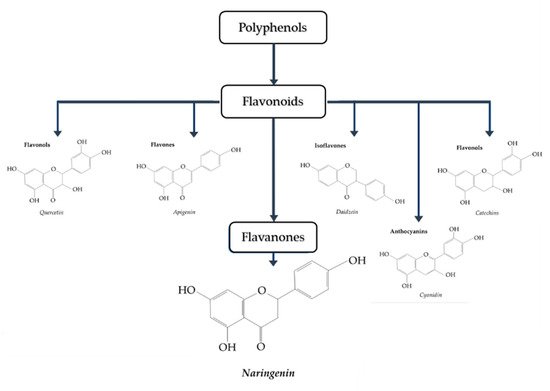
Type 2 diabetes mellitus (T2DM) is a metabolic disease characterized by insulin resistance and hyperglycemia and is associated with personal health and global economic burdens. Current strategies/approaches of insulin resistance and T2DM prevention and treatment are lacking in efficacy resulting in the need for new preventative and targeted therapies. In recent years, epidemiological studies have suggested that diets rich in vegetables and fruits are associated with health benefits including protection against insulin resistance and T2DM. Naringenin, a citrus flavanone, has been reported to have antioxidant, anti-inflammatory, hepatoprotective, nephroprotective, immunomodulatory and antidiabetic properties.
- insulin resistance
- diabetes
- naringenin
- naringin
- skeletal muscle
- adipose
- liver
- pancreas
1. Introduction
1.1. Glucose Homeostasis: Role of Insulin
1.2. Naringenin
2. Anti-Diabetic Effects of Naringenin
2.1. Effects of Naringenin: In Vitro Skeletal Muscle Cell Studies
| Cell | Naringenin Concentration/Duration | Effect | Reference |
|---|---|---|---|
| L6 muscle cells | 10–75 µM, 2 h | ↑ Glucose uptake ↑ Phospho-AMPK |
[46] |
| Primary porcine myotubes | Sambucus nigra flower (elderflower); Naringenin 0.1–10 µM, 1 h | ↑ Glucose uptake ↓ ROS levels |
[47] |
| L6 myotubes insulin resistance induced by palmitate (750 µM) | 50 and 75 µM, 16 h | ↑ Glucose uptake ↑ GLUT4 translocation ↑ Phospho-AMPK ↑ SIRT1 ↑ PGC-1α |
[48] |
2.2. Effects of Naringenin: In Vitro Adipocyte Studies
| Cell | Naringenin Concentration/Duration | Effect | Reference |
|---|---|---|---|
| 3T3-L1 preadipocytes | 5–100 µM, 48 h | ↓ Adipocyte proliferation ↑ LDH release |
[51] |
| 3T3-L1 adipocytes | 100 µM, 30 min | ↓ TNF-α FFA secretion ↓ IκB-α degradation ↓ Phospho-ERK protein expression ↑ Perilipin mRNA ↑ PDE3B mRNA |
[52] |
| 3T3-L1 adipocytes and mature human adipocytes | 20 µM, 2 min | ↓ Insulin-stimulated glucose uptake ↓ GLUT4 recruitment |
[53] |
| 3T3-L1 adipocytes | 10, 50 and 100 µM, 0.5–3 h | ↓ Inflammation ↓ TLR2 expression ↓ TNF-α ↓ MCP-1 |
[54] |
| 3T3-L1 differentiating and mature adipocytes | 0–50 µM, 0–120 h (Pre-adipocytes) and 0–24 h (Mature) | ↓ Adipogenesis ↓ Lipid accumulation ↓ aP2, PPARγ, STAT5A and adiponectin protein ↓ IRS-1 (Y896) ↓ Adiponectin |
[55] |
| Human white adipocytes | 8 µM, 7 to 14 days | ↑ GLUT4 mRNA ↑ Adiponectin mRNA ↑ UCP1, ATGL, CPT1β, PGC-1α and PGC-1β mRNA ↑ Oxygen consumption rate |
[56] |
2.3. Effects of Naringenin: In Vitro Hepatocyte Studies
| Cell | Naringenin Concentration/Duration | Effect | Reference |
|---|---|---|---|
| HepG2 human hepatoma cells | 10–200 µM, 24 h | ↓ Apo B secretion ↓ ACAT2 mRNA ↓ MTP protein and mRNA ↑ LDL receptor mRNA ↑ LDL uptake ↑ LDL degradation |
[58] |
| HepG2 human hepatoma cells | 200 µM, 6 h | ↓ Apolipoprotein B secretion ↑ SREBP-1 and LDLr expression ↑ PI3K activity |
[59] |
| HepG2 human hepatoma cells | 0–200 µM, 60 min | ↓ Apo B secretion ↑ ERK activity ↓ Microsomal triglyceride transfer protein |
[60] |
| Hepatoma (Fao) cells | 6–100 µM, 6 h | ↓ Glucose production ↓ Cellular ATP levels |
[61] |
| Huh7 hepatocytes and Lewis rat primary hepatocytes | 0–380 µM, 16–24 h | ↓ Triglyceride production ↑ Fatty acid oxidation ↓Trap220/Drip-2 and LBD ↓ LXRα response element ↑ mRNA of CYP4A11, ACOX, UCP1 and ApoAI |
[62] |
| Wistar rat hepatocytes | 300 µM, 30–50 min | ↓ Glucose production ↓ Gluconeogenesis ↓ Pyruvate transport |
[63] |
This entry is adapted from the peer-reviewed paper 10.3390/biom9030099