Ramadan is one of the five pillars of Islam, during which fasting is obligatory for all healthy individuals. Although pregnant women are exempt from this Islamic law, the majority nevertheless choose to fast. The association between Ramadan fasting and health outcomes of offspring is not supported by strong evidence. To further elucidate the effects of Ramadan fasting, larger prospective and retrospective studies with novel designs are needed.
- fasting
- Islam
- pregnancy
- humans
- fetal development
- pregnancy outcome
- infant
- newborn
1. Introduction
2. Ramadan Fasting during Pregnancy and Health Outcomes in Offspring
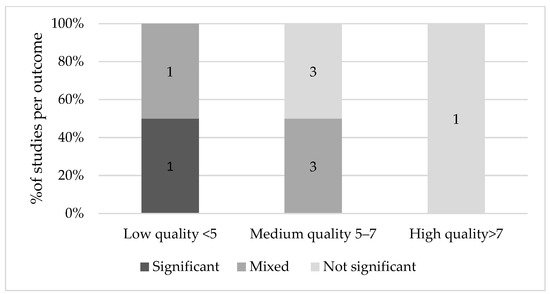
2.1. Fetal Growth Indices
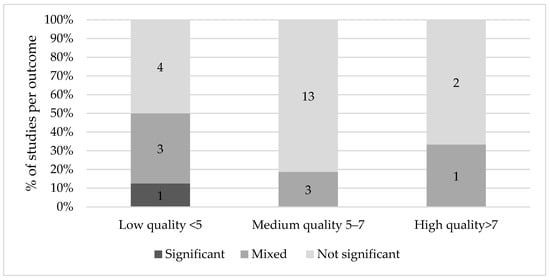
2.2. Birth Indices
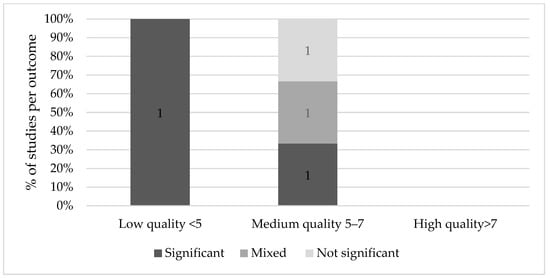
2.3. Cognitive Effects
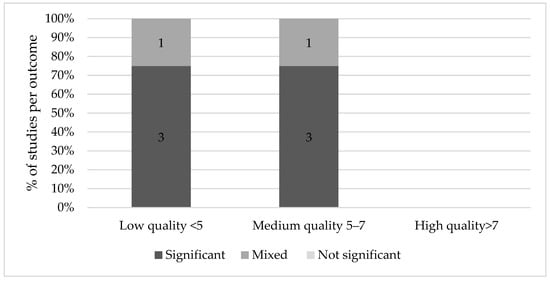
2.4. Long-Term Effects
an Ewijk [57] found that Muslims prenatally exposed to Ramadan fasting had poorer general health (6.1% of a standard deviation, p < 0.01), rated by professional health workers who measured a number of health and physical indicators such as height, weight, blood pressure, hemoglobin levels and lung capacity on a 9-point scale. This effect was more pronounced in those older than 45 years (18.5%, p < 0.01) and it appeared stronger when Ramadan started in the second trimester. Alwasel et al. [51] similarly found that boys and girls of mothers exposed to Ramadan had a significantly different length and length of gestation than their counterparts in the second trimester only (p = 0.005 and p = 0.04 respectively). Based on the same Indonesian Family Life Survey, Van Ewijk and colleagues found that on average, adult Muslims who were exposed to Ramadan in mid- and late-gestation had a lower BMI because of lower weight (respectively −0.93 kg, CI 95% −1.72, −0.14 and −1.06 kg, CI 95%–1.88, −0.25) compared to those not in utero during Ramadan [58]. Furthermore, those conceived during Ramadan, in addition to thinner stature, had a smaller stature, being on average 0.80 cm shorter than those who were not exposed. Although Kunto and Mandemakers [54] discovered a similar effect of prenatal exposure to Ramadan on BMI and stature, their results were not significant. For an overview of the evidence of long-term effects of Ramadan fasting on the offspring, see Figure 5.
3. Summary
Some studies found an association between Ramadan fasting and fetal growth indices, birth indices, cognitive scores and long-term consequences. However, significant results were predominantly found in low quality studies. None of the high-quality studies reported a significant effect on fetal growth, birth, cognitive or long-term outcomes. Medium quality studies generally found mixed or non-significant results, although the majority of medium quality studies found significant results for long-term effects.
Ramadan fasting did not seem to affect the health of healthy, pregnant women nor their offspring [2,11,12]. Rouhani and Azadbakht [11] did not find significant effects, however, the researchers advised to avoid Ramadan fasting due to the limitations of the studies that were included in the review. Glazier and colleagues [13] concluded that more studies are needed to accurately determine the association with maternal and neonatal outcomes. In their systematic review and meta-analysis, they found that birth weight is not adversely affected by Ramadan fasting, but there was insufficient evidence for potential effects on other perinatal outcomes. In line with Nikoo et al. [59], no reported effect of Ramadan fasting on fetal physical and mental growth was identified. However, although most studies found no association between Ramadan fasting and fetal measures, three studies found a decreased AFI [20,24,25]. Since other fetal parameters were normal, an explanation for this decrease could be maternal dehydration as a result of high temperatures and long durations of fasting. Low amniotic fluid levels have been linked to perinatal death, fetal deformations, PTD, LBW and poor neonatal health [60,61]. For this reason, it is advisable to monitor the pregnancies of these women more closely.
Future research should investigate the effect of Ramadan fasting on cognition and long-term effects, ideally with a prospective study design that involves many participants. These prospective studies should be carefully designed, as the sociological and religious dimension of Ramadan may also alter maternal behavior to protect the belief that Ramadan has no effect on their offspring. Another promising approach to studying these effects would be enhanced retrospective study designs based on routine data collection comparing Islamic pregnant women during and outside the Ramadan period to reduce the effect of confounding but only under the condition that (Ramadan) fasting is registered in routine care, as other seasonal effects on birth outcomes may still apply such as malaria [73,74] and vitamin D status [75,76]. These types of studies are also needed in order to confirm the results of high quality studies in birth and fetal health outcomes. In addition to the frequency of eating during Ramadan, the quality of the food that women eat during the nighttime also deserves attention. In addition to these quantitative studies into the effects of Ramadan fasting, we argue for qualitative research into the communication between pregnant women and their healthcare providers in order to improve the shared decision-making processes concerning fasting during pregnancy.
This entry is adapted from the peer-reviewed paper 10.3390/nu13103450