1. The Era of Cannabis sativa, Cannabinoids, and the Endocannabinoid System: A Long Journey Traveled
The
Cannabis sativa era has a long and remarkable history dating from prehistoric Xinjiang, an ancient Chinese place, where users consumed
Cannabis not only for religious/spiritual or hedonic purposes but also for its medicinal effects [
1,
2,
3]. The first report of hemp medicinal use comes from Chinese medicine, around 2300 B.C. In India,
Cannabis became part of the Hindu religion, being subsequently introduced to Europe between 1000 and 2000 B.C. Long after
Cannabis reached the Americas, South America (mainly Chile) in 1545, and over 60 years later (1606), its cultivation was introduced to North America. Western medicine slowly progressed from the understanding and moderate use in the early and mid-19th century, to its wider use, based on its medicinal properties in the 20
th century. Nevertheless, due to prejudice and misinformation, the use of this plant has been marginalized, which has hindered research progress regarding its medicinal beneficial effects [
1,
2].
Currently,
Cannabis is the most commonly cultivated, trafficked, and abused drug worldwide, potentially causing a substantial public health impact since it can alter sensory perception and induce elation and euphoria [
4,
5]. Recent use rates among the population in general show a concentration to adolescents and young adults (20 to 24 years-old), ranging from 2%–5% of the global population (an estimated 13 million cannabis-dependent individuals in 2010); yet, the highest numbers (∼10%–13%) are reported in North America [
5,
6,
7]. A study published by Hasin and colleagues revealed a significant rise in marijuana use prevalence in 2001–2002 and 2012–2013, accompanied by a large increase of marijuana-induced disorders in this same time period [
8,
9]. Conversely, another study showed that
Cannabis-induced disorders declined among young users during 2013-2014, in the USA [
10,
11]. According to United States Code, “marijuana/cannabis” comprises “all parts” of the plant
Cannabis sativa L. and every compound derivative of such plant. By the year 2016, 28 states in the USA have voted to authorize or implement medicinal cannabis programs. Among these, eight states and the district of Columbia have legalized the recreational use of
Cannabis [
12]. In other countries, including the United Kingdom (UK), Denmark, Czech Republic, Austria, Sweden, Germany, and Spain, it is formally approved; thus, decriminalizing the therapeutic use of
Cannabis and cannabis-based products [
13,
14]. Pioneering in Latin America, Uruguay, became the first country to legalize the sale, cultivation, and distribution of
Cannabis [
15,
16]. Wilkinson and D’Souza have previously described that the medicalization and/or incorporation of
Cannabis into a medicine is complex for a number of reasons, including that (i) it is a plant rather than a pharmaceutical product, and (ii) knowledge of its properties and effects is still limited [
17]. However, in light of the recently and largely reported pharmacological discoveries and therapeutic benefits of
Cannabis, the controlled and medicinal use of
Cannabis for some pathological conditions have been enforced.
Era of cannabinoids started when Mechoulam and Gaoni isolated and characterized the main psychoactive component of
Cannabis sativa, the Δ9- tetrahydrocannabinol (Δ9-THC). Subsequently, in 1988, Howlett’s group established the presence of a specific cannabinoid receptor in the rat brain by using a tritium labeled cannabinoid [
18], followed by the cloning of the cannabinoid receptor type-1 (CB1R) [
19]. Then, Matsuda and coworkers (1990) described a second receptor, named the cannabinoid receptor type-2 (CB2R), which was cloned by Munro and coworkers in 1993 [
18,
19]. These receptors can be activated by endogenous molecules produced normally by our bodies, and likewise by external synthetic and natural molecules. The number of natural compounds identified or isolated from
Cannabis sativa has been increasing in the last decade, with 565 identified substances between cannabinoids and non-cannabinoid constituents [
20]. The genus
Cannabis comprises closely related species, mainly,
Cannabis indica,
Cannabis ruderalis (identified in 1924),
Cannabis sativa L., which is widely known as “hemp” and not psychoactive, as well as
Cannabis sativa, which induces psychoactive effects [
1]. Cannabinoids are defined as a group of molecules that modulate cannabinoid receptors (CBR) and are characterized by three varieties, such as endogenous or endocannabinoids, synthetic cannabinoids, and phytocannabinoids. The latter variety comprehends natural terpenoids or phenolic compounds derived from
Cannabis sativa or other species, and will be further explored later in this review [
21]. Altogether, 120 cannabinoids have been isolated from the
Cannabis sativa plant and classified into 11 general types, as described below (
Table 1) [
20].
Table 1. Cannabis sativa L. constituents by chemical class.
|
Chemical Class
|
Compounds
|
|
Δ9-THC types
|
23
|
|
Δ8-THC types
|
5
|
|
CBG types
|
16
|
|
CBC types
|
9
|
|
CBD types
|
7
|
|
CBND types
|
2
|
|
CBE types
|
5
|
|
CBL types
|
3
|
|
CBN types
|
11
|
|
CBT types
|
9
|
|
Miscellaneous types
|
30
|
|
Total cannabinoids
|
120
|
|
Total non-cannabinoids
|
445
|
|
Grand Total
|
565
|
THC, tetrahydrocannabinol; CBG, cannabigerol; CBC, cannabichromene; CBD, cannabidiol; CBND, cannabinodiol; CBE, cannabielsoin; CBL, cannabicyclol; CBN, cannabinol; CBT, cannabitriol, as previously described [20].
Pharmacologically approaching, three compounds have been isolated and identified as the most important, namely the Δ9-tetrahydrocannabinol (Δ9-THC), cannabidiol (CBD), and cannabinol (CBN). Relevantly, preclinical and clinical research has shown that cannabinoids, especially CBD, play key a role in different pathological conditions (Table 2).
Table 2. CBD pharmacological actions on pathological conditions.
|
Research Themes
|
Main Findings
|
References
|
|
Alzheimer’s disease (AD)
|
CBD prevented expression of proteins involved with tau phosphorylation and AD progression. CBD showed therapeutic potential for AD-associated cognitive impairment.
|
[22,23]
|
|
Anti-inflammatory properties
|
CBD induced apoptosis and inhibited lipopolysaccharide-activated NF-κB and interferon-β/STAT inflammatory pathways in microglial cells; CBD protected oligodendrocytes progenitor cells from inflammatory-induced apoptosis.
|
[24]
|
|
Anxiety
|
CBD modulated anxiety responses partially through 5-HT1A-mediated neurotransmission, and demonstrated anxiolytic effects during a stimulated public speaking test; CBD action on limbic and paralimbic regions contributed to reduced autonomic arousal and subjective anxiety; CBD blocked anxiety-induced REM sleep alteration through anxiolytic properties.
|
[25,26]
|
|
Diabetes
|
CBD showed beneficial effects on glycemic control and cardiovascular dysfunction during diabetes.
|
[27]
|
|
Immunomodulatory effects
|
CBD modulated T-cell function and apoptotic signaling pathway.
|
[28]
|
|
Inflammatory bowel disease (IBD)
|
CBD attenuated intestinal inflammation and normalized motility in patients with IBD.
|
[29]
|
|
Cognitive impairments
|
CBD interacted with components of emotional memory processing and memory-rescuing, as well as attenuated THC-induced memory impairment effects.
|
[30]
|
|
Neuropathic pain
|
CBD inhibited chemotherapy-induced neuropathic pain.
|
[31,32]
|
|
Parkinson’s disease (PD)
|
CBD administration showed neuroprotective effects during PD progression.
|
[33]
|
|
Schizophrenia
|
CBD showed antipsychotic-like properties in schizophrenia, as well as prevented clinical social dysfunction, and inhibited psychomotor agitation.
|
[34,35]
|
|
Seizure/Epilepsy
|
CBD showed anticonvulsant effects in animal models of seizure and patients with refractory epilepsy. CBD was also described as safe and beneficial for the treatment of epileptic disorders.
|
[36,37,38,39]
|
CBD, cannabidiol; NF-κB, nuclear factor kappa B; STAT, signal transducer and activator of transcription protein family; 5-HT1A, serotonin 1A receptor; REM, rapid eye movement sleep; THC, tetrahydrocannabinol.
When we talk about the era of the “endocannabinoid system”, we have to keep in mind that this biological system was named over the response of its receptors to cannabinoid drugs, such as the previously mentioned and well-studied Δ9-THC and biologically active synthetic analogs, just like it has happened with the opioids in the past. In addition to its receptors, the system is highly modulated by the enzymes involved in the endogenous cannabinoids synthesis and inactivation (endocannabinoid metabolism). Furthermore, some other receptors have been reported to be activated by cannabinoid drugs and related molecules, including GPR55, GPR18, and GPR119 [
40,
41,
42]. CB1R is a key component of the endocannabinoid system (ECS), since it interacts with endogenous and exogenous cannabinoids, including Δ9-THC, and it is considered the most abundant metabotropic receptor in the brain [
43]. It has been cloned from humans and it is accountable for the
Cannabis effects on mood, as well as negative psychotomimetic effects, including anxiety, paranoia, and dysphoria [
4,
44]. While CB1R plays a role as a neurotransmission regulator in different brain regions and for this reason mediates the
Cannabis psychoactive effects, CB2R, in particular, mediates anti-inflammatory and immunomodulatory actions [
45]. An accumulating body of evidence suggests that both CB1R and CB2R, and their ligands, play a significant role in physiologic and pathologic processes [
46]. In this context, both receptors have been widely studied regarding their relevance in the modulation of immune-mediated inflammatory diseases, neuroinflammation, neurological and neurodegenerative diseases, cancer, and autoimmunity.
Beyond the CBR, mammalian tissues can both synthesize and release cannabinoid receptor ligands [
44,
47,
48]. The era of ECS started when Devane and colleagues (1992) described for the first time, the N-arachidonoylethanolamine molecule, named anandamide from porcine brain. Interestingly, anandamide interact to CBR and induces behavioral actions similar to the ones induced by Δ9-THC, when administered in rodents [
4,
49]. The mainly endogenous cannabinoids are the anandamide (AEA) and the 2-arachidonoyl glycerol (2-AG). It is now ordinarily accepted that the mammalian tissues contain an ECS composed by: (i) CB1R and CB2R cannabinoid receptors [
19,
44], (ii) endogenous cannabinoids ligands [
49,
50,
51], and (iii) enzymes involved in the cannabinoids ligands synthesis and inactivation. Regarding these enzymes, the fatty acid amide hydrolase (FAAH) breaks amide bond and releases arachidonic acid and ethanolamine from AEA, and the monoacylglycerol lipase (MAGL) is responsible for a more efficiently 2-AG degradation [
52]. Endocannabinoids are produced on demand from membrane lipids using the machinery of the enzymes responsible for their synthesis, transport, and degradation. For instance, the N-arachidonoyl phosphatidylethanolamine (NArPE) originates a phosphatidic acid by a reaction mediated by a specific phospholipase D (NAPE-PLD); most importantly, it is hydrolyzed to AEA, in a reaction catalyzed by N-acyltransferase (NAT). The latter reaction happens out of an acyl group from the arachidonoylphosphatidylcholine (diArPC) sn-1 position converted to a phosphatidylethanolamine (PE) amino group. Following, AEA is degraded by FAAH. Synthesis of 2-AG depends on the phosphatidylinositol (PI) conversion to diacylglycerol (DAG) by the phospholipase C (PLC) enzyme, and subsequent DAG transformation to 2-AG by the action of the diacylglycerol lipase (DAGL) [
53]. The ECS is involved with multiple biological functions, such as immune-mediated inflammatory and autoimmune diseases [
53], as well as neuroinflammatory and neurodegenerative conditions [
54]. Moreover, the ECS participates in the immune control at the CNS [
55], maintaining overall “fine-tuning” of immune response balance [
56], and influencing the neuroendocrine reaction to inflammation and infection [
57].
Importantly, the ECS (i.e., CBR, endogenous cannabinoids, and anabolic/catabolic enzymes) are present in the cardiovascular tissues (myocardium, smooth muscle, and vascular endothelial cells), as well as in the circulating blood cells [
58]. CB1R are expressed in the peripheral nervous system, including vagal afferent neurons, while CB2R are expressed in cardiomyocytes, coronary artery endothelial cells, and smooth muscle cells. For this reason, the endocannabinoid signaling exerts complex cardiac and vascular effects ranging from vasodilatation to vasoconstriction, and decreased myocardial contractility [
58]. Those are important biological effects, as they could play an essential role in side effects promoted by potential molecules that are able to modulate this system. For instance, in healthy individuals, CB1R activation decreased myocardial contractility and blood pressure, possibly by peripheral inhibition of noradrenaline release from postganglionic sympathetic axons that leads to regulation of cardiac output [
59]. In an opposite way, CB2R may exert a cardioprotective role associated to its immunomodulatory properties during tissue inflammation and tissue injury in cardiovascular diseases. The endogenous cannabinoids (2-AG and AEA) also have vascular effects, which are mediated by perivascular transient receptor potential vanilloid 1 (TRPV1) and transient receptor potential vanilloid 4 (TRPV4) activation in smooth muscle cells, promoting dilatory response [
60]. Between the common clinical adverse effects associated with the
Cannabis plant use, the increased cardiovascular activity and heart rate, as well as decreased blood pressure have been described [
60]. In addition, the uses of
Cannabis plant or synthetic cannabinoids have been linked to myocardial infarction, cardiomyopathy, arrhythmias, and stroke [
58,
61,
62]. It occurs, possibly due to dose-dependent effects of phytocannabinoids and consequent modulation of the autonomic nervous system, at least partly via CB1R activation [
60], since the CB1R antagonist Rimonabant
® ameliorate the cannabis-induced tachycardia [
63,
64]. It is important to be aware of the harmful consequences that come along with the use of
Cannabis plant and/or synthetic cannabinoids, as they could contribute to development of cardiovascular disorders, since the ECS has an essential role in the cardiovascular signaling.
The future, shedding light to a new era, is promising and based on the cloning of CBR associated with the possibility of manipulation of endocannabinoid levels in tissues, by using endocannabinoid enzymes-targeted pharmacology. This represents an opening of a possible gateway to the discovery and/or development of cannabimimetic ligands, beyond the
Cannabis plant, which could still show therapeutic effects and possibly rule out many of the important adverse effects. A previous review has already stated that some plants, not belonging to the
Cannabis genus, produce molecules chemically similar to the phytocannabinoids, named cannabimimetic ligands [
65] (
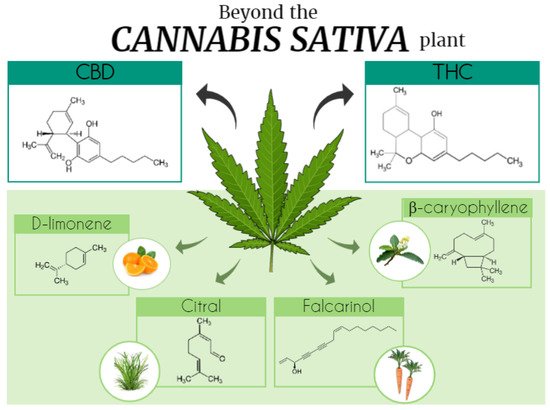
Figure 1). Cannabinoid-like molecules (mainly terpenes) of either plant or synthetic origin that are non-psychotropic have been studied. Terpenes and terpenoids are a widespread group of secondary metabolites found in numerous plant families, including Cannabaceae and others.
Figure 1. Beyond the Cannabis sativa plant. The Era of cannabinoids started with the description and isolation of the main Cannabis sativa psychoactive component, Δ9-tetrahydrocannabinol (THC). However, many other natural compounds were also identified, totalizing 565 substances among cannabinoids and non-cannabinoids constituents. This figure illustrates some of the Cannabis sativa compounds (d-limonene, β-caryophyllene, citral, and falcarinol) and its molecular structures that can be also found in other plants, such as Cordia verbenacea, lemon, Cymbopogon citratus, and carrot. CBD, cannabidiol. Figure created using the Mind the Graph platform.
2. Cannabis Phytocannabinoids: Focus on Tetrahydrocannabinol and Cannabidiol
The phytocannabinoid class includes more than a 100 compounds that are present in the
Cannabis sativa plant [
66], which interact with components of the human ECS, briefly addressed in this section. Phytocannabinoids production is dependent on plant internal factors (synthesized hormone levels, plant kind, and parts of the plant) and on external factors (humidity, light, type of soil, and temperature). The most elucidated compounds among the main phytocannabinoids are CBN, CBD, ∆8- e ∆9-THC, cannabigerol, and cannabivarin. The ∆9-THC is the major psychotropic compound found in high concentrations in the
Cannabis sativa plants. It is classified as a CB1R and CB2R partial agonist, showing preference for the CB1R. The agonist activity on CBR triggers adenylyl cyclase (AC) inhibition and, thereby, the ability of modulating different neurotransmitters release as dopamine, acetylcholine, glutamate, and gamma-aminobutyric acid (GABA) [
66]. Of note, phytocannabinoids not only bind to CBR, but also show potential actions on different kinds of receptors, such as peroxisome proliferator-activated receptors (PPAR), glycine receptors, and the transient receptor potential (TRP) cation channels. The CBD, unlike the tetrahydrocannabinol (THC), is a non-psychotropic cannabinoid that has been widely investigated regarding its potential therapeutic use. It has been already established in the literature that CBD shows anti-inflammatory, anti-epileptic, analgesic, anxiolytic, and neuroprotective properties, as well as it can be used to mitigate Parkinson’s disease (PD) symptoms [
67,
68,
69]—
Table 2. CBD acts as a negative allosteric modulator of CB1R [
65] and as an inverse agonist in CB2R, besides being a FAAH enzyme inhibitor.
To briefly highlight, many other phytocannabinoids (e.g., cannabigerol, cannabichromene, and cannabinol) showed significant therapeutic value. The cannabigerol (CBG) showed agonist and antagonist activity on TRP channels and it was also able to produce 5-HT
1 and CB1R antagonism [
70]. Additionally, CBG is an AEA reuptake inhibitor [
71], and it showed colon anti-tumor activity by inhibiting transient receptor potential melastatin 8 (TRPM8) channels [
72]. Relevantly, when associated with CBD, it demonstrated anti-inflammatory activity reducing tumor necrosis factor (TNF) expression and upregulating Interleukin–10 (IL-10) and Interleukin–37 (IL-37) levels [
70]. Cannabichromene (CBC) showed agonist activity on CB2R [
73]. Besides, it interacts with TRP channels, being suggested as a potential therapeutic resource for the treatment of pain and inflammation [
71]. Lastly, CBN showed similar therapeutic properties to other phytocannabinoids, such as anticonvulsant, anti-inflammatory, and antibacterial [
71]. In addition, CBN showed inhibitory activity on cyclooxygenase (COX), lipoxygenase (LOX), and P450 cytochrome enzymes [
71], as well as on keratinocyte proliferation, supporting a possible potential therapeutic for psoriasis cases [
74]. As it can be appreciated with the major phytocannabinoids, the wide ranges of possible interactions of these molecules with multiple targets in our body, demonstrates the magnitude and the complexity of phytocannabinoids acting in living organisms.
We just established that phytocannabinoids demonstrate different pharmacological effects, and it can get even more intriguing and complex when we focus on previous data describing that the combined use of some phytocannabinoids can possibly increase the positive effects proportionate by them. For instance, the use of CBD associated with ∆9-THC promoted downregulation of the neuroinflammatory process in animal models of multiple sclerosis (MS) [
75], besides, reducing pain [
76] and muscle spasticity in MS patients [
75]. Importantly, CBD attenuated the psychotropic effects of THC when used in a combined form [
75]. This last piece of data supports the hypothesis that CBD binds to an allosteric site on CB1R that is functionally distinct from the active site for 2-AG and THC [
77]. In this same context, a recent study reported that a botanical drug preparation (BDP) was more potent than pure THC to produce antitumor responses in cell culture and animal models of breast cancer. While pure THC mainly activated CB2R and generated reactive oxygen species (ROS), the BDP modulated different targets and mechanisms of action [
78]. This combined effect, observed with the association of phytocannabinoids and other compounds present in the
Cannabis sativa plant, such as terpenoids, is known as the entourage effect [
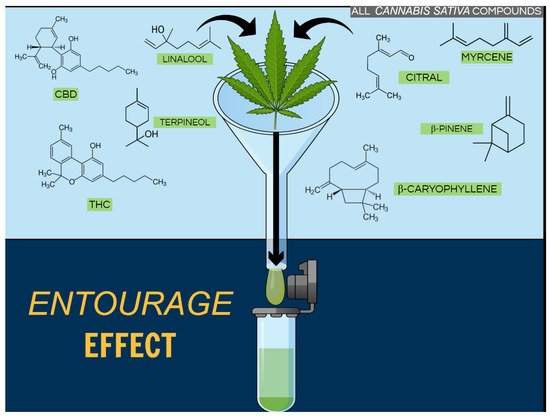
79] (
Figure 2).
Figure 2. Entourage effect. Beyond the Δ9- tetrahydrocannabinol (Δ9-THC) and cannabidiol (CBD), there are many compounds present in Cannabis sativa, including terpenoids (such as linalool, terpineol, and citral), which could contribute to beneficial effects related to this plant. However, the underlying mechanism of these medicinal effects is largely unknown when molecules are associated. Figure created using the Mind the Graph platform.
Cannabis Terpenoids
Beyond the phytocannabinoids, the
Cannabis plant is able to produce a diversity of compounds. Thirty-one-years ago, Mechoulam and Ben-Shabat described what they named the ‘’entourage effect’’, suggesting interactions between
Cannabis “inactive” metabolites and closely related molecules could markedly increase the activity of the “primary” cannabinoids (
Figure 2). From this, it was possible to hypothesize that could be a contribution of “minor cannabinoids” and
Cannabis terpenoids to the plant overall pharmacological effect. Therefore, a recent study evaluated the effect of common terpenoids, by themselves and in combination with THC, in AtT20 cells expressing CB1R or CB2R. Surprisingly, none of the analyzed terpenoids modulated the THC phytocannabinoid agonist signaling. Thus, the authors suggested that if the phytocannabinoids–terpenoids entourage effect exists, it is not at the CB1R or CB2R receptor level [
80]. Corroborating, when rats were submitted to an abdominal writhing model and treated only with terpenoids they demonstrated increased abdominal writhing, while the animals treated with THC showed robust analgesia, even better than the rats that received the
Cannabis full extract. In this case,
Cannabis antinociceptive property was linked to Δ9-THC, since terpenes alone do not alter the nociceptive behavior [
81]. Using a different approach, Nandal and co-authors exposed cancerous cell lines to treatment with phytocannabinoids combined with low concentrations of co-related terpenoids. They observed increased cell mortality at ratios similar to the ones obtained with the natural plant extracts [
82]. According to the authors, their results differed from Santiago et al. findings because they evaluated terpenoids without statistical correlation to THC, meaning that terpenoids concentrations in their preparations where higher than the natural-occurred in the plants [
80,
82]. Thus, the possible “entourage effect” and the positive contribution derived from the addition of terpenoids to cannabinoids could be interpreted as uncertain. However, the study of terpenoids represents an open window that goes beyond its actions
(i) in the endocannabinoid system solely, or
(ii) as mere phytocannabinoids passive co-authors, and even beyond the
Cannabis plant.