Mirizzi syndrome is a complication of gallstone disease caused by an impacted gallstone in the infundibulum of the gallbladder or within the cystic duct, causing chronic inflammation and extrinsic compression of the common hepatic duct or common bile duct. Eventually, mucosal ulceration occurs and progresses to cholecystobiliary fistulation. Numerous systems exist to classify Mirizzi syndrome, with the Csendes classification widely adopted. It describes five types of Mirizzi syndrome according to the presence of a cholecystobiliary fistula and its corresponding severity, and whether a cholecystoenteric fistula is present.
- Mirizzi syndrome
- cholelithiasis
- choledocholithiasis
- cholecystectomy
1. Introduction
2. Ultrasonography
3. Computed Tomography (CT)
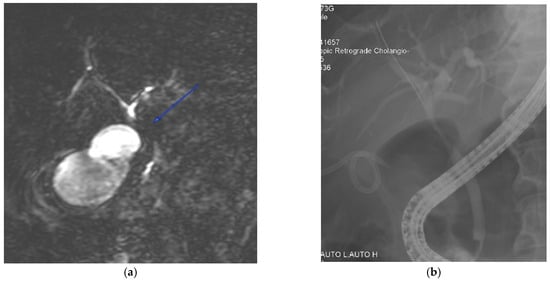
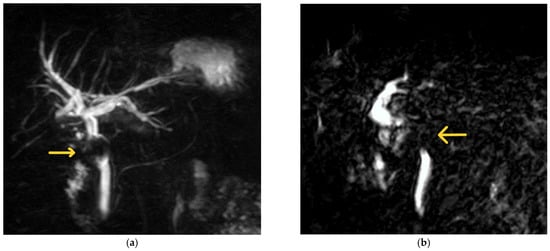
4. Magnetic Resonance Cholangiopancreatography (MRCP)
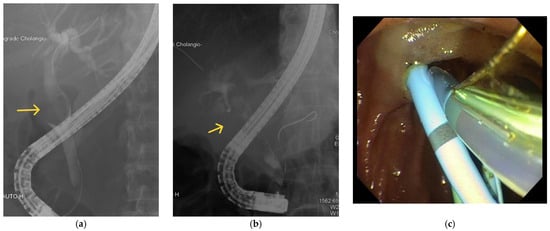
5. Endoscopic Retrograde Cholangiopancreatography (ERCP)
6. Percutaneous Transhepatic Cholangiography (PTC)
This entry is adapted from the peer-reviewed paper 10.3390/medicina60010012
References
- Valderrama-Treviño, A.I.; Granados-Romero, J.J.; Espejel-Deloiza, M.; Chernitzky-Camaño, J.; Barrera Mera, B.; Estrada-Mata, A.G.; Ceballos-Villalva, J.C.; Acuña Campos, J.; Argüero-Sánchez, R. Updates in Mirizzi Syndrome. HepatoBiliary Surg. Nutr. 2017, 6, 170–178.
- Lai, E.C.H.; Lau, W.Y. Mirizzi syndrome: History, present and future development. ANZ J. Surg. 2006, 76, 251–257.
- Shirah, B.H.; Shirah, H.A.; Albeladi, K.B. Mirizzi Syndrome: Necessity for Safe Approach in Dealing with Diagnostic and Treatment Challenges. Ann. Hepato-Biliary-Pancreat. Surg. 2017, 21, 122.
- Koike, D.; Suka, Y.; Nagai, M.; Nomura, Y.; Tanaka, N. Laparoscopic Management of Mirizzi Syndrome Without Dissection of Calot’s Triangle. J. Laparoendosc. Adv. Surg. Tech. 2017, 27, 141–145.
- Safioleas, M.; Stamatakos, M.; Safioleas, P.; Smyrnis, A.; Revenas, C.; Safioleas, C. Mirizzi Syndrome: An Unexpected Problem of Cholelithiasis. Our Experience with 27 Cases. Int. Semin. Surg. Oncol. 2008, 5, 12.
- Yip, A.W.; Chow, W.C.; Chan, J.; Lam, K.H. Mirizzi Syndrome with Cholecystocholedochal Fistula: Preoperative Diagnosis and Management. Surgery 1992, 111, 335–338.
- Yonetci, N.; Kutluana, U.; Yilmaz, M.; Sungurtekin, U.; Tekin, K. The Incidence of Mirizzi Syndrome in Patients Undergoing Endoscopic Retrograde Cholangiopancreatography. Hepatobiliary Pancreat. Dis. Int. HBPD INT 2008, 7, 520–524.
- Cui, Y.; Liu, Y.; Li, Z.; Zhao, E.; Zhang, H.; Cui, N. Appraisal of Diagnosis and Surgical Approach for Mirizzi Syndrome: Diagnosis and Treatment for Mirizzi Syndrome. ANZ J. Surg. 2012, 82, 708–713.
- Yun, E.J.; Choi, C.S.; Yoon, D.Y.; Seo, Y.L.; Chang, S.K.; Kim, J.S.; Woo, J.Y. Combination of Magnetic Resonance Cholangiopancreatography and Computed Tomography for Preoperative Diagnosis of the Mirizzi Syndrome. J. Comput. Assist. Tomogr. 2009, 33, 636–640.
- Chen, H.; Siwo, E.A.; Khu, M.; Tian, Y. Current Trends in the Management of Mirizzi Syndrome: A Review of Literature. Medicine 2018, 97, e9691.
- Piccinni, G.; Sciusco, A.; De Luca, G.M.; Gurrado, A.; Pasculli, A.; Testini, M. Minimally Invasive Treatment of Mirizzi’s Syndrome: Is There a Safe Way? Report of a Case Series. Ann. Hepatol. 2014, 13, 558–564.
- Toscano, R.L.; Taylor, P.H.; Peters, J.; Edgin, R. Mirizzi Syndrome. Am. Surg. 1994, 60, 889–891.
- Abou-Saif, A.; Al-Kawas, F.H. Complications of Gallstone Disease: Mirizzi Syndrome, Cholecystocholedochal Fistula, and Gallstone Ileus. Am. J. Gastroenterol. 2002, 97, 249–254.
- Gomez, D.; Rahman, S.H.; Toogood, G.J.; Prasad, K.R.; Lodge, J.P.A.; Guillou, P.J.; Menon, K.V. Mirizzi’s Syndrome—Results from a Large Western Experience. HPB 2006, 8, 474–479.
- Beltrán, M.A. Mirizzi Syndrome: History, Current Knowledge and Proposal of a Simplified Classification. World J. Gastroenterol. 2012, 18, 4639.
- Kulkarni, S.S.; Hotta, M.; Sher, L.; Selby, R.R.; Parekh, D.; Buxbaum, J.; Stapfer, M. Complicated Gallstone Disease: Diagnosis and Management of Mirizzi Syndrome. Surg. Endosc. 2017, 31, 2215–2222.
- Yeh, C.-N.; Jan, Y.-Y.; Chen, M.-F. Laparoscopic Treatment for Mirizzi Syndrome. Surg. Endosc. 2003, 17, 1573–1578.
- Kumar, A.; Senthil, G.; Prakash, A.; Behari, A.; Singh, R.K.; Kapoor, V.K.; Saxena, R. Mirizzi’s Syndrome: Lessons Learnt from 169 Patients at a Single Center. Korean J. Hepato-Biliary-Pancreat. Surg. 2016, 20, 17.
- Alemi, F.; Seiser, N.; Ayloo, S. Gallstone Disease. Surg. Clin. N. Am. 2019, 99, 231–244.
- England, R.E.; Martin, D.F. Endoscopic Management of Mirizzi’s Syndrome. Gut 1997, 40, 272–276.
- Kim, P.N.; Outwater, E.K.; Mitchell, D.G. Mirizzi Syndrome: Evaluation by Mr Imaging. Am. J. Gastroenterol. 1999, 94, 2546–2550.
- Chan, C.Y.; Liau, K.H.; Ho, C.K.; Chew, S.P. Mirizzi Syndrome: A Diagnostic and Operative Challenge. Surgeon 2003, 1, 273–278.
- Xu, X.; Hong, T.; Li, B.; Liu, W.; He, X.; Zheng, C. Mirizzi Syndrome: Our Experience with 27 Cases in PUMC Hospital. Chin. Med. Sci. J. 2013, 28, 172–177.
- Tan, K.; Chng, H.; Chen, C.Y.; Tan, S.; Poh, B.; Hoe, M.N. Mirizzi Syndrome: Noteworthy Aspects of a Retrospective Study in One Centre. ANZ J. Surg. 2004, 74, 833–837.
- Antoniou, S.A.; Antoniou, G.A.; Makridis, C. Laparoscopic Treatment of Mirizzi Syndrome: A Systematic Review. Surg. Endosc. 2010, 24, 33–39.
- Rayapudi, K.; Gholami, P.; Olyaee, M. Mirizzi Syndrome with Endoscopic Ultrasound Image. Case Rep. Gastroenterol. 2013, 7, 202–207.
- Moon, J.H.; Cho, Y.D.; Cheon, Y.K.; Ryu, C.B.; Kim, Y.S.; Kim, J.O.; Cho, J.Y.; Kim, Y.S.; Lee, J.S.; Lee, M.S.; et al. Wire-Guided Intraductal US in the Assessment of Bile Duct Strictures with Mirizzi Syndrome-like Features at ERCP. Gastrointest. Endosc. 2002, 56, 873–879.
- Wehrmann, T.; Riphaus, A.; Martchenko, K.; Kokabpick, S.; Pauka, H.; Stergiou, N.; Frenz, M. Intraductal Ultrasonography in the Diagnosis of Mirizzi Syndrome. Endoscopy 2006, 38, 717–722.
- Anderson, M.A.; Fisher, L.; Jain, R.; Evans, J.A.; Appalaneni, V.; Ben-Menachem, T.; Cash, B.D.; Decker, G.A.; Early, D.S.; Fanelli, R.D.; et al. Complications of ERCP. Gastrointest. Endosc. 2012, 75, 467–473.
- Rohatgi, A.; Singh, K.K. Mirizzi Syndrome: Laparoscopic Management by Subtotal Cholecystectomy. Surg. Endosc. 2006, 20, 1477–1481.