Cannabis sativa L. (
C. sativa) is a flowering, fast-growing, 1–2 m in height, shrub plant belonging to the
Cannabis genus and Cannabaceae family.
C. sativa is commonly known as hemp, cannabis, or marijuana, originates from Central Asia, and is widely distributed in temperate and tropical areas [
1,
2,
3,
4,
5]. There are several preparations of
C. sativa, which can be smoked by a cigarette or a hash pipe, inhaled, or ingested in the form of candy or brownies; the most common is marijuana (dried, crushed flower tops, stems, and leaves of
C. sativa plant), and hashish (resins of the flowering tops of
C. sativa plant) [
6,
7,
8,
9].
The cannabis plant is very rich in phytochemicals; it contains more than 560 known compounds and there are over 120 cannabinoids identified in the literature [
1,
10,
11,
12]. Phytocannabinoids are known for their physiological and often psychotogenic effects; out of a large number of cannabinoids present in the cannabis plant,
trans-Δ-9-tetrahydrocannabinol (THC (1),
Figure 1) and cannabidiol (CBD (2),
Figure 1), are the most commonly described [
10,
13], in addition to other minor phytocannabinoids such as cannabinol ((3),
Figure 1), cannabigerol ((4),
Figure 1), and cannabichromene ((5),
Figure 1) [
14].
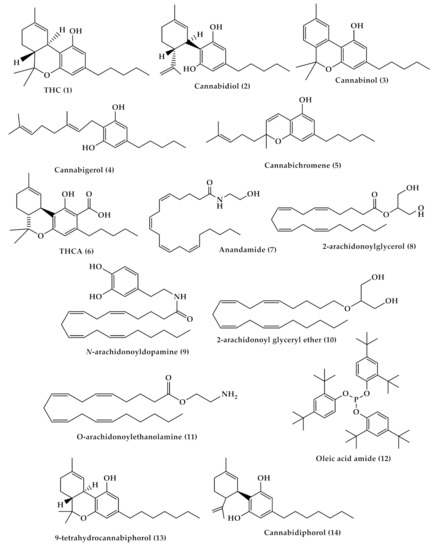
Figure 1. Chemical structures of Δ-9-tetrahydrocannabinol (THC, (1)), cannabidiol (2), Δ9- cannabinol (3), cannabigerol (4), cannabichromen (5) tetrahydrocannabinol-4-oic acid (THCA, (6)), anandamide (AEA, (7)) 2-arachidonoylglycerol (2-AG, (8)), N-arachidonoyldopamine (NADA, (9)), 2-arachidonoyl glyceryl ether (2-AGE, (10)), O-arachidonoylethanolamine (11), oleic acid amide (OA, (12)), Δ9-tetrahydrocannabiphorol (Δ9-THCP, (13)) and cannabidiphorol (CBDP, (14)).
Cannabis is used for recreational purposes in some geographic areas, and at the same time it is categorized as a drug of abuse with strict restrictions in most countries. Nowadays, cannabis legalization is increasing rapidly, with more than 200 million users worldwide, and for this reason it necessitates a greater awareness of its potential benefits and harms. According to the United Nations Office on Drugs and Crime (UNODC),
C. sativa is the most popular illicit drug of the 21st century. A dilemma surrounding cannabis safety and potential therapeutic effectiveness arises among researchers because most of the systemic reviews on cannabis use reported that cannabis has harmful outcomes and showed the clinical features of acute cannabis ingestion among children and adults that include anxiety, respiratory distress, decreased levels of consciousness, confusion and intoxication, psychiatric symptoms, and gastrointestinal adverse effects, especially among adults. Other reviews reported insufficient evidence of harm, or no evidence of harm outcomes, and encouraged cannabis legalization, showing its potential medical and therapeutic effects in treating different medical disorders such as cancer, neurological conditions, and others [
15,
16,
17,
18,
19,
20].
2. Cannabis Chemistry and Pharmacology
Cannabinoids can be classified into three groups according to their source of production: phytocannabinoids, endocannabinoids, and synthetic cannabinoids. The major cannabis chemical constituents are phytocannabinoids, which comprise a group of C21 terpene phenolic compounds, or C22 for the carboxylate forms, predominantly produced in cannabis. The plant also contains a wide range of non-cannabinoid terpenes and phenolic compounds [
14,
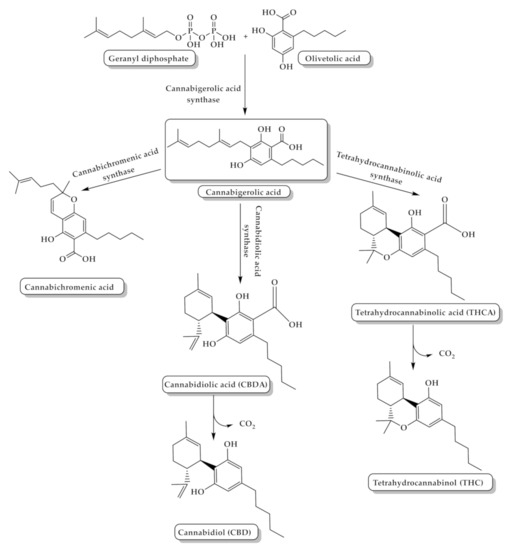
21]. Biosynthesis of phytocannabinoids is achieved by the coupling of olivetolic acid and geranyl diphosphate to produce different cannabinoids (
Figure 2) [
21].
Figure 2. The biosynthesis pathway of tetrahydrocannabinol (THC) and cannabidiol (CBD) from the coupling of olivetolic acid and geranyl diphosphate.
Phytocannabinoids are biosynthesized in carboxylated form and can be decarboxylated by heat [
22]. THC is the main and most potent psychoactive compound in cannabis that is responsible for the intoxicating effect which causes “highness” on consumption, and has a medical effect in which it can be used as an antiemetic and anti-inflammatory, in addition to its ability to reduce neuropathic and chronic pain [
23]. The potency of cannabis products is determined by their THC content [
24]. Δ9-tetrahydrocannabinol-4-oic acid (THCA (
6),
Figure 1) is the acidic precursor of THC and the major constituent of drug-type cannabis. THCA undergoes decarboxylation to THC by the heat of combustion during smoking [
3]. On the other hand, CBD is a non-intoxicating THC isomer with no psychotogenic effects, but it shows various pharmacological activities, such as pain and spasticity control [
25].
In the body, phytocannabinoids bind to specific receptors distributed throughout the body, which are called endocannabinoid receptors. Endocannabinoid receptors, along with their endogenous neurotransmitters N-arachidonoylethanolamine (anandamide, AEA) ((7),
Figure 1) and 2-arachidonoylglycerol (2-AG) ((8),
Figure 1), and the enzymes that are responsible for endocannabinoids synthesis and degradation, form the endocannabinoid system (ECS) [
26]. Recently, other molecules have also been considered as endocannabinoids, such as
N-arachidonoyldopamine (NADA, (9),
Figure 1), 2-arachidonoyl glyceryl ether (2-AGE, (10),
Figure 1),
O-arachidonoylethanolamine ((11),
Figure 1), and oleic acid amide (OA, (12),
Figure 1) [
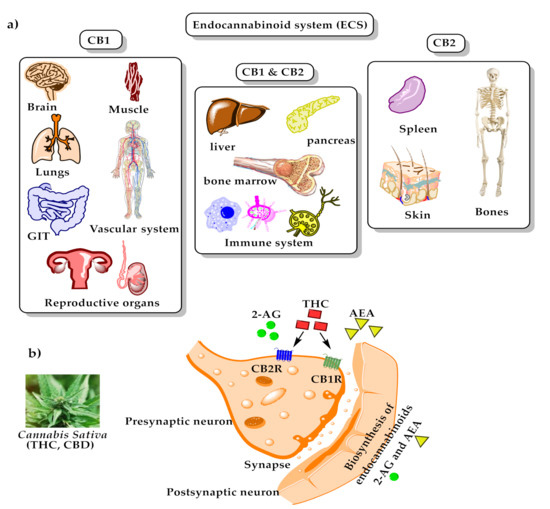
27]. There are two endocannabinoid receptors, CB1 and CB2, which belong to the G-protein coupled receptors family and are found in the immune tissues (where CB2 is mainly expressed) and in the central nervous system (where CB1 is mainly expressed and, hence, mediates the psychoactive effects of
Cannabis). Both exert inhibitory neuronal activity upon their interactions with the cannabinoids [
28,
29]. AEA has a high affinity for CB1 compared to CB2, while 2-AG has moderate affinity for both CB1 and CB2. Exogenous THC is a partial CB1 and CB2 agonist, while phytocannabinoid CBD has a low affinity for these receptors [
29,
30]. Recently, two phytocannabinoids were discovered and isolated from
Cannabis sativa: Δ9-tetrahydrocannabiphorol (Δ9-THCP, (13),
Figure 1), a Δ9-THC homolog that binds with high affinity to both CB1 and CB2, and cannabidiphorol (CBDP, (14),
Figure 1), a CBD homolog that has no available reports on its pharmacological effects yet [
31]. For the binding mode of some of the mentioned compounds with cannabinoid receptors type 1 (CB1) and type 2 (CB2), please see
Figure 3.
Figure 3. The endocannabinoid system; (a) distribution of endocannabinoids receptors through human body; (b) binding of endogenous anandamide (AEA), 2-arachidonoylsn-glycerol (2-AG), and exogenous Δ9-tetrahydrocannabinol (Δ9-THC) with cannabinoid receptors type 1 (CB1) and type 2 (CB2).
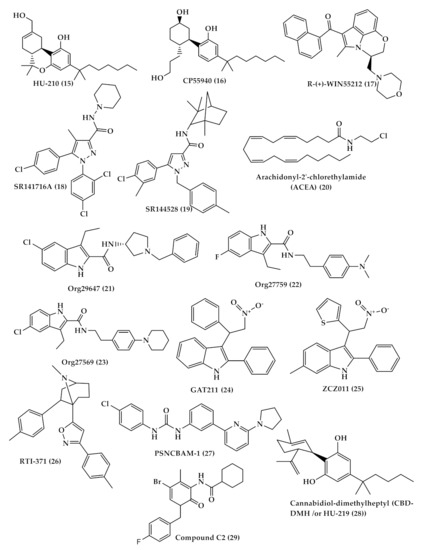
Several cannabinoid receptor agonists bind more or to a lesser extent to CB1 and CB2 receptors such as classical (THC and (−)-11-hydroxy-D8--THC dimethyl heptyl (HU-210) ((15),
Figure 4)), nonclassical (CP55940 (16),
Figure 4)), aminoalkylindole (R-(+)-WIN55212 ((17),
Figure 4)) which has a higher affinity to CB2 more than CB1 receptor) [
32], and antagonist-inverse agonists (SR141716A ((18),
Figure 4) for CB1 and SR144528 ((19),
Figure 4) for CB2) [
33]. In general, many antagonists show high selectivity toward the CB1 receptor which allows differentiation between CB1 and CB2, while numerous agonists show low selectivity between cannabinoid receptors. Despite that, some agonists, such as arachidonyl-2′-chlorethylamide (ACEA (20),
Figure 4) compound, show CB1 high selectivity [
33,
34,
35]. In addition, allosteric modulators that bind to different sites other than the ligand orthosteric site affect the stimulus of cannabinoid receptor by either enhancing or reducing its activity. Three allosteric modulators of CB1 were first described by Price et al.—Org29647 (21), Org27759 (22), and Org27569 (23) (
Figure 4)—which showed an enhancement of CP-55940 agonist binding to CB1 and reduction in SR141716 antagonist/inverse agonist binding [
36]. Other synthetic CB1 allosteric modulators were also developed, such as GAT211 (24), ZCZ011 (25), RTI-371 (26) and PSNCBAM-1 (27) (
Figure 4) [
37]. On the other hand, there are just two synthetic allosteric modulators of CB2 cannabidiol-dimethylheptyl (CBD-DMH /or HU-219 (28)) and compound C2 (29) (
Figure 4) [
38,
39].
Figure 4. Chemical structures of some synthetic agonist and antagonist cannabinoid; (−)-11-hydroxy-D8--THC dimethyl heptyl (HU-210) (15), CP55940 (16), R-(+)-WIN55212 (17), SR141716A (18), SR144528 (19), arachidonyl-2′-chlorethylamide (ACEA) (20), and allosteric modulators; Org29647 (21), Org27759 (22), and Org27569 (23), GAT211 (24), ZCZ011 (25), RTI-371 (26) and PSNCBAM-1 (27), cannabidiol-dimethylheptyl (CBD-DMH /or HU-219 (28)) and compound C2 (29).
Cannabinoids (both phytocannabinoids and endogenous) also interact with receptors other than cannabinoid receptors and act simultaneously on multiple targets within the nervous system, such as putative non-CB1/CB2 cannabinoid G protein-coupled receptor (GPCR) 55 [
40], transient receptor potential (TRP) channels, the N-arachidonoyl glycine (NAGly) receptor [
41,
42], and 5- hydroxytryptamine (5-HT) receptors [
43,
44].
3. Cannabis and Cannabinoids: Potential Therapeutic Uses
For thousands of years, the cannabis plant has been utilized in traditional remedies. Cannabis-induced analgesia is the most common reason for using cannabis medically. During the past several decades, synthetic chemical analogues of THC were made and are known as synthetic cannabinoids. Several innovative drugs, structurally similar to or mimicking the activity of THC and CBD, have been developed and applied clinically, or are still in clinical studies, for treating conditions like chronic pain, epilepsy, and multiple sclerosis, and for use as appetite stimulants and antiemetic agents in HIV/AIDS and cancer patients [
45,
46,
47]. Therefore, cannabinoids can provide a lead compound for new drug development.
Treatment with herbal cannabis and cannabis-based medicine can be administered in various routes, such as smoking, vaporization, oral, oromucosal, and others; which affect the absorption and toxicity of cannabinoids. Long-acting oral preparations are the mainstay of treatment for chronic conditions, and vaporization can be utilized as an add-on treatment for acute symptoms. Adverse events of cannabis are mainly attributed to THC; therefore, the total daily dose-equivalent of THC should generally be limited to 30 mg/day or less, preferably combined with CBD [
48]. In contrast to medical cannabis, recreational cannabis tends to be high in THC content to attain the euphoric high. In medical cannabis, some strategies should be applied to minimize the adverse effects of cannabis. Adverse effects of THC, such as fatigue, tachycardia, and dizziness, are avoided by starting with low doses and slow titration of cannabis preparations. The general approach of cannabis medical prescription is ‘start low, go slow, and stay low’. In addition, combining CBD with THC can balance THC side effects [
48,
49]. Medical cannabis patients frequently use CBD-predominant products with the minimum amounts of THC to have the best improvement in symptoms and quality of life, with the fewest adverse effects.
4. Cannabis Poisoning
Cannabinoid use as analgesics, antiemetics, appetite stimulants, and anti-spastics are already approved by regulatory bodies such as the US FDA, Health Canada, and the European Medicines Agency. However, several undesired effects may be associated with cannabis and synthetic cannabinoid (SC) use, such as psychosis and self-harm. Exposure to high concentrations of THC could lead to psychological and neurological events, such as dizziness, drowsiness, ataxia, seizures, hypotonia, stupor, coma, and ocular features such as mydriasis and conjunctival hyperemia, in addition to gastrointestinal disorders, and cardiovascular features such as tachycardia, arterial hypertension, and postural hypotension [
105,
106,
107,
108,
109,
110,
111,
112,
113]. However, the use of SCs can lead to more toxic side effects, which may be attributed to the low or no CBD content that has a protective role (anxiolytic and antipsychotic properties), and/or to the high affinity to CB1 receptors compared to THC. The use of SCs is associated with typical acute adverse effect (ex. euphoria, delusions, anxiety, panic attacks, vomiting, seizures, dizziness and others), cardiovascular side effects (tachycardia and hypertension), and long-term adverse effects (high abuse, dependence and tolerance) [
111,
113]. On the other hand, recreational use of cannabis is considered of low harm, but at the same time may cause damage to the physical and mental health of users in short- and long-term use. Several studies showed that medical cannabis users employed it for recreational reasons, and this may result in intolerable psychoactive effects in patients with no recreational experience, leading them to discontinue medical use [
114,
115]. Smoking dried cannabis leaves is the preferred consumption method for recreational use because it affords high bioavailability and easy preparation and dosing. Most users experience relaxation, mild euphoria, time distortion with little dysphoria, and anxiety effects, which can increase with the amplification of the THC content, especially in naive users [
116].
Cannabis intoxication is dose-related, and its absorbance depends on the route of administration and concentration being used. Inhaled doses of 2–3 mg and ingested doses of 5–20 mg of THC can affect memory and cause short-term memory impairment and loss of attention, while inhaled doses more than 7.5 mg/m2 in adults and oral doses of 5–300 mg in pediatric subjects can cause more serious effects, such as respiratory depression, panic, anxiety, hypotension, myoclonic jerking and other symptoms [
117]. The LD50 (the lethal dose at which 50% of the sample population dies) of THC is not determined in humans due to ethical reasons, but in animals it ranges from 40 to 130 mg/kg intravenously. The LD50 of THC inhalation from smoked cannabis in Fisher rats is 42 mg/Kg, a value that is similar to the IV vascular access port value, which indicates that THC is the active intoxicant of smoked cannabis [
117,
118].
Cannabis-induced adverse effects may be influenced by other several factors such as genetic variation, age, sex, ethnicity, and duration and frequency of cannabis use [
119,
120,
121]. Significant toxicity from cannabis and cannabinoid-containing substances is uncommon in adults, unlike children, who may develop significant symptoms. Fortunately, these toxicity symptoms are usually short-lived and last for several hours [
122,
123]. A case of cannabis poisoning was reported in a preschool child who was on oral hemp seed oil for three weeks after medical prescription to strengthen his immune system. The child exhibited acute neurological symptoms such as stupor and low reactivity to stimulation, associated with conjunctival hyperemia. THC was detected in the product ingested by the child, and the acid metabolite of THC was detected in the child’s urine [
124]. Carstairs et al. reported a case of a 14-month-old child who ingested hashish and was in a prolonged coma for more than 48 hours. The THC metabolite, 11-nor-carboxy-Δ9–THC, was detected in high levels in the patient’s urine, and the patient’s clinical improvement coincided with the decline of the THC metabolite’s level in urine [
125].
Generally, cannabis has modest harm that can be avoidable if the starting dose is low, and dose titration is slow. Medical use of cannabis may be associated with adverse events, like drowsiness, fatigue, dizziness, dry mouth, anxiety, nausea, cognitive effects, euphoria, blurred vision, headache, and orthostatic hypotension. Smoking medical cannabis is commonly associated with coughing, phlegm, and bronchitis [
126,
127,
128]. Recreational use is done with no calculated doses nor medical monitoring, likely to be heavy and sustained, and is done most commonly by harmful methods like smoking. Hence, recreational cannabis users are more prone to cannabis poisoning and toxicity.
5. Legalization of Cannabis
Cannabis legalization is rising in countries worldwide and the opinions about its use are split into supporters who believe that cannabis legalization can improve public health, stimulate the economy, and reduce criminal justice expenditure, while critics believe that legalization will increase cannabis use, which may affect health and safety, lower the educational achievement in teens, and increase crime [
256].
To date, the FDA has only approved one cannabis-derived drug product (Epidiolex (cannabidiol)) and three synthetic cannabis (dronabinol (Marinol and Syndros) and nabilone (Cesamet)) products, and did not approve any other cannabis or its derivatives. Cannabis is classified in Schedule I by the FDA, where substances that have high potential for abuse are restrictively categorized [
5,
257]. Cannabis being in Schedule I increases the complexity for research studies, because all researchers must follow Schedule I research registrations. In addition, cannabis is a controlled substance and researchers must obtain it from registered cultivators with the Drug Enforcement Administration (DEA) and licenses from the state-controlled drug authority [
257,
258]. Medical use of cannabis and cannabinoids must be supervised by medical practitioners and dispensed by prescription where the drug should be used only when necessary [
259]. Although cannabis is federally illegal in the US, nine US states have legalized adult recreational use of cannabis since 2012. Furthermore, in 1999, Canada allowed the use of cannabis for medical issues, and in 2018, it decriminalized and legalized recreational cannabis use. The UK also legalized medical cannabis in 2019, in addition to other countries worldwide. Changes in legalization laws and the liberalization of cannabis increase the need for more research to understand the cannabis plant and its effects, which may be available in the future [
260,
261,
262,
263].