Acute lower extremity proximal deep venous thrombosis (DVT) requires accurate diagnosis and treatment in order to prevent embolization and other complications. Point-of-care ultrasound (POCUS), a clinician performed, and clinician interpreted bedside ultrasound examination has been increasingly used for DVT evaluation mainly in the urgent and critical care setting, but also in the ambulatory clinics and the medical wards.
1. Introduction
Acute lower extremity proximal deep venous thrombosis (DVT) is a serious vascular condition with an annual incidence of 0.1% in adults [
1]. Accurate diagnosis and treatment of acute DVT is crucial in order to prevent embolization and other complications. Mortality from pulmonary embolization, a potentially fatal complication of DVT, could be up to 30% if left untreated [
2]. Although the gold standard for the diagnosis of DVT is contrast venography, duplex ultrasonography performed by radiology or vascular laboratories has become the standard of care due to its widespread availability, cost-effectiveness, lack of radiation, lack of intravenous contrast, and patient comfort [
3]. Point-of-care ultrasound (POCUS), a clinician-performed and clinician-interpreted bedside ultrasound examination, has been increasingly used in the emergency department (ED), the intensive care unit (ICU), medical wards and in the outpatient setting for evaluation of the proximal lower extremity venous system [
4,
5,
6,
7]. Studies have found that POCUS may have comparable diagnostic accuracy to radiology or vascular lab-performed duplex ultrasonography for the detection of proximal lower extremity DVT, which makes it a very useful tool in routine clinical practice [
4,
5]. The American College of Emergency Physicians has supported the use of POCUS by trained physicians to evaluate for DVT since the 1990s [
8], but it was not until 2017 that DVT was added in the list of twelve core ultrasound applications for emergency medicine physicians [
9]. Interest in using POCUS for diagnosing DVT has grown substantially, not only in emergency medicine and critical care, but also in internal medicine and hospital medicine.
2. Equipment and Current Technology
Ultrasound machines used in existing literature can range from pocket-sized handheld devices to more sophisticated trolley or cart mounted machines with varying cost, ranging between 1500 and greater than 30,000 US dollars [
10,
11,
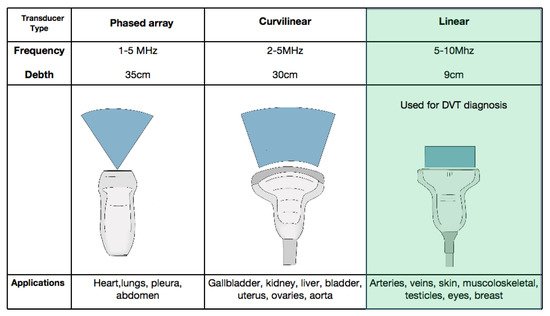
12]. The linear transducer is used in the venous mode with depth ranges between 1–4 cm and frequency set around 7.5 Mhz [
13,
14] (
Figure 1). Most handheld manufactures sell a probe that can be used for vascular applications and many of these devices include a probe with multiple applications.
Figure 1. The three types of transducers used in point-of-care ultrasound (POCUS). The linear transducer (light green) is preferred for the evaluation of veins. DVT = deep vein thrombosis.
3. Patient Preparation
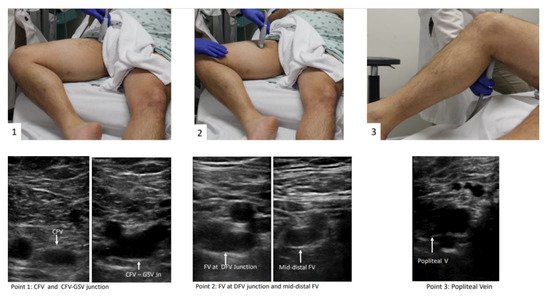
The patient should be positioned supine and the head should be elevated to 30° preferably, which can help blood pooling in the veins of the lower extremities and aid in visualization of the vasculature [15]. Then the examiner should externally rotate the patient’s hip and bend the knee slightly into what is known as the “frog leg” position [15]. This is the most popular position because it enlarges the femoral veins and brings it closer to the field of vision for the plane of the ultrasound probe. In addition, the “frog leg” position allows the examiner to scan the inguinal region and the popliteal fossa without having to reposition the patient [16]. When possible, prone position can help in examining the popliteal veins [17]. The examiner is typically most comfortable standing at the patient’s side, ipsilateral to the extremity being evaluated. When using a cart-based ultrasound machine, it should be positioned within the examiner’s reach at the head of the bed. The bed height should be elevated for examiner comfort [12]. The patient preparation and positioning are depicted in Figure 2.
Figure 2. 3-point POCUS technique for evaluation of acute proximal DVT in the right lower extremity. The “frog-leg” position is depicted. Veins were presented in all points before compression application. Abbreviations: Rt = right, CFV = common femoral vein, GSV = great saphenous vein, FV = femoral vein, DFV = deep femoral vein.
4. Protocols
There is variability in the definition of POCUS protocols to evaluate for DVT and their names, as well as the levels they include, can be a source of confusion for learners. The two main types of POCUS examinations that have been studied for the diagnosis of DVT are called “2-point” and “3-point” exams, which is somewhat of a misnomer because they both involve scanning more levels or segments of vein than that. Even within 3-point protocols, there is variability in the levels of proximal lower extremity vein included. The term “compression ultrasound” is used historically to refer to bedside ultrasound in B-mode without Doppler. This involves inspection for echogenic thrombus and if a thrombus is not seen, testing for compressibility of the visualized segment of vein with the probe in the transverse orientation [12]. For the purpose of this entry, the term POCUS is used and unless otherwise specified refers to B-mode inspection for thrombus and the compression ultrasound technique.
The “2-point” POCUS technique evaluates the common femoral vein (CFV) and the popliteal vein (PV) [
18,
19,
20,
21]. In the 2-point examination, the common femoral vein is assessed from the inguinal ligament until it becomes the femoral vein (FV) (historically named the superficial femoral vein). This includes the common femoral vein–greater saphenous vein (CFV-GSV) junction. The PV is assessed starting from where it is parallel to the popliteal artery and following it until the trifurcation [
14]. In the “3-point” technique, the CFV and PV are evaluated as in the 2-point examination, but further scanning of the FV in the proximal thigh is undertaken [
11,
22,
23]. The 3-point compression protocol begins at the level of CFV and includes the CFV-GSV junction, the proximal FV, mid-distal FV, and PV (
Figure 2). A graphic representation of the aforementioned vein levels typical for a 3-point POCUS examination is shown in
Figure 3. The use of color Doppler or spectral Doppler are advanced techniques when it comes to point of care setting but can be very useful in determining the degree of occlusion when a DVT is found [
11]. Determining the chronicity of a DVT is also typically reserved for vascular lab and diagnostic radiology, not POCUS evaluation.
Figure 3. Cross-sectional anatomy of lower extremity proximal vasculature. Compressions should be performed at each of the marked points (3-point technique).
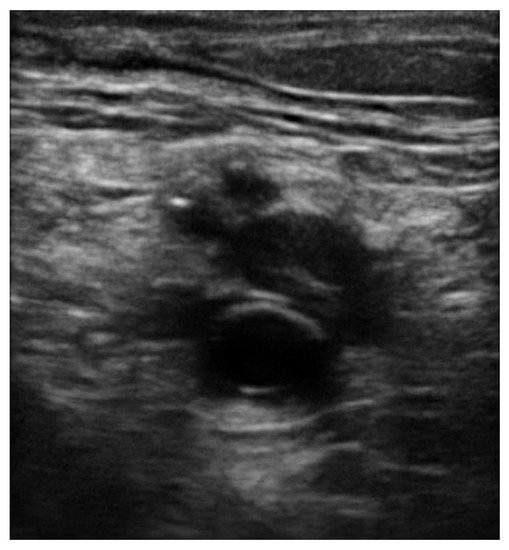
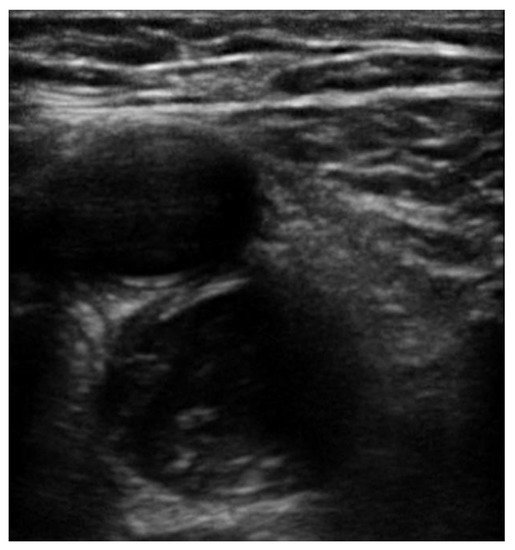
In all POCUS techniques, the diagnosis of DVT is made by visualizing echogenic thrombus (Figure 4 and Figure 5) or if an area of vein is not able to be fully compressed.
Figure 4. Echogenic thrombus is visible in the right popliteal vein (vein on the top of the artery).
Figure 5. Echogenic thrombus is visible in the left distal femoral vein (artery on the top of the vein).
5. Sensitivity and Specificity
Overall, the existing studies have shown that POCUS has excellent diagnostic accuracy for evaluation of acute proximal DVT. However, it should be emphasized that these studies have significant heterogeneity as far as the setting (ICU, ED, medical ward), as well as the preceding training of the clinicians performing POCUS (resident vs. attending). Therefore, extrapolating these findings to different users with varied training must be undertaken with caution.
6. Pre-Test Probability and D-Dimer
Crucial to the evaluation of suspected DVT is an accurate determination of pre-test probability for a clot. Widely accepted guidelines recommended the use of validated scores and high sensitivity D-dimer to evaluate the likelihood of a diagnosis of DVT in patients presenting with suggestive symptoms [
31].
Use of algorithms incorporating pre-test probability assessment with a sensitive D-dimer test have been shown to reduce the number of imaging studies performed [
32,
33]. A scoring system from Wells et al. is the most commonly used in clinical practice where a score ≥2 indicated a high pre-test probability of DVT [
33]. After an unlikely pretest probability of DVT, a negative D-dimer test is adequate to safely rule-out DVT and venous ultrasound may not be appropriate for those individuals [
33]. Ultrasound to diagnose DVT is appropriate for patients with a likely pretest probability or an unlikely pretest probability with a positive D-dimer test [
32,
33,
34]. It should be emphasized that the above recommendations were designed for radiology or vascular lab-performed ultrasonography but can provide a helpful tool in the hands of clinicians using POCUS regarding risk classification.
7. Time and Resources
The main advantage to POCUS in the evaluation for DVT is that it can be performed immediately at the beside by the clinician using a device already readily available in the ED, the ICU or on the medical ward. As far as turnaround time is concerned, a meta-analysis performed by Pomero et al. revealed that POCUS, as an alternative to radiology or vascular lab-performed venous ultrasound, may have an important role in current healthcare especially when these services are not available on a 24-h basis [
4]. In another study, POCUS appeared to have practical utility in the context of a busy emergency department setting since the average time from request to completion of study was within the first 15 min [
4].
8. Education
An important consideration when introducing POCUS in clinical practice is determining the necessary training and experience. The American College of Emergency Physicians guidelines suggest performance of the POCUS for clinical decision making after completion of a two-day course and 25–50 quality assurance reviewed studies [
9,
42,
43]. There is a lot of variability in educational material and curriculum used regarding education on POCUS techniques in general, but also when it comes to the diagnosis of DVT.
Overall, there is evidence supporting the assertion that clinicians or other skilled staff can perform POCUS to diagnose or rule out proximal DVT with high diagnostic accuracy after training [
46]. However, it is not clear how extensive the training should be and what it should entail. More studies are needed to further evaluate this domain.
10. Limitations
The pooled proportions of the false-negative rate of the 2-point and 3-point POCUS have been estimated around 4% and are similar between the 2 protocols [49,50]. A false negative evaluation for DVT would mean underdiagnosing thrombosis potentially leading to life-threatening pulmonary embolism. The pooled proportions of the false-negative rate of the 2-point POCUS and 3-point POCUS have been estimated around 4% and are similar between the two protocols [49,50]. Whether a full examination for distal DVT is appropriate or is still a debate, there are publications showing that 48% of patient with PE have contemporary isolated distal clots while this percentage for negative PE population is only 12% [51]. Unfortunately, these patients would be considered false negative while performing a standard POCUS protocol instead of a full CUS performed by a radiologist [52,53]. POCUS can also have false positives around 4% as reported by Fischer et al., which can lead to unnecessary anticoagulation treatment and risk of bleeding or other complications [11,54]. There are several potential causes of a false positive POCUS evaluation for DVT worth noting. Superficial thrombophlebitis can be mistaken for DVT, however the major difference is that superficial veins do not accompany arteries while deep veins do [55]. A Baker’s cyst appears as a circular anechoic structure in the popliteal fossa that can resemble a non-compressible vein (Supplemental Video S9) [56]. Enlarged inguinal lymph nodes can appear similar to a vein with a clot because of their oval structure, anechoic rim with hyperechoic center, but are easy to distinguish from a vein by scanning through to see that the structure is self-contained and even easier when the true CFV and arteries are found in a different fascial plane (Supplemental Video S10). Rarely, pseudoaneurysms and groin hematomas can be falsely diagnosed as DVT by non-experienced performers [56,57]. An important technical consideration for POCUS performers learning to evaluate for DVT is knowing how much to compress the vein. If the operator does not apply enough pressure or if the ultrasound probe is not perpendicular to the vein, this can lead to false positives [58]. Another cause of false-positive POCUS examination for DVT is the presence of “rouleaux formation” that is an accumulation of erythrocytes lying over the venous valves represented by spontaneously echogenic blood flow inside the vessel. While rouleaux is a common finding and usually does not have a clinical impact, it is important to highlight that this can also be frequently observed when there is a proximal venous obstruction, and thus a more proximal DVT must be ruled out. In contrast to a real condition of thrombosis, veins with rouleaux formation are compressible [59]. While POCUS can be immensely helpful in the rapid diagnosis of DVT at the bedside, equivocal findings should prompt further evaluation by radiology or a vascular lab-performed duplex ultrasound study.
This entry is adapted from the peer-reviewed paper 10.3390/jcm10173903