1. Introduction
The prevalence of type 2 diabetes mellitus (T2DM) has been rising worldwide, reaching epidemic proportions in both high- and middle-income countries [
1]. Morbidity and mortality have also been rising dramatically due to diabetic complications, mainly chronic kidney disease (CKD) and cardiovascular disease (CVD) [
2].
Diabetic nephropathy is the leading cause of kidney disease globally [
3]. Albuminuria and a reduced glomerular filtration rate (GFR) are the main risk factors for end-stage CKD, CVD and death [
4].
CVD, specifically ischemic heart disease, coronary artery disease (CAD), heart failure (HF), stroke and peripheral artery disease, accounts for 50% of deaths in patients with T2DM, a number that rises in the context of CKD [
5].
Multiple initiatives have been launched to prevent diabetes, achieve optimal glycemic control, and identify and treat diabetic complications as early as possible. Intensive blood glucose control and the management of body weight, blood pressure and lipid levels are all recommended for T2DM patients with tailored treatment objectives and plans [
6]. The fundamental component of T2DM therapy continues to be lifestyle modifications, namely adopting a customized food plan and engaging in regular physical activity. However, a significant number of patients fail to adhere to this, and this is occasionally insufficient to protect the target organs [
7]. The current list of antidiabetic medications includes metformin, dipeptidyl-peptidase-4 inhibitors (DPP4i), glucagon-like peptide-1 (GLP1) receptor agonists, insulin, sulfonylureas, thiazolinediones and sodium-glucose transporter inhibitors (SGLT2i).
The target-organ protective strategy has taken the place of the glucose-center approach since rigorous monitoring of glucose has failed to lower the frequency of complications, particularly macroangiopathy [
8]. Through a recently proposed algorithm, the European Society of Cardiology (ESC) and the European Association for the Study of Diabetes (EASD) have emphasized the importance of taking into account factors other than glucose levels and HbA1c, such as the protection, early detection and treatment of diabetes’ main target organs, the kidney and the heart [
9]. GLP-1 receptor agonists are recommended as the first line of therapy for people with risk factors for CVD or those who already have the disease, based on favorable findings from trials with cardiovascular and renal outcomes [
10].
SGLT2i remain the first line of treatment in HF and CKD since they have demonstrated remarkable outcomes in heart and kidney failure independent of diabetes, indicating that they act beyond glucose [
11]. SGLT2 inhibitors block the SGLT2 transporters and decrease renal glucose absorption in the early proximal renal tubule, leading to glucosuria and reduced blood glucose levels [
12,
13]. As already mentioned, based on cardiovascular and renal outcomes research, their application has grown dramatically. The Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG OUTCOME) was the first study that revealed that SGLT2i improved cardiovascular outcomes in T2DM patients at high cardiovascular risk [
14]. According to the DAPA-CKD study, dapagliflozin lowers all-cause mortality and significant adverse renal and cardiovascular events in both diabetic and non-diabetic CKD patients. Dapagliflozin might be initiated in people with an eGFR as low as 25 mL/min, based on the favorable benefit-to-risk ratio in patients with and without T2DM [
15]. Numerous other studies, including the Empagliflozin Outcome Trial in Patients with Chronic Heart Failure and a Reduced Ejection Fraction (EMPEROR-Reduced), have confirmed and expanded these findings [
16,
17,
18,
19,
20,
21,
22]. SGLT2i are currently included in the 2019 ACC/AHA first-level preventive recommendations for CVD, and the combination of metformin and dapagliflozin is suggested as the optimal therapy regimen for glucose-lowering medication treatment of T2DM [
23].
The cardiovascular benefits of SGLT2i are thought to be caused by a number of processes, such as osmotic diuresis and natriuresis, which lower blood pressure, reduce arterial stiffness and vascular resistance, promote weight loss and reduce uric acid and oxidative stress. Elevated hemoglobin and hematocrit levels may also be involved, and glucagon’s control over heart glucose uptake is important for the beneficial inotropic and anti-arrhythmogenic effects [
14,
24,
25]. Another theory states that SGLT2i increase the effectiveness of myocardial activity by switching the metabolism of fuel from inefficient free fatty acids to more effective ketones [
26].
The renal protection mechanisms of SGLT2i are also multifactorial. SGLT2i reduce sodium reabsorption in the proximal tubule, increasing sodium delivery to the macula densa. This restoration of tubular glomerular feedback results in reduced kidney blood flow, decreased glomerular hyperfiltration and lowered intra-glomerular pressure [
27]. These effects lead to an acute reduction in albuminuria and eGFR, followed by long-term eGFR stability [
28]. SGLT2i also positively impact risk factors for renal impairment that have been already mentioned, including high blood glucose, hypertension, serum uric acid and body weight, suggesting potential nephroprotective effects in diabetes patients [
29].
According to the definition, a biomarker is “a characteristic that is objectively measured and evaluated as an indicator of normal biological processes, pathogenic processes, or pharmacologic responses to a therapeutic intervention”. Biomarkers are used to detect subclinical disease before it manifests clinically. A biomarker should be easy to test in a non-invasive manner using a well-defined approach, and the measurement obtained should be capable of identifying those who are at risk [
30]. Biomarkers can be either a clinical parameter, a circulating molecule (plasma, serum, or urine) or an imaging characteristic [
31].
2. Renal Biomarkers and SGLT2i Treatment
2.1. Renal Clinical Biomarkers and SGLT2i Treatment
The renoprotective effect of SGLT2i is largely mediated by osmotic diuresis and natriuresis-induced blood pressure (BP) reduction, local renin-angiotensin-aldosterone system inhibition and a reduction in body mass index (BMI) and arterial stiffness [
101,
102]. Clinically significant decreases in both systolic and diastolic BP have been observed in several randomized controlled studies utilizing SGLT2i in T2DM patients without any compensatory increase in heart rate [
103,
104,
105]. The EMPA-REG outcome study showed that the hemodynamic effects of empagliflozin reduce BP by a reduction in intraglomerular pressure [
106].
The regulation of body weight also plays a role in the renoprotective effect of SGLT2i. Both the EMPA-REG OUTCOME trial and the EMPEROR-Reduced trial demonstrated a statistically significant weight loss when SGLT-2 inhibitors were used. In subgroups identified by glucose-lowering medication at baseline and follow-up, a 5 kg decrease in body weight was observed [
105]. Patients in the ALTITUDE study slightly decreased their body weight as well [
107]. Treatment with dapagliflozin caused significant weight loss, an increase in ketone bodies, an increase in adiponectin, a tendency for high-sensitivity CRP to decline, an increase in glucagon and no change in immunoreactive insulin (IRI), pointing to the possibility that SGLT2i may enhance adipocyte function in obese T2DM patients [
108].
2.2. Renal Circulating Biomarkers and SGLT2i Treatment
Several regulators of inflammatory response, including nuclear factor-B (NF-B), interleukin 6 (IL-6), monocyte chemoattractant protein 1 (MCP-1), tumor necrosis factor-a (TNF-a), enzymes such as matrix metalloproteinase 7 (MMP-7) and other molecular structures such as fibronectin-1 have been shown to decrease in response to SGLT2i therapy. Among these, TNF-a is considered essential for CKD patients’ ability to manage inflammation. TNF-a may bind to any of the several TNF-Receptor (TNFR) isoforms, including isoforms 1 and 2. Elevated TNFR-1 or TNFR-2, are signs of renal failure. Treatment with canagliflozin was found to reduce TNFR-1 and TNFR-2 levels [
107]. As the sole biomarker unrelated to other risk factors for renal function decrease and whose change has been strongly linked to a decline in eGFR, the effect on TNFR-1 appears to be significant [
109].
Biomarkers of tubular injury are proteins released in the circulation by the tubular epithelial cells as a response to injury. Among them, kidney injury molecule-1 (KIM-1) is located on the apical membrane of the proximal tubule. It is released into the tubular lumen and absorbed by the peritubular capillaries and is considered a predictor of kidney failure [
110]. Compared to placebo, dapagliflozin decreased urinary KIM-1 excretion by 22.6% [
111]. Regardless of baseline renal function, ertugliflozin also demonstrated a sustained reduction in KIM-1 in patients with T2DM and stage 3 CKD [
112]. Neutrophil gelatinase-associated lipocalin (NGAL) is another biomarker of both proximal and distal tubule injury. Dapagliflozin treatment did not result in NGAL changes [
111], however, elevated NGAL levels in patients hospitalized with an acute illness and acute kidney injury treated with SGLT2i indicated that SGLT2i may enhance medullary damage [
113]. Lastly, liver-type fatty acid-binding protein (L-FABP), a marker of proximal tubular function, did not change in response to dapagliflozin treatment [
111].
In T2DM patients [
113], SGLT2i were found to be more effective than placebo at reducing the IgG-to-IgG4 fractional clearance ratio, a measurement of glomerular charge selectivity. However, dapagliflozin therapy had little to no effect on the IgG-to-albumin clearance ratio, a glomerular size selectivity indicator [
111].
Glomerular filtration rate (GFR) remains an ideal marker of kidney function. Due to the time-consuming nature of measuring GFR, it is typically estimated using equations that account for endogenous filtration markers such as serum creatinine (SCr) and cystatin C (CysC) [
114].
In a cross-sectional study, patients with T2DM who were treated with SGLT2i for at least 24 weeks were compared to those who had not in terms of their estimated glomerular filtration rate (eGFR), which was calculated using both CysC and the estimated glomerular filtration rate (eGFRcys) based on the former. The group receiving SGLT2i had significantly increased eGFRcr while eGFRcys remained the same. The SGLT2i group had a considerably greater difference between eGFRcr and eGFRcys (eGFRcr-cys) [
115,
116]. Independent of whether or not they had T2DM, the DAPA CKD trial revealed that individuals with CKD who received dapagliflozin had a significantly lower risk of a sustained decline in estimated GFR of at least 50%, end-stage kidney disease or death from renal or cardiovascular causes [
117]. The evaluation of ertugliflozin efficacy and safety cardiovascular outcomes (VERTIS CV) trial in T2DM patients with atherosclerotic CVD showed that ertugliflozin was associated with the preservation of eGFR and reduced urine albumin–creatinine ratio (UACR) [
21].
At the start of the dapagliflozin treatment, fractional urea excretion was dramatically decreased, and free water clearance was also significantly decreased after four and 14 days [
118]. Dapagliflozin also elevated plasma levels of renin, angiotensin II, urine aldosterone, angiotensinogen and copeptin in an immediate and sustained manner [
118].
A minor but substantial decrease in HbA1c has been associated with SGLT2i therapy in CKD patients, but not with a decrease in urine fractional glucose excretion [
112,
119].
2.3. Renal Urinary Biomarkers in Treatment with SGLT2i
The urine albumin/creatinine ratio was dramatically decreased after SGLT2i treatment. Urine 8-hydroxy-2C-deoxyguanosine (8-OHdG), a marker of oxidative stress linked to kidney injury, decreased but urinary N-acetyl-b-d-glucosaminidase (NAG), urinary b2-microglobulin and urinary KIM-1 remained unaltered [
119,
120]. According to Dekkers et al., decreased intra-glomerular pressure or lessened tubular cell damage may be the causes of the albuminuria-lowering effects of SGLT2i treatment [
111]. The albumin-to-creatinine ratio changed noticeably more in patients whose mean arterial pressure was under 92 mmHg [
121,
122].
Proteomics and metabolomics investigations have recently revealed new information about the discovery of novel biomarkers for the progression of diabetic nephropathy. Proteomics comprises methods for studying the urine proteome, whereas metabolomics identifies and quantifies urinary metabolites. The proteomic classifier CDK273 urine test was employed in the PRIORITY trial, and it was found that patients with T2DM had a 2.5-fold higher incidence of microalbuminuria [
123].
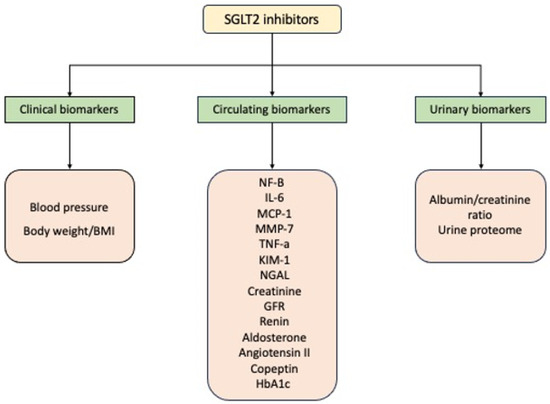
A summary of biomarkers related to renal function affected by SGLT2i treatment is presented in Figure 1.
Figure 1. Renal biomarkers affected by SGLT2i treatment. Abbreviations: NF-B: nuclear factor-B; IL-6: interleukin 6; MCP-1: monocyte chemoattractant protein 1; MMP-7: matrix metalloproteinase-7; TNF-a: tumor necrosis factor-a; KIM-1: kidney injury molecule-1; NGAL: neutrophil gelatinase-associated lipocalin; GFR: glomerular filtration rate.
This entry is adapted from the peer-reviewed paper 10.3390/pharmaceutics15112526