India continues to grapple with a significant burden of HIV infections. Despite notable progress in prevention and treatment efforts, multiple challenges, such as high-risk populations, inadequate testing facilities, and limited access to healthcare in remote areas, persist. Though the Government of India offers HIV-1 plasma viral load testing at various medical centers, aiding treatment decisions and monitoring antiretroviral therapy effectiveness, enhancing care for individuals living with HIV under the National AIDS Control Program (NACP), the nation’s large population and diverse demographics further complicate its outreach and response. Hence, strategic interventions and alternative methods of testing remain crucial to curbing HIV transmission and improving the quality of life for those affected. Dried blood spot (DBS) sampling has emerged as a convenient and cost-effective alternative for HIV-1 viral load testing, revolutionizing the landscape of diagnostic and monitoring strategies for HIV infection. Though the plasma-based viral load remains the gold standard for monitoring HIV-1, DBS-based HIV-1 viral load testing holds immense promise for improving access to care, particularly in resource-limited settings where traditional plasma-based methods may be logistically challenging. DBS entails the collection of a small volume of blood onto filter paper, followed by drying and storage. This approach offers numerous advantages, including simplified sample collection, transportation, and storage, reducing the need for cold-chain logistics.
- HIV/AIDS
- HIV-1
- viral load
- dried blood spot (DBS)
- diagnosis
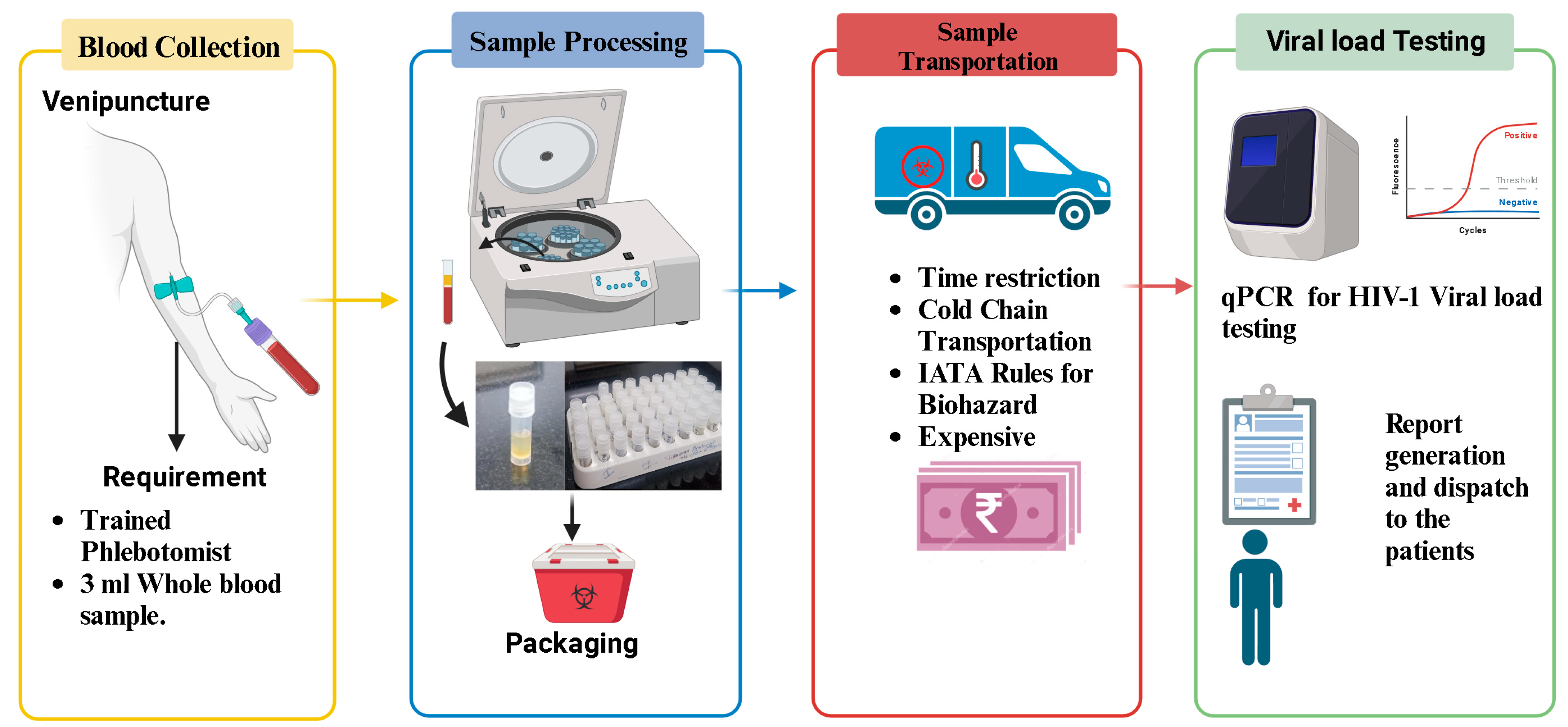
1. Conventional Method of HIV-1 Viral Load Testing
2. The Potential of Dried Blood Spot Analysis as a Convenient and Cost-Effective Alternative for HIV-1 Viral Load Measurement
3. Advantages of Dried Blood Spot over Plasma Specimen
| Assay Platform | VL Threshold | Sample Size | Sensitivity | Specificity | References |
|---|---|---|---|---|---|
| Abbott RealTime HIV-1, BioMerieux, Roche, and Siemens VERSANT | 1000 | 10,871 | >83% | >83% | [12] |
| Roche CAP/CTM, Abbott RealTime HIV-1, and the bioMérieux NucliSENS EasyQ | 1000 | 323 | 80% | 90% | [7] |
| Abbott RealTime HIV-1 | 1000 | 497 | 93% | 95% | [8] |
| Abbott RealTime HIV-1 | 1000 | 200 | 93% | 88% | [9] |
| Abbott RealTime HIV-1 | 1000 | 793 | 88.1% | 93.1% | [10] |
| Abbott RealTime HIV-1 | 1000 | 323 | 76.0% | 89.7% | [11] |
| Abbott RealTime HIV-1 | 2000 | 100 | 95% | Not reported | [13] |
| Abbott RealTime HIV-1 | 1000 | 130 | 50–100% | 100% | [14] |
| Abbott RealTime HIV-1 | 1000 | 203 | 90.1% | 96.2% | [15] |
| Abbott RealTime HIV-1 | 1000 | 87 | 94.8% | Not reported | [16] |
4. Feasibility Study Results of Implementation of Dried Blood Spot for Viral Load Testing in Different Setups
5. Principle of Dried Blood Spot-Based HIV-1 Viral Load Testing
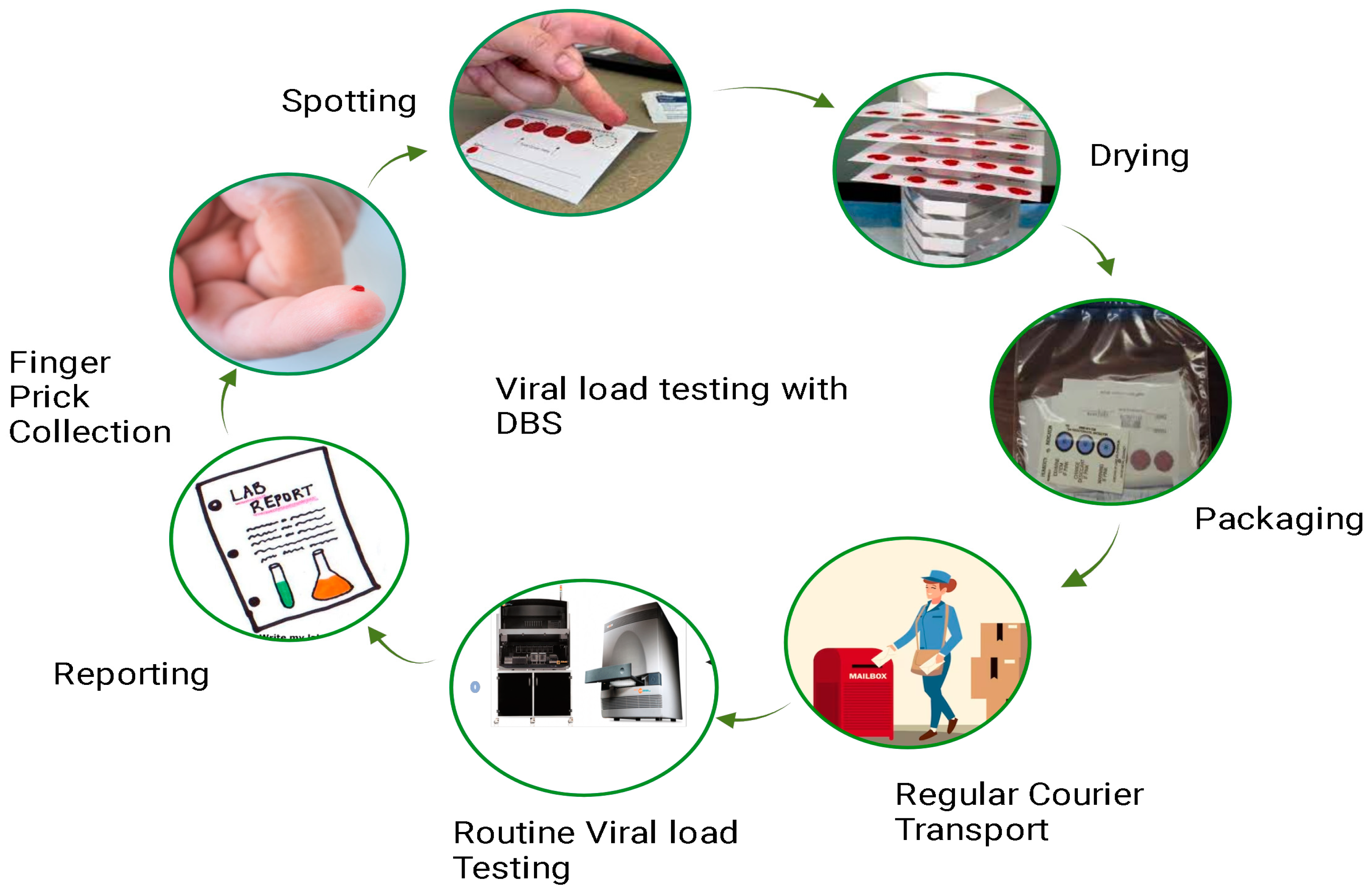
Methodology for Working with Dried Blood Spot
-
Blood Collection: A small volume of blood, usually obtained through a finger prick, is collected onto a filter paper card specifically designed for DBS collection. The filter paper absorbs the blood and preserves it.
-
Drying: The blood-soaked filter paper is allowed to air-dry completely, usually at room temperature. This step stabilizes the blood components on the filter paper, preventing degradation of the biological material.
-
Sample transport and storage: Once dried, the DBS card can be stored at room temperature for an extended period. This eliminates the need for immediate cold-chain transportation and storage, making it particularly advantageous in resource-limited or remote settings.
-
Sample extraction and analysis: To perform HIV-1 viral load testing, a small disc or punch is cut from the dried blood spot on the filter paper. This disc is then extracted to obtain the genetic material (RNA) of the virus. The extracted RNA is then subjected to nucleic acid amplification techniques, such as reverse transcription polymerase chain reaction (RT-PCR), to quantify the amount of HIV-1 viral RNA present in the blood.
This entry is adapted from the peer-reviewed paper 10.3390/healthcare12040413
References
- Blaurock, G.; Rische, H.; Rohne, K. Development of the blotting paper method in the dried blood reaction for syphilis. Dtsch. Gesundheitsw. 1950, 5, 462–464.
- Tuaillon, E.; Kania, D.; Pisoni, A.; Bollore, K.; Taieb, F.; Ontsira Ngoyi, E.N.; Schaub, R.; Plantier, J.-C.; Makinson, A.; Van de Perre, P. Dried Blood Spot Tests for the Diagnosis and Therapeutic Monitoring of HIV and Viral Hepatitis B and C. Front. Microbiol. 2020, 11, 373.
- WHO. Consolidated Guidelines on HIV Prevention, Diagnosis, Treatment and Care for Key Populations; WHO: Geneva, Switzerland, 2016.
- Simushi, P.; Kalunga, M.N.; Mwakyoma, T.; Mwewa, M.; Muchaili, L.; Hazeemba, N.; Mulenga, C.; Mwewa, P.; Chiyenu, K.O.R.; Kachimba, J.; et al. Verification of Dried Blood Spot as a Sample Type for HIV Viral Load and Early Infant Diagnosis on Hologic Panther in Zambia. BMC Res. Notes 2023, 16, 75.
- Makadzange, A.T.; Boyd, F.K.; Chimukangara, B.; Masimirembwa, C.; Katzenstein, D.; Ndhlovu, C.E. A Simple Phosphate-Buffered-Saline-Based Extraction Method Improves Specificity of HIV Viral Load Monitoring Using Dried Blood Spots. J. Clin. Microbiol. 2017, 55, 2172–2179.
- CDC. Shipping Guidelines for Dried-Blood Spot Specimens; CDC: Atlanta, GA, USA, 2017.
- Pannus, P.; Claus, M.; Gonzalez, M.M.P.; Ford, N.; Fransen, K. Sensitivity and Specificity of Dried Blood Spots for HIV-1 Viral Load Quantification: A Laboratory Assessment of 3 Commercial Assays. Medicine 2016, 95, e5475.
- Tang, N.; Pahalawatta, V.; Frank, A.; Bagley, Z.; Viana, R.; Lampinen, J.; Leckie, G.; Huang, S.; Abravaya, K.; Wallis, C.L. HIV-1 Viral Load Measurement in Venous Blood and Fingerprick Blood Using Abbott RealTime HIV-1 DBS Assay. J. Clin. Virol. 2017, 92, 56–61.
- Zeh, C.; Ndiege, K.; Inzaule, S.; Achieng, R.; Williamson, J.; Chih-Wei Chang, J.; Ellenberger, D.; Nkengasong, J. Evaluation of the Performance of Abbott M2000 and Roche COBAS Ampliprep/COBAS Taqman Assays for HIV-1 Viral Load Determination Using Dried Blood Spots and Dried Plasma Spots in Kenya. PLoS ONE 2017, 12, e0179316.
- Schmitz, M.E.; Agolory, S.; Junghae, M.; Broyles, L.N.; Kimeu, M.; Ombayo, J.; Umuro, M.; Mukui, I.; Alwenya, K.; Baraza, M.; et al. Field Evaluation of Dried Blood Spots for HIV-1 Viral Load Monitoring in Adults and Children Receiving Antiretroviral Treatment in Kenya: Implications for Scale-up in Resource-Limited Settings. J. Acquir. Immune Defic. Syndr. 2017, 74, 399–406.
- WHO. Public Reports of World Health Organization Prequalified IVDs: Abbott RealTime HIV-1 (M2000sp). PQDx 0145-027-00; WHO: Geneva, Switzerland, 2023.
- Gutema, G.; Hailu, H.; W/semeyat, B.; Yilma, A.; Abdela, S.; Kidane, E.; Adane, S.; Yimer, M.; Tsegaye, A. Effect of Sample Management on Quantitative HIV-1 Viral Load Measurement at Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia. PLoS ONE 2022, 17, e0269943.
- Vidya, M.; Saravanan, S.; Rifkin, S.; Solomon, S.S.; Waldrop, G.; Mayer, K.H.; Solomon, S.; Balakrishnan, P. Dried Blood Spots versus Plasma for the Quantitation of HIV-1 RNA Using a Real-Time PCR, M2000rt Assay. J. Virol. Methods 2012, 181, 177–181.
- Neogi, U.; Gupta, S.; Rodridges, R.; Sahoo, P.N.; Rao, S.D.; Rewari, B.B.; Shastri, S.; Costa, A.D.; Shet, A. Dried Blood Spot HIV-1 RNA Quantification: A Useful Tool for Viral Load Monitoring among HIV-Infected Individuals in India. Indian. J. Med. Res. 2012, 136, 956–962.
- Taieb, F.; Tran Hong, T.; Ho, H.T.; Nguyen Thanh, B.; Pham Phuong, T.; Viet Ta, D.; Le Thi Hong, N.; Ba Pham, H.; Nguyen, L.T.H.; Nguyen, H.T.; et al. First Field Evaluation of the Optimized CE Marked Abbott Protocol for HIV RNA Testing on Dried Blood Spot in a Routine Clinical Setting in Vietnam. PLoS ONE 2018, 13, e0191920.
- Benedicto, P.; Dladla, P.; Goba, G.; Shawa, I. Assessment of the Accuracy of Dried Blood Spot (DBS) Sample in HIV-1 Viral Load as Compared to Plasma Sample Using Abbot Assay. Int. J. Res. Med. Sci. 2013, 1, 338.
- Mwau, M.; Danda, J.; Mbugua, J.; Handa, A.; Fortunko, J.; Worlock, A.; Nair, S.V. Prospective Evaluation of Accuracy of HIV Viral Load Monitoring Using the Aptima HIV Quant Dx Assay with Fingerstick and Venous Dried Blood Spots Prepared under Field Conditions in Kenya. PLoS ONE 2021, 16, e0249376.
- Mahajan, N.B.S.; Aggarwal, S. Use of Dried Blood Spots as a Screening Method in STI Testing: A Mini-Review. Public Health Open Access 2022, 6, 000203.
- Kamble, S.; Shidhaye, P.; Mukherjee, A.; Tak, M.; Bembalkar, S.; Aggarwal, S.; Deb, A.; Kapoor, N.; Verma, V.; Das, C.; et al. A Protocol for Feasibility of Plasma Based GeneXpert Platform and Dried Blood Spot (DBS) Based Abbott Platform for HIV-1 Viral Load Testing among the People Living with HIV Attending ART Centers in India. PLoS ONE 2023, 18, e0285942.
- Nguyen, T.A.; Tran, T.H.; Nguyen, B.T.; Pham, T.T.P.; Hong Le, N.T.; Ta, D.V.; Phan, H.T.T.; Nguyen, L.H.; Ait-Ahmed, M.; Ho, H.T.; et al. Feasibility of Dried Blood Spots for HIV Viral Load Monitoring in Decentralized Area in North Vietnam in a Test-and-Treat Era, the MOVIDA Project. PLoS ONE 2020, 15, e0230968.
- Teran, R.A.; Sobieszczyk, M.E.; Chiasson, M.A.; Uhlemann, A.-C.; Weidler, J.; Shah, J.G.; Chang, J.Y.; Otto, C.; Hirshfield, S. Longitudinal Viral Load Monitoring Using Home-Collected Dried Blood Spot Specimens of MSM Living with HIV: Results from a Feasibility Pilot Study. AIDS Behav. 2021, 25, 661–666.
- Hrapcak, S.; Pals, S.; Itoh, M.; Peters, N.; Carpenter, D.; Hackett, S.; Prao, A.K.; Adje-Toure, C.; Eboi, E.; Mutisya, I.; et al. HIV Viral Load Scale-up Among Children and Adolescents: Trends in Viral Load Suppression, Sample Type and Processing in 7 PEPFAR Countries, 2015–2018. Pediatr. Infect. Dis. J. 2023, 42, e102–e104.
- Nguyen, L.B.L.; Soumah, A.A.; Hoang, V.T.; Nguyen, A.T.; Pham, T.H.; Royer-Devaux, S.; Madec, Y. Performances of Dried Blood Spots and Point-of-Care Devices to Identify Virological Failure in HIV-Infected Patients: A Systematic Review and Meta-Analysis. AIDS Patient Care STDS 2023, 37, 66–83.