Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Development of innovative and time-efficient strategies to involve youth in physical activity is pivotal in the actual inactivity pandemic. Moreover, physical activity may improve academic performance, of great interest for educators. This entry aimed to analyze the effects of high-intensity interval training (HIIT) on cognitive performance and psychological outcomes in youth.
- exercise
- performance
1. Introduction
Consistent participation in physical activity is associated with a widespread range of physical health benefits for young people, including physiological and psychological benefits related to an active lifestyle [1,2]. Literature suggests that physical activity provides a positive effect on neurocognitive (i.e., attention, concentration) and behavioral (i.e., anxiety, psychological stress, depression) outcomes in youth [3,4]. Moreover, in recent years, a growing number of studies have also reported physical fitness as an influent intermediary of the effects of exercise training on cognition functions and academic performance, through direct and indirect psychological, physiological, and learning methods [5,6]. The conception that greater levels of physical fitness may improve attention, concentration, thinking and consequently academic performance, has a high level of interest for educators and physical educators [7].
Even with the extensive benefits of an active lifestyle, physical inactivity amoung young people is predominant [8,9], and tendencies report a secular weakness in adolescents’ physical fitness levels [10,11]. Assuming that several mechanisms of life change (i.e., increased physical activity, behavioral activation, autonomy, self-efficacy, self-esteem) are frequently supported by concepts associated with enthusiasm or motivation, the employment of existing research and theory may be helpful when drawing novel methodologies [12]. The previous evidence highlights the importance of developing innovative and time-efficient strategies to involve adolescents in physical activity, providing health benefits and effective solutions to this inactivity pandemic.
Accepted as a time-efficient method of achieving the health benefits of physical activity, high-intensity interval training (HIIT) has emerged as a useful and efficacious alternative to the traditional training methods [13,14]. HIIT is comprised of different interval protocols, but generally involves short intervals (≤45 s) of bouts of maximal sprints in high intensity (>85% maximal heart rate) combined with recovery breaks (<60 s) [15,16]. A great curiosity of HIIT is that it represents a method that requires no or minimal equipment, being completed in a short period of time. Moreover, it seems to provide similar physiological adaptations when compared to longer sessions of traditional training methods [15,16,17]. Furthermore, younger populations may consider short bouts of vigorous-intensity exercise more likely, desirable and simple to follow when compared to traditional moderate-intensity exercises [18]. Additionally, involving children and adolescents in activities that could be pleasurable may support the implementation of healthy habits (e.g., remaining physically active), and the development of self-reliant physical activity to be sustained into adulthood [19].
An emergent body of literature supports the feasibility and efficacy of HIIT on improving cognitive function and psychological variables (i.e., depression, emotional wellbeing, sleep quality) in the young population [20,21,22,23,24].
Cognitive performance could be described by several variables concerning executive functions such as concentration, selective attention or working memory [25]. Psychological outcomes are obtained by variables describing behavioral actions such as anxiety, depression, distress, well-being and self-efficacy [26,27]. Low level of cognitive performance during youth has been associated with psychological concerns such as unkind emotions. Those emotions could produce depressive feelings, unhappiness or harmful interpretations of the environment, and influence daily living activities [28,29]. On the other hand, a positive relationship between physical activity (e.g., moderate aerobic exercise or coordinative activities) and cognitive performance in youth has been found [25]. An earlier study inclusively showed a small-to-medium positive effect of physical activity on children’s cognitive outcomes and academic performance [30]. Furthermore, a previous narrative review developed by Logan, Harris, Duncan, and Schofield [31], summarized evidence of the efficacy of HIIT in adolescent health. The authors reported meaningful evidence supporting HIIT as a potentially efficacious exercise modality for use in amoung adolescents. Nonetheless, it also recognized a need to explicitly report between-group differences for HIIT intervention and the control groups or steady-state exercise, such as the magnitude of difference between HIIT and other exercise modalities being of great interest to public health. An earlier narrative review presented by Tomporowski, Davis, Miller, and Naglieri [32] included studies of the effects of physical exercise on cognition and academic performance in children. The latter authors reported that physical exercise could be a fundamental strategy to improve mental functioning characteristics, which are essential to cognitive development. Nonetheless, the outcomes of the studies revealed variability, and a weak selected outcome measure was exposed. This may be due to the researchers selecting populations that are not representative of the general population [32].
Due to the interest in the potential for physical exercise in its numerous practices to develop cognitive performance, it was considered that a systematic and rigorous approach to review the literature was necessary, enabling a robust summary of the knowledge on this important thematic.
2. Description of the Studies Reviewed
A detailed analysis of these studies was reported (Table 1). The age of participants in all articles was under 18 years old and included boys and girls. The sample came from four different countries: 2 studies in Australia [20,39], 3 studies in Spain [21,22,40], 1 study in Japan [23], and 2 studies in the United Kingdom [24,41]. These studies included sample sizes from 30 to 184 subjects, ranging in age between 8 and 16 years old. For the study design, all the studies included a randomized controlled trial design. From the 8 studies reviewed, 62.5% (n = 5) developed a chronic intervention (i.e., repeated sessions of HIIT throughout days, weeks, or months), and 37.5% (n = 3) applied an acute intervention (i.e., single sessions of HIIT). Regarding the modality of HIIT, 87.5% (n = 7) of the studies [20,21,22,23,24,40,41] applied a traditional HIIT, in terms of running, sprinting, jumping, whereas 12.5% (n = 1) of the studies [39] used a traditional HIIT and also a high-intensity functional circuit training. Concerning the variables studied, 50.0% (n = 4) of the studies focused on cognitive performance [21,22,23,40], 37.5% (n = 3) of the studies targeted the psychological outcomes [20,24,41] and 12.5% (n = 1) of the studies determined the cognitive performance and psychological outcomes [39].
Table 1. Characteristics of analyzed studies (N = 8).
| Authors | Sample/Group/Age (Years)/Country | Exercise Protocol | Cognitive, Psychological and Behavior Measures | Main Outcomes |
|---|---|---|---|---|
| [39] | N = 65 EG1 = 21, EG2 = 22; C = 22 Age = 14–16 years Australian and New Zealand |
Exercise Intervention EG1: WU + GMCardio + Stretch (work-to-rest 30 s:30 s) EG2: WU + CombCR + Stretch (work-to-rest 30 s:30 s) C: PE 3 sessions/week in 8 weeks |
EF TMT—TA and TB PWB The Flourishing Scale PD Kessler Psychological Distress ScalePSC Physical Self-Description Questionnaire |
EG1 EF (TMT B), d = 0.26, +11.45% EG2 EF (B-A), d = 0.28, + 17.73% | EF (TMT B), d = 0.39, +17.33% EG1 PWB, d = 0.19, +3.32% EG2 PWB, d = 0.21, +3.62% EG2 PSC, d = 0.50, +23.58% |
| [20] | N = 38 Age = 9–15 years Australia |
EG1: intermittent fast running for shorts periods + long active recovery periods (30 min, HIIT, ≥85 HRmax) 3 sessions/week in 12 weeks |
Psychological assessment Piers-Harris Children’s Self-Concept Scale |
EG1 PSYA total score, d = 0.28, +8.71% |
| [24] | N = 30 Age = 11–13 years UK |
EG1: 3′ WU at 20 W + 8 × 1-min work intervals at 85% peak power interspersed with 75 s active recovery at 20 W + 2′ Stretch at 20 W | Affective responses FS Perceived enjoyment During exercise EES; post-exercise PACES Perceived exertion Pictorial Children’s OMNI scale Behavioral activation and behavioral inhibition BIS and BAS |
BAS/BIS with enjoyment responses PACES high BAS d = 0.55, +2.67% PACES low BIS d = 0.22, +1.35% Self-efficacy with enjoyment responses PACES high efficacy d = 0.55, +2.70% PACES low efficacy d = 0.83, +4.11% |
| [41] | N = 54 Age = 12–15 years UK |
HIIT protocol: 3′ WU at 20 W + 8 × 1-min intervals at 90% peak power + 75 s recovery at 20 W + 2′ Stretch CMIE protocol: continuous moderate intensity cycling at 90% GAS) |
Exercise Enjoyment Modified PACES for adolescents (perceived enjoyment) |
HIIT protocol in PACES score (boys, d = 0.73, + 32.43%; girls, d = 0.39, + 11.58%) |
| [22] | N = 184 EG1 = 90, C = 94 Age = 12–15 years Spain |
2 sessions/week in 12-weeks intervention EG1: 4′WU + 16′ over 85% HRmax within PE classes (work-to-rest between 20 s:40 s to 40 s:20 s) C: static stretch within PE classes) |
Memory Ad hoc test of 1 min (RIAS test) Selective attention and concentration Brickenkamp’s d2 Test Linguistic reasoning Ad hoc test (reading speed and semantic comprehension) |
EG1 selective attention, d = 0.29, +10.68% EG1 concentration, d = 0.28, +8.00% EG1 linguistic reasoning, d = 0.25, +7.66% |
| [21] | N = 158 EG1 = 77, C = 81 Age = 12–16 years Spain |
Exercise Intervention EG1: 4′WU + 16′ combination cardiorespiratory and coordinative exercise (4 sets, 4 exercises, work-to-rest 30 s:30 s) C: static stretching |
Cognitive Performance Ad hoc test 1 min (memory test) Brickenkamp’s d2 test (selective attention and concentration capacity) Measurements on baseline, immediately post, and after 2, 3, 4, 24, 48 h) |
EG1 (after training) selective attention, d = 0.81, + 60.73% EG1 (after training, and 2 h after training) Concentration, d = 0.71, + 61.10%, and d = 0.72, + 62.49% |
| [23] | N = 56 EG1 = 27, C = 29 Age = 8–12 years Japan |
Exercise Intervention EG1: 10′WU + 8′aerobic and core exercise + 5′Stretch (work-to-rest 30 s:30 s) C: PE 3 sessions/week in 4 weeks |
Executive Function DFS/DBS test ToH |
EG1 DFS test total score d = 0.33, +10.56% EG1 DFS test MS d = 0.22, +6.36% EG1 DBS test total score d = 0.30, +14.14% EG1 DBS test MS d = 0.34, +13.37% EG1 ToH 3-disk d = 0.75, +78.56% C ToH 4-disk d = 0.84, +66.18% |
| [40] | N = 67 EG1 = 26, EG2 = 23, C = 18 Age = 12–14 years Spain |
EG1: PE, 4 sessions (55 min)/week for 16 weeks EG2: PE + high intensity training, 4 sessions (55 min)/week for 16 weeks C: PE, 2 sessions (55 min)/week for 16 weeks |
Cognitive Performance IGF-M (non-verbal and verbal abilities, abstract reasoning, spatial ability, verbal reasoning and numerical ability) |
Non-verbal abilities EG1, d = 0.39, +5.29% EG2, d = 0.88, +47.70% Verbal abilities EG2, d = 1.58, +22.61% Abstract Reasoning EG1, d = 0.34, +5.37 EG2, d = 0.75, +44.50% Spatial Ability EG2, d = 37.19, + 22.85% Verbal Reasoning EG2, d = 1.00, + 15.71% Numerical Ability EG2, d = 1.20, +8.28% |
3. Risk of Bias in the Included Articles
About 50.0% of the studies were randomized and 50.0% used a crossover design. Most investigations did not implement a blinding design, and most of the studies made a between-group comparison. In fact, the blinding item is identified as the lesser item applied, due to inherent difficulty for practical reasons [42]. Only 25.0% of the studies revealed their concealed allocation, which would conduct itself toward systematic bias of therapeutic effectiveness [42]. About 75.0% of the studies reported a low risk of bias in the incomplete outcome data (attrition bias domain), which revealed transparency in the methodology used, and that well reported losses and exclusions occurred in the studies [37] (Figure 2 and Figure 3).
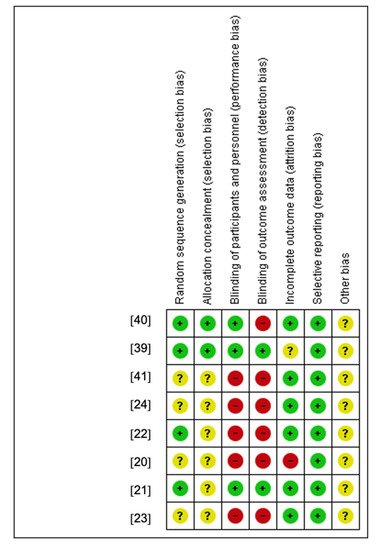
Figure 2. Judgments about each risk-of-bias item for each included study.
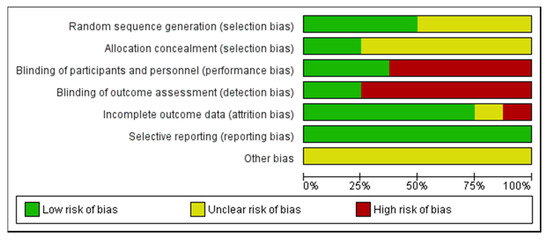
Figure 3. Risk-of-bias item presented as percentages across all included studies.
4. HIIT in Children and Adolescents Cognitive Performance
The cognitive performance of children and adolescents was observed in 4 studies [21,22,23,40], producing a total of 9 intervention effects (Table 1). One study found a positive effect of HIIT (4 weeks, 3 sessions/week, ≥85% HRmax, aerobic and core exercises) on executive function [23]. Another study [22] reported a positive small effect of HIIT (12 weeks, 2 sessions/week of HIIT, >85% HRmax, work-to-rest 20 s:40 s to 40 s:20 s) on linguistic reasoning, concentration, and selective attention. Mezcua-Hidalgo and colleagues [21] found positive effects through a large and medium effect size of HIIT (single session of HIIT, combination cardiorespiratory and coordinative exercises, work-to-rest 30 s:30 s) on selective attention and concentration, respectively. Finally, Ardoy et al. [40] showed significant effects on non-verbal, verbal and numerical abilities, as well as to abstract and verbal reasoning, and a medium effect size on spatial ability when physical education classes were combined with high intensity training (16 weeks, 4 sessions/week).
5. HIIT in Children and Adolescents Psychological Outcomes
The psychological outcomes on children and adolescents were studied in 3 studies [20,24,41], yielding a total of 2 intervention effects (Table 1). One of those 3 studies found a positive effect of HIIT interventions (12 weeks, 3 sessions/week, ≥85% HRmax) on self-concept [20]. Another study [41] reported remarkable results through a positive medium and small effect size of HIIT intervention (single session of HIIT ≥ 85% HRmax) in the psychological well-being of boys and girls, respectively. Malik and colleagues [24] observed positive effects of HIIT intervention (single session, at 85% peak power) on children’s psychological well-being.
6. HIIT in Cognitive Performance and Psychological Outcomes
Interestingly, children and adolescents’ cognitive performance and psychological outcomes were analyzed in one [39] of the 8 studies included in the present review, which obtained different intervention effects (executive function, psychological well-being, physical self-concept). In this sense, a positive small effect was observed through two HIIT interventions (8 weeks, 3 sessions/week, protocol a: gross motor cardiorespiratory exercises; protocol b: combination cardiorespiratory plus bodyweight resistance training exercises) in executive function. As for psychological well-being, a positive small effect from both HIIT protocols was also observed. In the physical self-concept, a positive medium effect was obtained from one of the HIIT protocols (i.e., combination cardiorespiratory and bodyweight resistance training exercises) (Table 1).
This entry is adapted from the peer-reviewed paper 10.3390/ijerph18105344
This entry is offline, you can click here to edit this entry!