; Santos, D.; Marco, V.; Lin, J.; Cortijo, A.; Nosal, S.; Schoenbaum, E. Enhancing Medical Stu-dent-Interpreter Collaboration in an Urban Free Clinic. Fam. Med. 2019, 51, 593–597.
- Kalet, A.; Gany, F.; Senter, L. Working with interpreters: An interactive Web-based learning module. Acad. Med. 2002, 77, 927.
- Kalet, A.L.; Mukherjee, D.; Felix, K.; Steinberg, S.E.; Nachbar, M.; Lee, A.; Changrani, J.; Gany, F. Can a web-based curriculum improve students’ knowledge of, and attitudes about, the interpreted medical interview? J. Gen. Intern. Med. 2005, 20, 929–934.
- Lie, D.; Bereknyei, S.; Kalet, A.; Braddock, C., 3rd. Learning outcomes of a web module for teaching interpreter interaction skills to pre-clerkship students. Fam. Med. 2009, 41, 234–235.
- Fung, C.-C.; Lagha, R.R.; Henderson, P.; Gomez, A.G. Working with interpreters: How student behavior affects quality of patient interaction when using interpreters. Med. Educ. Online 2010, 15, 5151.
- Lie, D.A.; Bereknyei, S.; Vega, C.P. Longitudinal development of medical students’ communication skills in interpreted en-counters. Educ. Health 2010, 23, 466.
- Avalos, O.H.; Pennington, K.; Osterberg, L. Revolutionizing Volunteer Interpreter Services: An Evaluation of an Innovative Medical Interpreter Education Program. J. Gen. Intern. Med. 2013, 28, 1589–1595.
- Bansal, A.; Swann, J.; Smithson, W. Using professional interpreters in undergraduate medical consultation skills teaching. Adv. Med. Educ. Pract. 2014, 5, 439–450.
- Quick, K.K.; Selameab, T.; Woll, A.; Mazzei, C.; Miller, J.L. Creating and Evaluating Skills-Based Training in Working with Spoken-Language Interpreters for Oral Health Professions Students. J. Dent. Educ. 2019, 83, 645–653.
- McEvoy, M.; Santos, M.T.; Marzan, M.; Green, E.H.; Milan, F.B. Teaching medical students how to use interpreters: A three year experience. Med. Educ. Online 2009, 14, 4507.
- Ikram, U.Z.; Essink-Bot, M.-L.; Suurmond, J. How we developed an effective e-learning module for medical students on using professional interpreters. Med. Teach. 2014, 37, 422–427.
- Marion, G.S.; Hildebrandt, C.A.; Davis, S.W.; Marín, A.J.; Crandall, S.J. Working effectively with interpreters: A model curriculum for physician assistant students. Med. Teach. 2008, 30, 612–617.
- Jacobs, E.A.; Diamond, L.C.; Stevak, L. The importance of teaching clinicians when and how to work with interpreters. Patient Educ. Couns. 2010, 78, 149–153.
- Aitken, G. Medical Students as Certified Interpreters. AMA J. Ethics 2019, 21, 232–238.
- Mihalic, A.P.; Morrow, J.B.; Long, R.B.; Dobbie, A.E. A validated cultural competence curriculum for US pediatric clerkships. Patient Educ. Couns. 2010, 79, 77–82.