Oral mucositis (OM) is a pathological condition with several oral manifestations, originate from cytotoxic effects of non-surgical cancer therapies. The clinical manifestation ranges from diffuse erythematous areas to necrotic ulcers lesions in the mucosa. The oral mucosa presents confluent, deep, and devastatingly painful ulcerations in the most advanced clinical form.[1] Almost all oral or oropharyngeal mucosa areas undergoing radiation will develop this side effect, however, the patients undergoing chemotherapy regiment develop the condition depending on the dose and cytotoxicity of the drug used. Usually, incidence goes around 20 to 40% for solid tumors, while in the therapies with a high dose of cytotoxic drugs, like hematopoietic stem cell transplant, the incidence is around 80%.[2] The patients that develop OM during the cancer treatment can manifest alterations in physical, mental, emotional, and social health factors, proving an unhealthy state. Patients present diet modifications and weight loss, necessitate opioid analgesics, require supplemental nutrition, increase the risk of bacteremia and sepsis, disrupt optimal cancer therapy, and increase healthcare costs. [3]
It is common the association of head and neck cancer and OM in medical care however, the frequency in other cancers has long been overlooked and underreported. For this reason, a multidisciplinary team composed of other health professionals, as dentists, can identify and treat pathologies in advance during oncological treatment.
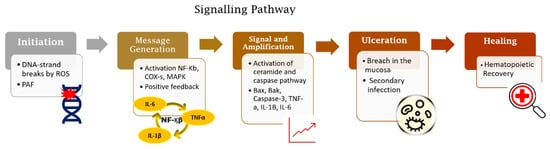
The OM development is described in a five-step pathogenesis model with several biological factors’ combinations. The lesion occurs with the damage of basal epithelial cells due to the radio-chemotherapy. The cascade of events starts with severe alterations in the environment that involves the generation of reactive oxygen species (ROS), activation of transcription factors (NF-kB) and inflammatory pathways (COX), and up-regulation of proinflammatory cytokines (TNF-a, IL1b, and IL-6).[2]
The clinical diagnosis can be made in the early stages. The mucosa presents erythema, the patients complain of burning and intolerance of some specific foods. After two weeks, the ulcerated lesions can be detected in one or more areas of the oral cavity. The patient refers to slight discomfort and inconvenience to severe pain, dysphagia, and difficulty in eating that lead to the opioid intervention. As a result of the cancer treatment, it is common to occur salivary alterations in composition and quantity, leading to the exasperation of OM development and impairment in the patient’s quality of life. The lesions recover depending on the patient's immune compromise, however, heal spontaneously for at least 2 weeks following the completion of the therapeutic regimen.[4] Medical and scientific community discourse about effective management of OM in cancer patients due to its high incidence and clinical significance in patient prognosis. Several scientific studies are carried out to discover a well-defined strategy that provides improved management of OM that may allow more aggressive therapeutic doses and more effective cancer treatment, improved patient survival, and wellbeing.[5]
All guidelines for the management of OM agree OM management can be divided into three basic components: general oral care, prevention, and palliative cares. The oral care purpose is to reduce some host-related risk factors for stomatitis, including lowering the impact of oral microbial flora. Therefore, a simple care protocol must be suggested, as brushing teeth, daily flossing, and mouth rinsing. In addition, spicy food, alcoholic beverages, and alcohol-based mouthwashes must be avoided.[6]
Prevention is the second most important factor in addressing oral mucositis. The combination of agents and physical strategies can provide anti-inflammatory, analgesic, and anti-microbial more effective effects in OM management. The preventive use of oral cryotherapy and photobiomodulation (PBM) therapy showed a reduction in the impact of the treatment toxicity in the oral mucosa.[7] The OM treatment effectivity increase can be noted with the use of several pharmacological agents (pentoxifylline, benzydamine hydrochloride, thalidomide, and simvastatin) and natural products such as Omega-3 FFA, essential oils from manuka (Leptospermum scoparium), vitamins, glutamine, chamomile, aloe vera, and curcumin.[8] The OM palliative care has focused on symptom control using topical or systemic analgesics and the application of barrier agents to cover injured mucosa.[3]
In conclusion, OM is a painful and wasting consequence of anticancer chemotherapy and/or radiotherapy. The occurrence of this pathology increases the risk of treatment interruption and a decrease in quality of life. A multidisciplinary team can provide global attention during the treatment, detecting early necessary interventions to manage the side effects of the cytotoxic therapeutic and providing wellbeing for cancer patients.
Reference:
1. Sonis, S. Oral Mucositis. Volume1. Springer Healthcare 2012 ISBN 10.1007/978-1-907673-46-7.
2. Sollecito,PT. Clinical Approaches to Oral Mucosal Disorders: Part II, An Issue of Dental Clinics of North America, Volume 58, Issue 2 of The Clinics: Dentistry, Elsevier Health Sciences, 2014, ISBN 0323289967, 9780323289962).
3. Sonis, S.T. Treatment for Oral Mucositis—Current Options and an Update of Small Molecules Under Development. Current Treatment Options in Oncology. 2021 22.. doi:10.1007/s11864-021-00823-6).
4. (Scully, C., Sonis, S., Diz, P., 2006. Oral mucositis. Oral Diseases 12, 229–241. doi:10.1111/j.1601-0825.2006.01258.x).
5. Campos MI, Campos CN, Aarestrup FM, Aarestrup BJ. Oral mucositis in cancer treatment: Natural history, prevention and treatment. Mol Clin Oncol. 2014;2(3):337-340. doi:10.3892/mco.2014.2536.
6. Lionel D, Christophe L, Marc A, Jean-Luc C. Oral mucositis induced by anticancer treatments: physiopathology and treatments. Ther Clin Risk Manag. 2006;2(2):159-168. doi:10.2147/tcrm.2006.2.2.159
7. de Carvalho, P.A.G.; Lessa, R.C.; Carraro, D.M.; Assis Pellizzon, A.C.; Jaguar, G.C.; Alves, F.A. Three photobiomodulation protocols in the prevention/treatment of radiotherapy-induced oral mucositis. Photodiagnosis Photodyn Ther. 2020 Sep; 31:101906. doi: 10.1016/j.pdpdt.2020.101906.
8. Lessa, R.C.; Alves, F.A.; Fortunati E.; Lu J. Oral Mucositis in Cancer and Potential Use of Omega-3 Free Fatty Acids in Its Management: A Review Biomedicines 2021 doi: 10.3390/biomedicines9111531.
1. Introduction
Oral mucositis (OM) is a severe form of acute inflammation and ulceration in the oral mucosa that can be induced by oncological therapy. OM induces erythema and swelling in the oral mucosa, followed by generalised ulceration and bleeding that can spread further from the oral cavity to the digestive tract and that is capable of causing debilitating effects for patients with OM. Effects include pain, inflammation, compromised oral hygiene, an increased risk for local and systemic infections as well as impaired nutrition [
1,
2,
3,
4]. The OM doubles the risk of systemic infections and quadruples the risk of death in cancer patients. Supportive care approaches to managing symptoms are commonly used in the OM condition. However, due the complicated pathobiology, those interventions are often not efficient and effective for all patients. Therefore, OM relief still represents an unmet need.
2. Biomolecular Mechanisms of OM
Radiation-induced and chemotherapy-induced OM have similar developmental mechanisms [
1]. The cascade of biological events responsible for the genesis of OM begins with the induction of DNA damage caused by radiation or chemotherapeutic cancer therapy [
6,
13] (
Figure 1).
Figure 1. Five-phase pathobiological model of oral mucositis. Based on this model, the process trigger is DNA damage induced by radio-chemotherapy followed by activation of inflammatory pathways together with apoptosis. These processes lead to the loss of integrity of the mucosal barrier and subsequent wound formation. The end of the signalling pathway occurs spontaneously after cessation of tissue damage.
The genesis of OM in neoplastic treatments occurs with or without mucosal cell DNA damage. Radiation-induced OM takes place when DNA degrades in oral basal-epithelial cells, while chemotherapy-induced OM occurs when basal cells become damaged by chemotherapeutic agents present in the systemic circulation [
14]. In radiation-induced OM, reactive oxygen species (ROS) are produced in response to DNA damage. The production of ROS negatively impacts the epithelium by causing irreversible DNA damage, promoting cell apoptosis. It is important to note that, at this stage, patients do not present any clinical symptoms, but the biological disruptions will have already occurred in the submucosa, advancing the progression of OM [
13,
14,
15]. With submucosal injury, initiators of inflammation are triggered (
Figure 2). Taken together, these endogenous mechanisms trigger a cascade of biological events and inflammatory pathways that initiate tissue damage in the oral mucosa [
5,
13,
16,
17,
18].
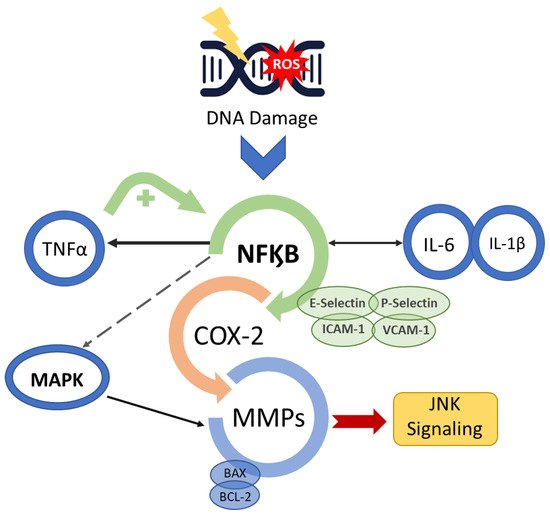
Figure 2. Mucositis signal amplification. Anti-cancer treatment activates the transcription factor nuclear factor-κB (NF-κB) after damage to basal epithelial cells and cells in the underlying tissue. The break in double-stranded DNA, the generation of ROS and PAF release through platelet aggregation leads to cell death and/or injury. NF-κB up-regulation initiates a positive feedback loop and consequently amplifies the production of pro-inflammatory cytokines (TNF-α, interleukin (IL)-6 and IL-1β) as well as the transcription of genes encoding MAPK, COX-2 and tyrosine-kinase signalling molecules, prompting activation of apoptotic genes (BAX and BCL-2) and matrix metalloproteinases.
Additionally, enzymatic and fibroblast activation occurs, further accelerating cell apoptosis in the oral submucosa, advancing OM [
19]. The activation of the pro-inflammatory NF-kB pathway also induces the expression of various adhesive molecules, including E-selectin, P-selectin, ICAM-1, vascular adhesion molecule 1 (VCAM-1) and angiogenesis molecules [
18,
20,
21]. Consequently, c-Jun N-terminal kinase (JNK) signalling is triggered, initiating a fibronectin breakdown and leading to macrophage activation [
14,
15,
22,
23]. NF-kB also affects genes in the B-cell lymphoma 2 (BCL2) family, which may directly induce cell apoptosis [
24].
There is a change in the interface integrity between the epithelium and the submucosa in the basement membrane, which is mediated by the transcription factor that activates protein 1 (AP1), which controls the genes that regulate matrix metalloproteinases (MMP) production [
13,
14,
22,
23,
24]. The modification in the production of MMP causes destruction of the subepithelial matrix and, consequently, may enhance the effectiveness of other signals, such as those carried out by TNF-α [
13].
Tissue-destructive processes result in visible inflammation and ulceration in the oral mucosa, often leading to bacterial colonisation and further aggravating tissue damage. Alterations in the oral microbial communities occur during cancer treatments, leading to microbiota imbalances and consequently to an increase in normally contained populations of microorganisms [
25]. The presence of pro-inflammatory microbiota influences the severity of OM. For example, the increased amount of
Porphyromonas gingivalis and the oral yeasts
Candida glabrata and
Candida kefyr alter the recovery capacity of epithelial cells of oral mucosa, leading to a delay in the wound healing capacity [
26]. Ruptures in the oral mucosal tissue thereafter led to microbial colonisation and growth, creating a risk of infection for patients. The open wounds in the oral cavity caused by OM allow opportunistic bacteria, such as
Actinomyces, Lactobacillus, Bifidobacterium and
Eubacterium, to colonise the tissue and release toxins into the submucosa, causing damage and leading to infection. This also increases the risk of septicaemia in patients with neutropenia [
27,
28,
29].
The inflammatory process culminates with wound healing associated with hematopoietic recovery, the re-establishment of balanced local microbial flora and an absence of factors that interfere with wound healing, such as infection resolution and diminished mechanical irritation [
16,
30,
31]. The resulting repair of the extracellular matrix leads to mucosal renewal and healing via stimulated proliferation, migration, adhesion and differentiation of compromised tissues in the submucosa [
15,
32]. Nevertheless, residual angiogenesis in the tissue after an OM episode induces higher risk of future episodes [
33].
The course of OM progression is not only associated with treatment factors but also with patients’ characteristics such as body mass profiles, renal and hepatic function, local oral factors and genetics [
5,
31,
34]. Despite OM being an independent risk factor for the development of infections, several researchers have demonstrated that microbial flora is not a primary causative factor for the developmental pathology [
23]. Once the individual risks for mucositis have been identified, efforts to interfere in the inflammatory responses from different treatment approaches will naturally follow. Therefore, the therapy-based strategy involves the concomitant use of agents that are able to act in different phases of the pathogenesis of mucositis [
34].
3. Prevention and Management Strategies
OM treatment is a miscellany of therapies that quest the control of the diseases and the symptoms relieved. Therefore, the clinical practice guidelines from the Multinational Association of Supportive Care in Cancer and International Society of Oral Oncology (MASCC/ISOO) summarized the standard protocol to manage the OM in cancer patients [
32,
34]. The proposed intervention strategy is to begin with the care in oral health with a combination of toothbrushing and flossing [
35]. The strategy is followed by the elimination of any type of irritant and the control of the proliferation of oral pathogenic microflora through mechanical removal, combined with the individual use of mouth rinses to maintain oral hygiene. Complete oral examinations and dental interventions are critical components performed in conjunction with oncological treatments [
32,
34,
35].
Oral cryotherapy and photobiomodulation (PBM) therapy have been utilised preventively to reduce the impact of the treatment toxicity in the oral mucosa [
36]. The PBM is recommended for the prevention and treatment of OM in patients receiving cancer treatments. Several studies have demonstrated the effectiveness of anti-inflammatory effects in supporting tissue repair [
13,
33,
37,
38,
39,
40,
41,
42,
43,
44,
45]. Nevertheless, clinical evidence still shows that some patients present recurring episodes of OM during their cancer therapy despite being treated with LLLT [
37].
Pharmacological agents (pentoxifylline, benzydamine hydrochloride, thalidomide and simvastatin) currently utilized to prevent and treat OM have variable efficacy rates and significant side effects, rendering this treatment strategy less than ideal [
13,
14,
15]. The requirement to reduce the side effects of pharmacological agents and increase the possibility of a patient’s fast recovery elicited the need for research to demonstrate the benefits of utilising natural resources and herbal medicines to manage the OM wound and related inflammatory conditions [
3,
33]. For this reason, several natural products such as chamomile, essentials oils from manuka (
Leptospermum scoparium) and kanuka (
Kunzea ericoides), vitamins A, B12 and E, folate, glutamine, aloe vera and curcumin have been studied [
46,
47,
48,
49]. In addition, several studies have investigated the mechanisms of action of n-3 fatty acids (or omega-3 fatty acids) against several diseases, with observed successes that are likely due to the fatty acids’ anti-inflammatory effects [
50].
Researchers have demonstrated that the use of a combination of agents and physical strategies can provide anti-inflammatory, analgesic and anti-microbial effects that can be used to manage cancer-therapy-induced OM in general. The combination strategy has been promising for patients’ symptom relief and wellness during the OM course [
13,
37].
This entry is adapted from the peer-reviewed paper 10.3390/biomedicines9111531