- vitamin D
- 1
- 25-dihydroxyvitamin D
- rheumatic diseases
- rheumatology
- rheumatoid arthritis
- systemic lupus erythematosus
- spondyloarthropathies
- osteoarthritis
- hyperuricemia
- gout
1. Introduction
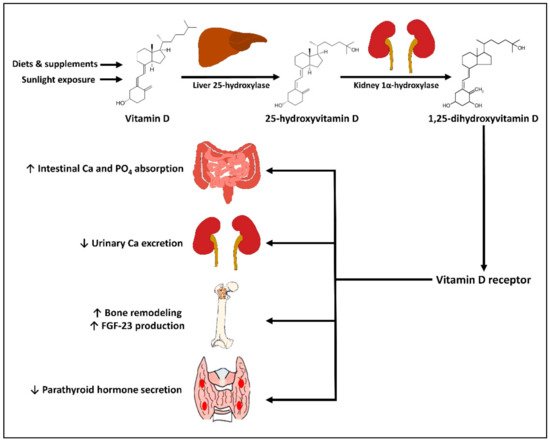
2. Physiology of Vitamin D
3. Vitamin D in Prevention and Treatment of Rheumatic Diseases
3.1. Rheumatoid Arthritis
Vitamin D is believed to play a role in modulating the pathogenesis and disease activity of RA, based on the actions of 1,25(OH)2D on the adaptive immune response that suppresses the proliferation and activity of TH1 and TH17 and enhances the Treg activity [63]. Furthermore, genomic studies have shown that certain polymorphisms of the gene encoding VDR and DBP are associated with susceptibility to RA, suggesting that the vitamin D signaling pathway may be involved in the pathogenesis of RA [64,65].
Multiple observational studies have shown the association of vitamin D status or intake with incidence and severity of RA [66]. For example, in a prospective cohort study by Merlino et al., women in the highest tertile of vitamin D intake had a lower risk for RA by 33% compared with those in the lowest tertile [67]. Moreover, a higher amount of ultraviolet B exposure was shown to be associated with a decreased risk of incident RA in the Nurse Health Study cohort of 106,368 women aged 30–55 years old [68]. This finding is in line with the evidence that the risks of some immune-mediated diseases (e.g., type 1 diabetes, multiple sclerosis, and RA) are higher in high-latitude regions where there is a relatively low amount of ultraviolet radiation and a high prevalence of vitamin D deficiency [69,70]. These observations, therefore, support that vitamin D obtained from either oral intake or sunlight exposure could possibly be protective against RA. In the COMOrbidities in Rheumatoid Arthritis (COMORA) study consisting of 1413 patients with RA from 15 countries, the serum level of 25(OH)D was inversely correlated with disease activity, as assessed by the Disease Activity Score-28 (DAS28) after adjusting for potential confounders [71].
3.2. Systemic Lupus Erythematosus
3.3. Spondyloarthropathies
3.4. Gout and Hyperuricemia
3.5. Osteoarthritis
3.6. Other Rheumatic Diseases
This entry is adapted from the peer-reviewed paper 10.3390/ijms221910659