The rapid advances in human-friendly and wearable photoplethysmography (PPG) sensors have facilitated the continuous and real-time monitoring of physiological conditions, enabling self-health care without being restricted by location.
- skin electronic
- optoelectronic device
- photodiodes
- phototransistors
1. Introduction
With an aging population, the demand for wearable electronic devices to monitor physiological conditions has increased exponentially in recent years [1,2,3,4]. The continuous and real-time measurement of physiological parameters using different sensing techniques plays an important role in diagnosing health conditions. For example, small wearable sensor systems have been developed for people who are at risk of heart attack, seizures, and stroke [5,6,7]. Wearable devices are also becoming widely used to gather information about an individual’s muscle activity, sleep quality, and other physiological activities in daily life [8,9].
Several options for wearable technology have emerged in the form of integrated clothing, accessories, and body attachments [10,11,12,13,14]. A classic example is a photoplethysmography (PPG) sensor which utilizes infrared light to noninvasively measure changes in pulsatile blood flows at the skin surface [15]. At present, the PPG can be applied to various aspects of cardiovascular monitoring, including the detection of arterial oxygen saturation (SpO2), heart rate, blood pressure, cardiac output, respiration, arterial aging, endothelial function, microvascular blood flow, and autonomic function [16,17,18,19,20,21,22,23,24].
By applying sensors and mobile computing devices directly onto the body surface, the PPG sensor could also be designed as a skin-on interface [25,26]. The skin-interfaced wearable devices have the advantage of allowing the continuous monitoring of various physiological data as comfortably as possible. Moreover, flexible and stretchable electronic devices can conformally be placed on the skin and detect various signals with extremely high sensitivity [27,28,29].
3. Photoplethysmography (PPG) Sensor and Its Application
3.1. Mechanism of PPG Sensor
A PPG sensor is an optically obtained plethysmogram to monitor blood volume changes in the microvascular system. Conventional PPG sensors comprise two main components: light-emitting diodes (LEDs) and photodetectors (PDs). In the device architecture, red and near-infrared light from LEDs has generally been used as the long wavelengths are suitable for measuring deep-tissue blood flow [43]. The PDs detect volumetric changes in blood from cardiac pressure by absorbing light illumination from LEDs through the skin. The noninvasive and optical measurement system enables a PPG to monitor breathing, hypovolemia, and other circulatory conditions [44].The PPG signal can be acquired in reflection or transmission mode [45]. In transmission mode, the light transmitted through the medium (tissue, bone, and/or blood vessels) is detected, while backscattered or reflected light is detected in the reflection mode. In the PPG sensors’ transmission mode, the sensing locations are limited owing to confined transillumination [46]. Therefore, the location of PDs in transmission mode is limited by the thinness of the subject, such as on the fingers, earlobes, and neonatal feet. Conversely, in the reflection mode, the LEDs and PDs are integrated into the same plane, possibly located on various spots, such as the forehead, forearm, abdomen, and legs (Figure 2a).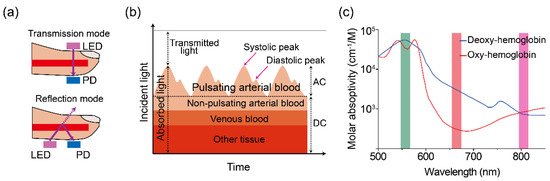 Figure 2. (a) Illustration of a two-mode (transmission and reflection) PPG sensor. (b) Variation in tissue light attenuation. (c) Molar absorptivity of oxygenated (blue line) and deoxygenated (red line) hemoglobin in arterial blood as of wavelength. Reproduced with permission from [50,51], ELSEVIER (1997) and SPIE (1999).The PDs can detect changes in light intensity from transmitted and/or reflected light in response to volumetric changes in veins and capillaries. As shown in Figure 2b, the typical PPG waveform consists of direct current (DC) and alternating current (AC) components. The DC component is caused by the absorption of nonpulsating arterial blood and scattering in all tissues, while the AC component is attributed to the volumetric change of arterial blood between systolic and diastolic phases in cardiac cycles [47,48]. The height of the AC signal fluctuates over time due to arterial blood pulsed by the heartbeat.Pulse oximetry is a revolutionary method for evaluating oxygen saturation levels (SpO2) using PPG devices. In a theoretical estimation, the oxygen saturation of the arterial blood can be expressed as the amount of oxygenated hemoglobin against the full quantity of hemoglobin: % SpO2=HbO2HbO2+Hb×100 %
Figure 2. (a) Illustration of a two-mode (transmission and reflection) PPG sensor. (b) Variation in tissue light attenuation. (c) Molar absorptivity of oxygenated (blue line) and deoxygenated (red line) hemoglobin in arterial blood as of wavelength. Reproduced with permission from [50,51], ELSEVIER (1997) and SPIE (1999).The PDs can detect changes in light intensity from transmitted and/or reflected light in response to volumetric changes in veins and capillaries. As shown in Figure 2b, the typical PPG waveform consists of direct current (DC) and alternating current (AC) components. The DC component is caused by the absorption of nonpulsating arterial blood and scattering in all tissues, while the AC component is attributed to the volumetric change of arterial blood between systolic and diastolic phases in cardiac cycles [47,48]. The height of the AC signal fluctuates over time due to arterial blood pulsed by the heartbeat.Pulse oximetry is a revolutionary method for evaluating oxygen saturation levels (SpO2) using PPG devices. In a theoretical estimation, the oxygen saturation of the arterial blood can be expressed as the amount of oxygenated hemoglobin against the full quantity of hemoglobin: % SpO2=HbO2HbO2+Hb×100 %

where HbO2 and Hb are the concentrations of oxy and deoxygenated hemoglobin, respectively. Typically, a pulse oximeter utilizes two different wavelengths of light. One is red and the other is infrared with wavelengths of 660 and 940 nm, respectively. The absorption intensity of light differs significantly depending on the oxygenated condition of hemoglobin. The iron-containing hemoglobin in the red blood cells can bind and transport oxygen during internal respiration. As shown in Figure 2c, the absorption spectra of hemoglobin varied under oxy/deoxygenated conditions. Significantly lower absorption in red (660 nm) light and slightly higher absorption in infrared (940 nm) are observed for oxyhemoglobin compared to deoxyhemoglobin [49]. The red/infrared modulation ratio (R), double-ratio of pulsatile (AC), and nonpulsatile (DC) components in red and infrared light can be used to calibrate the SpO2 level as follows:
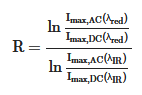
where A is absorbance. The calculated values of the modulation ratio R correspond to the SpO2 level. Considering low oxygenated conditions, for example, the amplitude of the AC component in the red-light region decreases compared to its behavior in the IR light region owing to the relatively higher absorption coefficient of deoxyhemoglobin at 660 nm (Figure 2c), resulting in a low R-value.
3.2. Applications of PPG Sensor
In clinical practice, the accurate measurement of the clinically relevant hemoglobin derivatives and bilirubin levels can provide useful diagnostic information. Figure 3 shows the absorption spectra of hemoglobin derivatives and bilirubin that can be further studied using skin-compatible PPG sensors.
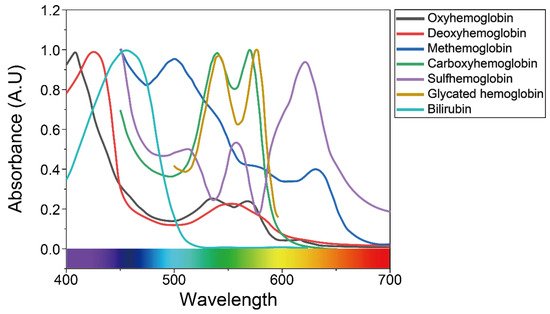 Figure 3. Absorbance of bilirubin and various types of hemoglobin in the visible light region, as mentioned in previous studies. Reproduced with permission from [58,59,60], ELSEVIER (1981), SPIE (2012), and ACS Publications (2016).
Figure 3. Absorbance of bilirubin and various types of hemoglobin in the visible light region, as mentioned in previous studies. Reproduced with permission from [58,59,60], ELSEVIER (1981), SPIE (2012), and ACS Publications (2016).
Methemoglobin (MetHb), along with carboxyhemoglobin (COHb) and sulfhemoglobin (SHb), represents a dyshemoglobin that does not bind O2. Normally, only small traces of MetHb and carboxyhemoglobin (COHb) are found in the blood, while sulfhemoglobin (SHb) is absent [52,53]. However, levels of MetHb and COHb are often elevated in severely ill patients, including clinical hypoxia [54], exposure to certain toxic agents [55], smokers [56], and the lack of genetic reductase [57].
Several observational studies reported the benefits of the continuous monitoring of MetHb and COHb levels to identify patients with carbon monoxide poisoning at triage in the hospital emergency departments [61,62,63]. Unlike MetHb, which is reversible with an antidote, methylene blue [64], SHb is an irreversible form of oxidized hemoglobin resulting from the incorporation of a sulfur atom in its porphyrin ring [65,66]. Currently, devices such as co-oximeters and blood gas analyzers are used to detect the abnormal presence of MetHb and SHb in blood samples [67,68]. However, the detection tests are not performed routinely in most intensive care units due to cost. The readings provided by those devices are not reliable, giving a false-positive result for methemoglobinemia [69]. Therefore, the noninvasive and low-cost approaches in the detection of MetHb and SHb at the point-of-care would be useful for the early detection of cyanotic conditions. Glycated hemoglobin (HbA1c), which is formed by the binding of hemoglobin, reflects the average blood glucose level over the preceding 60 days [70]. A range of studies [71,72,73,74] have demonstrated the benefits of point-of-care HbA1c testing, and the rapid availability of HbA1c testing has been shown to facilitate safe and effective diabetes management. Bilirubin levels are routinely monitored in cases of neonatal jaundice to identify hyperbilirubinemia and to prevent bilirubin-related neurotoxicity [75,76]. Many laboratory devices and methods are available to measure bilirubin levels in the blood. However, results are obtained 24 h after testing leading to delays in treatment. Thus, there is an important need for an accurate point-of-care system that allows rapid and appropriate treatment.
For the continuous and accurate evaluation of health status, securing stable adhesion between the light-responsive active components of PPG sensors and the target surfaces is crucial by minimizing motion artifacts [77]. Additionally, the devices percutaneously monitoring biometric signals require avoidance of toxicity, electric shock, electrolysis, and excessive thermogenesis [78]. To improve these problems, it is necessary to focus on the development of materials. In the next section, an innovative strategy for human skin-compatible PPG sensors depending on different types of light-absorbing semiconducting materials is highlighted.
This entry is adapted from the peer-reviewed paper 10.3390/app11052313