Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Subjects:
Rheumatology
Giant cell arteritis (GCA) is an autoimmune disease affecting large vessels in patients over 50 years old. It is an exemplary model of a classic inflammatory disorder with IL-6 playing the leading role.
- giant cell arteritis
- pathogenetic mechanism
- monocytes
1. Introduction
Giant cell arteritis (GCA) stands out as the most prevalent form of primary systemic vasculitis in the elderly [1]. It is an autoimmune granulomatous disease that can affect large arteries with a notable predilection of the aortic arch and its branches. The superficial cranial branches of the external carotids, along with the ophthalmic branch of the internal carotid artery, are typically involved. Despite historical recognition of the systemic repercussions, manifested through constitutional symptoms and elevated inflammatory marker levels, GCA has traditionally been considered a predominantly cranial disease [2]. However, applying advanced imaging techniques has unveiled a broader spectrum, extending beyond cranial vasculature to involve other extracranial large and medium-sized vessels, underscoring the inherently systemic nature of GCA at the tissue level [3] (Figure 1). GCA is often associated with polymyalgia rheumatica (PMR), characterized by abrupt-onset pain, aching, and morning stiffness in the shoulder and hip girdle muscles. PMR is also an independent disease, suggesting that these two disorders could represent distinct expressions of a common underlying pathological process [4].
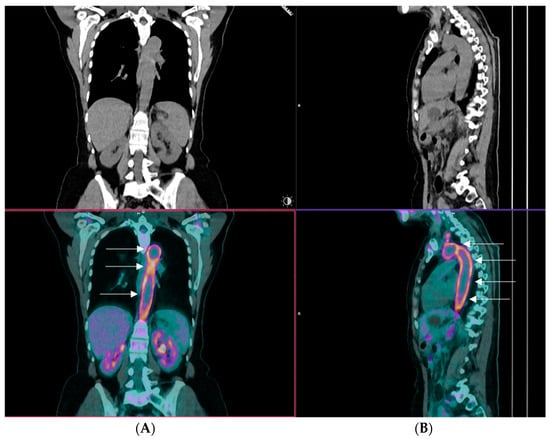
Figure 1. A representative image of an 18F-fluorodeoxyglucose positron emission tomography/computed tomography (PET/CT) of a patient with giant cell arteritis and extracranial large vessel involvement. The image displays coronal (Panel (A)) and sagittal views (Panel (B)), highlighting robust tracer uptake within the arch of the aorta, which is shown by arrows (kindly provided by our collaborator Dr CD Anagnostopoulos (BRFAA)).
1.1. Epidemiology
Despite its global prevalence, GCA exhibits geographic variability in its incidence and prevalence. Regardless of the diagnostic criteria used, several studies consistently identify people of northern European ancestry with the highest reported incidence (44 cases per 100,000 persons aged more than 50 years) and Asians, particularly in southeast Asia, as the area with the lowest (0.4 per 100,000 persons aged 50 years and above) [5]. Notably, there is a discernible north-to-south decreasing gradient even across Europe, highlighting the potential influence of ethnic origins in disease development. Females exhibit an almost threefold increased likelihood of developing GCA compared to males, with a propensity for more extracranial artery involvement and a higher prevalence of PMR [6]. Seasonal variation adds another layer to the epidemiological profile, with a notable preponderance of diagnoses during the spring and summer [7,8].
1.2. Risk Factors
Among the various risk factors associated with the development of GCA, age emerges as the single most important determinant. GCA abstains from affecting individuals under the age of 50, and after that, its incidence steadily ascents, with more than 80 percent of diagnosed patients surpassing the age of 70 [9]. This age-dependent pattern highlights the intricate interplay between aging and the pathogenesis of the disease. The etiology hangs between the age-related restructuring of the immune system and the age-related vascular remodeling and dysfunction. Immunosenescence, characterized by the reduction of the naïve T-cell pool, contraction of T-cell diversity, and accumulation of memory T-cells, is accompanied by low-grade inflammation, commonly referred to as inflammaging [10]. Vascular aging introduces pivotal changes in the structural properties of the vascular wall, leading to increased arterial stiffness and reduced compliance [11]. The interplay between these two aging-related phenomena forms a complex network that contributes to the initiation of GCA. Unraveling the most prominent driving forces in the aging process remains a critical challenge for a better understanding of the pathophysiology of GCA.
1.3. Clinical Picture
Regardless of the underlying pathogenetic origins, GCA presents with a variety of clinical features extending from constitutional symptoms to headaches, scalp tenderness, jaw claudication, and visual manifestations [12]. The onset of the disease typically follows a subacute trajectory over several weeks, although abrupt presentations are not uncommon. If left untreated, GCA poses the ominous risk of its most dreaded complication, permanent visual loss and, less frequently, stroke. Notably, recent reports indicate a decline in the incidence of visual loss, dwindling from 20% of patients to less than 10%, attributed to the advancements in awareness, timely diagnosis facilitated by rapid temporal artery color Doppler ultrasonography assessment [13], and swift medical intervention [14]. Although visual loss can occur abruptly and without warning, single or multiple episodes of transient visual loss (amaurosis fungax) may precede [15]. These brief episodes, though temporary, serve as critical warning signs, offering a window of opportunity for prompt recognition and initiation of treatment. According to the latest recommendations from EULAR in 2023, ultrasound, including assessment of the axillary arteries, is now advocated as the first-line imaging diagnostic test for GCA. If there is a high clinical suspicion coupled with a positive imaging test, a biopsy can be omitted from the diagnostic procedure [16]. However, clinical suspicion should always be heightened for GCA mimickers, with the most prominent being ANCA vasculitis, amyloidosis, and atherosclerosis [17]. Lately, COVID-19 has also been added to the list of conditions with similar presenting symptoms, such as headaches and acute phase responses. Thrombocytosis may lean more towards GCA, while lymphopenia may suggest COVID-19, aiding in the correct diagnosis [18].
2. Pathogenetic Mechanism in GCA
2.1. Initiation Phase
Similar to almost all systemic autoimmune and autoinflammatory disorders, the triggering factor(s) of GCA remains unknown. Several reports in the past have tried to elucidate the role of infections. Furthermore, tissue alterations via intrinsic mechanisms such as cell stress and accelerated atherosclerosis have also been proposed as initiating disease events. The lack of spontaneous experimental models, along with the poor understanding of tissue injury in GCA at the very early stages of the disease, are serious obstacles to understanding the initial mechanistic events. The initiating elements, when present, act synergistically upon a particular gene profile of patients with GCA that extends from antigen presentation (MHCs), adaptive and innate immunity genes (e.g., IL-2, IFN-γ), and several regulatory genes (e.g., TLRs).
2.1.1. Genetics
The genetic component has been considered an essential factor in GCA pathogenesis, based mainly on two observations: (i) reports on familial clustering of the disease [23,24,25] and (ii) an increased prevalence in Europeans of northern and Scandinavian ancestry [26]. With the utilization of molecular techniques from different scientific groups, they sought to decipher the genetic landscape of the disease. In the past two decades, genetic studies have been categorized into two types, according to the candidate-tested genes: (i) studies of targeted gene polymorphisms associated with disease susceptibility and (ii) genome-wide association studies.
In the first category, the main focus of research has included genes encoding the human leukocyte antigen (HLA) classes I and II and different molecules participating in the inflammatory response of GCA (IL-1β, IL-6, IL-10, IL-17A, IL-21, IL-23R, IL-33, TNF-α, VEGF, MMP-9, MPO, and others). Several studies in small patient cohorts interrogated the role of the HLA region in the disease. They revealed an association of GCA with the expression of HLA-DRB1*04 alleles (HLA-DRB1*0401, HLADRB1*0404, and HLADRB1*0408 haplotypes) [27,28,29,30,31,32,33,34,35,36]. Studies of genes encoding inflammatory molecules yielded various results. The rs2250889 polymorphism of the MMP-9 gene was associated with GCA susceptibility, but the study included only 30 patients [37]. Salvarani et al. demonstrated an association of the G/R 241 SNP in the ICAM-1 gene with the disease [38], but Amoli et al. reported a lack of association [39]. These studies included several weaknesses in sample size, lack of successful replicability, absence of appropriate geographical sample representation, and the use of low throughput technologies that did not allow for a large number of tested SNPs [40].
The research in this field entered the high-throughput screening era, producing more interesting results for the community. A large-scale study revealed that the HLA class II region is strongly associated with GCA [41], differentiating GCA from other systemic vasculitides that are genetically linked to HLA class I molecules (Takayasu arteritis, Behçet’s disease) [42] and supporting the implication of antigenic presentation processes in the initiation phase of the disease. A genome-wide association study (GWAS) confirmed this association, in addition to the identification of the plasminogen (PLG) gene polymorphism rs4252134 and the Prolyl 4-hydroxylase subunit alpha-2 (P4HA2) gene polymorphism rs128738 as genetic risk factors in GCA [43]. Furthermore, a meta-analysis highlighted the IL12B gene polymorphism rs755374 as a new risk SNP for GCA and a re-verification of the strongly associated HLA class II genes [44].
Overall, different studies exploring the contribution of SNPs in genes encoding proteins associated with the proinflammatory and tissue remodeling phases of GCA suggested the relevance of a plethora of innate and adaptive immunity molecules to disease pathogenesis. Additionally, GWAS introduced new genes as risk factors in GCA and reinforced the hypothesis of an unknown antigen-driven immune response initiating the pathogenesis of the disease.
2.1.2. Infections and Microbiome
The antigen-driven hypothesis of triggering the initiation of vascular inflammation observed in GCA has been a matter of debate for many years in the literature. In this direction, several studies have investigated the implication of different infectious agents in vascular dendritic cell activation and subsequent disease onset [81]. Of the infectious agents interrogated, human herpes virus (HHV)-6, HHV-7, varicella-zoster virus, and Epstein–Barr virus have not been associated with GCA. Although cytomegalovirus, parvovirus B19, herpes simplex virus, human parainfluenza 1, and chlamydia pneumonia were initially correlated with the disease, none of these results were confirmed by subsequent studies in larger cohorts [81]. A previous study reported the presence of varicella-zoster virus (VZV) antigen in 64–73% of temporal artery biopsies (TABs) of large vessel vasculitis (LVV) patients, with or without temporal artery involvement, as opposed to 22% of normal arteries tested [82]. Although this finding implied a possible disease-causing mechanism of VZV infection, the study lost its validity after Pisapia et al. reported an increased false-positive rate due to non-specific staining of the antibody used in the immunohistochemistry assay for VZV detection [83].
State-of-the-art approaches such as whole genome sequencing and 16S Ribosomal RNA gene sequencing have also been utilized in search of infectious agents implicated in GCA pathogenesis. In a shotgun sequencing-based study, none of the previously reported pathogens were detected in GCA TABs. Moreover, the microbiome did not differ between GCA cases and controls since only members of the normal skin flora were observed [84]. Two studies of another group that followed aseptic techniques during tissue collection found that the microbiome of thoracic aortic aneurysms from isolated aortitis and GCA differ substantially from the microbiome of non-inflammatory aortic aneurysms [85] and that from TABs of GCA patients [86]. These studies provided novel insights into the candidate role of the microbiome of different vascular components in health and disease. However, the translation of these findings in a comprehensive manner that could enrich our knowledge of GCA pathogenesis still has a long way to go.
2.1.3. Vascular Aging/Inflammaging
Undoubtedly, increasing age is a major etiological factor in GCA’s initiation, with different compartments of immunity being affected [11]. T-cells, in particular, exhibit a senescent phenotype due to the loss of the CD28 cell surface marker [87]. CD4+ CD28− and CD8+ CD28− cells are reported to be enriched in T-cell subsets of aged individuals [88]. There is also a marked decrease in the numbers of naïve T-cells and the T-Cell Receptor (TCR) repertoire diversity as opposed to an increase in T effector and memory cells [89]. Dendritic cells (DCs) can also be impacted by aging, displaying impaired activation and migration capacity [90]. Senescent macrophages display an altered, more inflammatory phenotype characterized by the expression of proinflammatory mediators (IL-1β, IL-6, TNF-α) [91]. It is reported that epigenetics may play a vital role during this so-called inflammaging process. Indeed, DNA methyltransferase 1 (DNMT1) levels in T-cells are decreased during the aging process [92]. DNMT1 is an enzyme that facilitates the maintenance of DNA methylation levels between cell divisions, a disturbed process during aging that leads to altered methylation levels in T-cells, a phenomenon associated with increased risk for autoimmunity and cancer. On the other hand, structural arterial changes are observed that correlate with increasing age, including calcium deposition, increased artery stiffness, wall thickening, and alterations in the extracellular matrix of the arteries [93]. The effect of inflammaging on the immune system, which is disturbed in GCA, and the vasculature, the target organ of the disease, supports the central role of senescence in GCA pathogenesis.
2.2. Perpetuation and Sustainability of the Inflammatory Response
Different studies of tissue biopsies of GCA patients reveal many types of immunocytes involved in innate and adaptive immune responses that are usually activated as attested by cellular markers and cytokines. Essentially, the perpetuation of tissue inflammatory response is performed through acute DTH mechanisms in which activated monocytes play a central role. At the same time, sustainability is implemented through chronic DTH responses with granuloma formation, which is the histological hallmark of the disease. In some instances, the local autoimmune injury is probably continuously fueled by the formation of ectopic germinal centers [94]. Disturbances in immune cell subpopulation frequencies in peripheral blood mononuclear cells (PBMCs) are also observed during active and inactive disease states [95]. An unmet need of GCA is the exact definition of cells participating in the acute inflammatory response in correlation with the cells in remission. Indeed, the type of cells and the inflammatory mediators differ in the acute and remission phases since the metabolic landscape is also different [96]. To this end, other groups and ours have suggested the investigation of pairs of biological samples in both activity and remission states in an attempt to gain clinically relevant biomarkers. Hereafter, the types and functions of major immune cell types are described.
2.2.1. Dendritic Cells and TLRs
The activation of resident DCs and subsequent activation of T-cells in the affected GCA arteries is thought to be the initial step of the intense inflammatory response. Following sensing intrinsic or extrinsic antigens, these cells induce strong innate and adaptive immune responses via TLR ligation and cell activation, which leads to chemokine and cytokine production, orchestrating tissue infiltration from T-cells. Thus, TLR differential expression and activation in the context of this pathology is of great importance [97].
Resident DCs observed in the adventitia of normal arteries display an immature phenotype [98,99] and contribute to immune surveillance. Detection of activated DCs in TABs is not exclusive to GCA but has also been described in TABs of patients with PMR. Activated DCs are located in the adventitia of PMR patient TABs as opposed to GCA patient TABs, in which activated DCs are extended in all three layers of the vascular wall [99]. Moreover, DCs are restricted to the artery and do not migrate to lymph nodes [98], a phenomenon facilitated by a positive-feedback loop of specific chemokine production (CCL19 and CCL21) and their receptor, CCR7 [99], leading to the migration of more DCs at the site of inflammation and restricting their escape to the lymph nodes. Additionally, DCs express CD83, an activation marker, and CD86, a co-stimulatory molecule that renders them capable of activating naïve T-cells. A study in a human artery–mouse chimera model of GCA showed that DC depletion with an antibody against CD83 was able to effectively reduce the inflammatory response, T-cell infiltration, and IFN-γ production [99], recapitulating the significance of DCs in the initial inflammatory cascade of GCA. It has also been demonstrated that the immunoprotective PD-1/PD-L1 immune checkpoint is defective in GCA-affected tissue DCs, thus rendering them more susceptible to activation [100]. Interestingly, a study investigating the expression profile of TLR genes of 6 GCA-affected arteries obtained during autopsy showed a distinct TLR profile for each affected vessel studied [101]. Until recently, there were no reports on DC subpopulations in the peripheral blood of GCA patients. Reitsema et al. investigated the frequencies of DC subsets in the peripheral blood of GCA and PMR patients compared to healthy individuals for the first time [102]. The authors noted that plasmacytoid DCs (pDCs) and type-2 conventional dendritic cells (cDC2) frequencies did not differ between patients and controls, whereas cDC1 frequencies were substantially reduced in patients. Additionally, in GCA/PMR patients, pDCs exhibited higher expression of the immune checkpoint CD86 and reduced expression of CD40, whereas cDC2 subsets exhibited lower activation status as shown by lower HLA-DR activation marker expression [102]. Overall, the interpretation of these results is challenging in understanding GCA pathogenesis since there are no surrogate data of DC subsets on the inflamed tissue level.
Examining the mechanism of DC activation in the context of the disease is pivotal in understanding the clinical heterogeneity in GCA, with some patients exhibiting disease restricted to temporal arteries while others display a more pronounced inflammatory response in different large vessels. A multidimensional study correlating TLR repertoire, pathogen expression (bacteria and viruses), and the activation status of different DC subpopulations in different anatomically affected arteries has never been conducted and may provide insights into understanding the etiology and initiation phase of GCA.
2.2.2. CD4 T-Cells
In GCA, a pronounced T-cell compartment participates in the underlying inflammation [103]. Indeed, activated DCs recruit CD4+ T-cells at the site of inflammation through CCL18, CCL19, CCL20, and CCL21 chemokine expression [104]. Upon arrival, activated CD4+ cells differentiate into Th1 and Th17 T-cell subsets through proinflammatory signals of the inflamed artery (IL-1β, IL-6, IL-12, IL-18, and IL23) [105,106]. In Th1 responses, CD4+ cells, under the influence of IL-12 and IL-18, differentiate into Th1 cells that secrete IFN-γ [107], a critical regulatory cytokine in the disease’s pathogenesis [108]. On the other hand, Th17 responses include the differentiation of CD4+ cells into Th17 cells under the effect of IL-1β, IL-6, and IL23 [107]. It is well established that these two T-cell axes operate in the vicious, inflammatory cycle observed in the disease. However, the order of appearance of Th1 and Th17 responses is unknown. GC treatment is highly effective in restricting Th17 responses, as proved by the reduction of both the number of Th17 cells in the peripheral blood and IL-17 serum levels [105,109]. However, IFN-γ producing Th1 responses show resistance after GC treatment in GCA patients [105,110].
Another dysregulated CD4+ subset implicated in GCA pathogenesis is T regulatory cells (Tregs). Tregs are reduced in both peripheral blood and at the tissue level in GCA [105,106,111]. Moreover, the high levels of IL-6, IL-21, and IL-23 in the inflamed tissue microenvironment lead to the restricted expression of FOXP3 transcriptional factor, which is crucial for the differentiation of Tregs, favoring the upregulation of RORγt transcriptional factor that mediates Th17 differentiation [112]. An imbalance of the Th17/Treg axis participating in the GCA pathogenetic mechanism has been observed and is restored by IL-6R blockade as shown by normalization in Treg peripheral blood frequencies and a decrease in activation status [111,113]. Miyabe et al. also highlighted that Tregs in GCA present a reduced suppressor capacity, possessing a proinflammatory phenotype with increased production of IL-17 [114].
Recent evidence has emerged for the role of Th9 cells in GCA. Th9 cells constitute a distinct lineage of T-cells differentiated from CD4+ naïve cells under the influence of IL-4, TGF-β, and thymic stromal lymphopoietin (TSLP) and are effective producers of IL-9. In GCA, Th9 cells are mainly observed in artery tissues with transmural inflammation and small vessel vasculitis, as opposed to their absence in vasa vasorum vasculitis [115]. Furthermore, patients with GCA exhibit a defective, macrophage-induced CD155-CD96 immune checkpoint that leads to Th9 expansion [116]. The same study showed increased vessel wall destruction due to increased IL-9 production in a humanized mouse model of GCA [116]. Although all groups have not demonstrated the functions and disease relevance of the Th9 subset in GCA, their implication in the pathogenic phenomena appears important and requires further research.
GCA-affected tissue may possess ectopic germinal center (EGC)-like structures that are important for perpetuating local inflammatory responses. In the formation of such structures, Follicular helper T (Tfh) cells play a central role. Tfh cells have been detected in the inflamed artery and the peripheral blood of GCA patients [117]. Tfh cells are capable of producing IL-21, which, among other functions, increases B-cell differentiation into plasmablasts and triggers germinal centers to produce immunoglobulins [118]. However, autoantibodies characterizing the disease have not been detected yet.
2.2.3. CD8 T-Cells
For years, the role of CD8+ T-cells in GCA has not attracted much attention due to their low number in both the periphery and tissue [119,120,121]. Nonetheless, CD8+ cells present oligoclonality in GCA tissue. They may infiltrate temporal arteries, producing proinflammatory cytokines such as IL-17A and IFN-γ as well as cytotoxic substances such as granzymes A and B [119]. These observations give rise, once again, to an antigen-driven theory of GCA initiation. Furthermore, a decreased number of immunosuppressive CD8+ CCR7+ FoxP3+ Tregs has been observed in the peripheral blood of GCA patients, potentially leading to a failure in the control of CD4+ T-cell proliferation and activation through a NADPH oxidase-2 dependent mechanism [122]. In addition, a decrease in CD8+ T-cells was associated with aging and GCA pathogenesis [122]. The fact that this defect was not abrogated by GC treatment in patients raises new questions about the pathogenetic role of CD8+ cells.
2.2.4. B-Cells
The role of B-cells in GCA had been overlooked for many years due to the initial reports of a low number of B-cells infiltrating the temporal artery [123,124], suggesting that humoral immunity plays a marginal role in the inflammatory process. Data on serum autoantibodies in GCA patients support a more active role for B-cells in the inflammatory process. Autoantibodies that were identified include (i) low titers of anti-cardiolipin of the IgG isotype that disappeared following GCs treatment [125,126,127,128]; (ii) anti-endothelial cell antibodies which were not specific for GCA and were also detected in other systemic vasculitides [129,130]; and (iii) anti-smooth muscle cell antibodies, but the study included a low number of patients [130]; additionally, (iv) Baerlecken et al. reported antibodies against the human ferritin heavy chain in a high percentage of GCA patients (92%) [131] while Régent et al. reported lower titers, but yet with high prevalence (71.9%) in GCA patients and 34% in patients with a diagnosis other than GCA diagnosis [132]. These results collectively support the idea that these autoantibodies are not disease-specific but an epiphenomenon of the inflammatory bulk.
In recent years, the formation of tertiary lymphoid organs (ATLOs) has been identified in the aortas of GCA patients but not in the affected temporal arteries [94,133]. Moreover, those ATLOs were found in the adventitia of inflamed aortas and were absent from GCA-positive temporal arteries, suggesting different organization according to the size of the affected artery. ATLOs consist of follicular dendritic cells located near T-cells and endothelial cells in the media layer, supporting the organization of lymphoid tissue against arterial wall-derived antigens. In the peripheral blood of treatment-naïve GCA and PMR patients, B effector cells are decreased compared to healthy controls and reach normal levels after GC treatment, exhibiting an enhanced IL-6 production capacity [134]. In contrast, serum levels of CXCL9 and CXCL13, major chemokines for the organization of ATLOs, are elevated [135,136]. The same study highlighted that B-cells were detected in the inflamed arterial tissue, and their migration pattern followed the CXCR3–CXCL9 and CXCR5–CXCL13 chemokine axes [136]. The above data indicate that B-cells in active disease are reduced in the peripheral blood due to their migration to the affected temporal arteries. In cases of large vessel involvement, ectopic lymphoid tissue is generated and is possibly connected to chronic inflammatory processes.
2.2.5. Monocytes
The abundant expression of IFN-γ in the initial steps of inflammation induces CCL2 expression by vascular smooth muscle cells (VSMCs), leading to tissue infiltration by monocytes of the classical subset, expressing the CCR2 receptor [137]. In addition, non-classical monocytes also participate in the inflammatory process and reach out to the tissue lesion under stimuli of the CX3CR1–CX3CL1 axis [138]. The predominant type of monocytes in the GCA tissue lesions is still a matter of debate, with different groups reporting either the classical monocyte subset [137] or non-classical subsets as the major monocytic type [138]. In the peripheral blood of GCA patients during diagnosis, elevated classical monocyte numbers [95,138] persisted after three months of GC treatment. Interestingly, disease remission correlated with a decrease in the number of intermediate and non-classical monocytic lineages, indicating that GCs act partly towards normalizing monocyte numbers [138]. Following integrative analysis of the methylome and transcriptome of CD14+ cells in GCA active and inactive disease, a recent study identified IL-11 as a novel cytokine pathway associated with the disease [139]. However, functional studies on the relevance of their findings to disease pathogenesis are needed.
2.2.6. Cytokines with a Significant Contribution to the Inflammatory Response of GCA
IL-6: IL-6 is considered to be the leading inflammatory cytokine in GCA’s pathogenetic mechanism. Serum levels of IL-6 appear to be elevated early during the disease course [105] and decrease rapidly after a few hours of GC initiation [140], without, however, reaching the levels of healthy individuals, even after chronic administration of GCs [141]. In addition, after GC tapering, IL-6 is among the first cytokines that arise in GCA patients’ serum [140]. IL-6 also correlates highly with acute phase reactants (erythrocyte sedimentation rate and C-reactive protein) and may serve as a biomarker of disease activity [142]. The above clinical observations made IL-6 a therapeutic target, and tocilizumab, a humanized monoclonal antibody to the IL-6 receptor (IL-6R), is now consistently used for patients with relapsing or refractory disease [143].
Although targeting of IL-6 is successful in therapy, the exact mechanism of action in GCA pathogenesis has not been elucidated, probably due to its pleiotropic effects. IL-6 is expressed by various immune and stromal cells, including activated monocytes, macrophages, B-cells, T-cells, fibroblasts, and endothelial cells [144]. IL-6 signal transduction is mediated by the complex IL-6/IL-6R/gp-130, with the latter being ubiquitously expressed, while hepatocytes, activated monocytes, macrophages, B-cells, and endothelial cells mainly express IL-6R. An established function of IL-6 is to control the balance between Th17 cells and Tregs [145], which is also evident in GCA [111,114]. The reduced frequency and the proinflammatory phenotype of Th17 expressing Tregs are reversed in GCA patients after tocilizumab treatment. There are conflicting reports on the effect of IL-6 on tissue remodeling. In a study by O’Neill et al., serum amyloid A (SAA) protein, which is triggered by IL-6 hepatocyte signaling and is increased in GCA patients’ serum, induced the protein expression of vascular endothelial growth factor (VEGF) and MMP-9 in an ex vivo culture model of temporal arteries. However, a more recent study of the same group argues a role of IL-6 in tissue remodeling since there was no effect of IL-6 treatment on myofibroblast proliferation and migration in a myofibroblast outgrowth culture model of GCA [146].
GM-CSF: Granulocyte-macrophage colony-stimulating factor (GM-CSF) has been recently suggested as a highly influential cytokine in GCA [147]. This proinflammatory cytokine is expressed by fibroblasts, endothelial, epithelial, myeloid, and T-cells upon appropriate stimulatory cues [148]. The GM-CSF heterodimeric receptor is composed of an α chain specific to GM-CSF and a signal transduction β chain, which is also found in the IL-3 and IL-5 receptors and, upon phosphorylation, triggers the activation of the JAK2/STAT5 signaling pathway [148]. Patient serum levels of GM-CSF are extremely low and comparable with healthy individuals [147]. On the contrary, GM-CSF protein levels are increased in GCA TABs [147] and PBMCs upon stimulation in vitro [106], suggesting a paracrine function of this cytokine on the inflamed tissue. The only functional study about GM-CSF in GCA was by Corbera-Bellalta et al. and highlighted the role of this cytokine in GCA. GM-CSF blockade by mavrilimumab, a fully human IgG4 monoclonal antibody to GM-CSFRα, abolished immune cell infiltration, inflammatory markers, and tissue remodeling factors, suggesting a role of GM-CSF in both the perpetuation of the inflammatory response and tissue injury phases [147]. A phase-2 clinical trial on mavrilimumab showed promising results on sustaining disease remission in week 26. However, further clinical trials are needed to determine whether this treatment modality is superior to current treatment options [149].
This entry is adapted from the peer-reviewed paper 10.3390/cells13050430
This entry is offline, you can click here to edit this entry!