Candida albicans is a commensal fungal species that commonly colonizes the human body, but it is also a pervasive opportunistic pathogen in patients with malignant diseases. A growing body of evidence suggests that this fungus is not only coincidental in oncology patients, but may also play an active role in the development of cancer. More specifically, several studies have investigated the potential association between C. albicans and various types of cancer, including oral, esophageal, and colorectal cancer, with a possible role of this species in skin cancer as well. The proposed mechanisms include the production of carcinogenic metabolites, modulation of the immune response, changes in cell morphology, microbiome alterations, biofilm production, the activation of oncogenic signaling pathways, and the induction of chronic inflammation. These mechanisms may act together or independently to promote cancer development.
- cancer
- oral cavity
- Candida albicans
1. Introduction
|
No. of Mechanism |
Mechanism |
Reference |
|---|---|---|
|
1. |
adhesion to different surfaces |
[8] |
|
2. |
morphological changes |
[9] |
|
3. |
adaptation to different environmental conditions |
[1] |
|
4. |
production of hydrolytic enzymes |
[10] |
|
5. |
biofilm formation |
[11] |
|
6. |
avoidance of host defenses |
[12] |
2. Exploring the Links between Candida albicans and Cancer
|
Cancer Type |
Findings |
Methods |
Refs. |
|---|---|---|---|
|
Oral cancer |
C. albicans enhances the proliferation, migratory processes, as well as invasion of oral squamous cell carcinoma cells in laboratory conditions and also promotes tumor growth and metastases in test animals. |
Modulation of tumor cell behavior and the host immune response by upregulating oncogenes and potentiating a premalignant phenotype. |
[16] |
|
C. albicans infection enhances the expression of interleukin-17A(IL-17A) and its receptor (IL-17RA) in oral cancer cells and macrophages. |
The increased IL-17A/IL-17RA signaling activates macrophages and promotes the release of inflammatory cytokines, which in turn enhances the proliferation, migration, and invasion of oral cancer cells. |
[17] |
|
|
Immune cell infiltration was observed in carcinogenesis prompted by C. albicans infection. |
Single-cell expression profiling |
[18] |
|
|
Upregulation in programmed death-ligand 1 (PD-L1) expression in oral cancer cells. |
Inhibition of T cell activation and proliferation by upregulation of programmed death-ligand 1 (PD-L1) expression in vivo and in vitro. |
[19] |
|
|
C. albicans biofilm may contribute to the development and progression of oral cancer. |
Induction of lipid droplet formation and decreasing the efficacy of chemotherapy drugs |
[20] |
|
|
Genetic mutations and chromosomal abnormalities can be associated with the development of cancer. |
DNA damage and inhibition of DNA repair mechanisms cause by acetaldehyde. |
[21] |
|
|
Genetic mutations and chromosomal abnormalities can be associated with the development of cancer. |
Reactive oxygen species promote chronic inflammation and cause mitochondrial damage. |
[22] |
|
|
Esophageal cancer |
Development of epidermoid esophageal cancer. |
Treatment-resistant esophageal candidiasis. |
[23] |
|
Chronic mucocutaneous candidiasis leads to squamous cell carcinoma. |
Mutation in STAT1 protein |
||
|
Gastric cancer |
An imbalance in fungal communities with changes in fungal composition and a large increase in the abundance of C. albicans leads to gastric cancer. |
The increase in C. albicans is involved in the decrease in the abundance and diversity of other gastric fungi. |
[26] |
|
Deletion of the Dectin-3 gene led to a substantial increase in colorectal cancer development, with fungal burden in the feces of knockout mice. |
The deletion of the Dectin-3 gene led to a significantly increased abundance/proportion of C. albicans in knockout mice. |
[27] |
|
|
Differences in the composition of the feces and abundance of C. albicans could promote the process of colorectal carcinogenesis. |
Transplantation of feces from knockout, cancer-bearing mice into other mice confirmed that the feces and C. albicans could promote the process of colorectal carcinogenesis. |
[27] |
|
|
Skin cancer |
Compared with the control group, patients with Candida infection had a significantly higher risk for overall skin cancer. |
A case-control study enrolled 34,829 patients with Candida infection and an equal number of controls. |
[28] |
|
Progression of verrucous candidiasis of lip to SCC after 12 months of follow-up. |
A case report |
[29] |
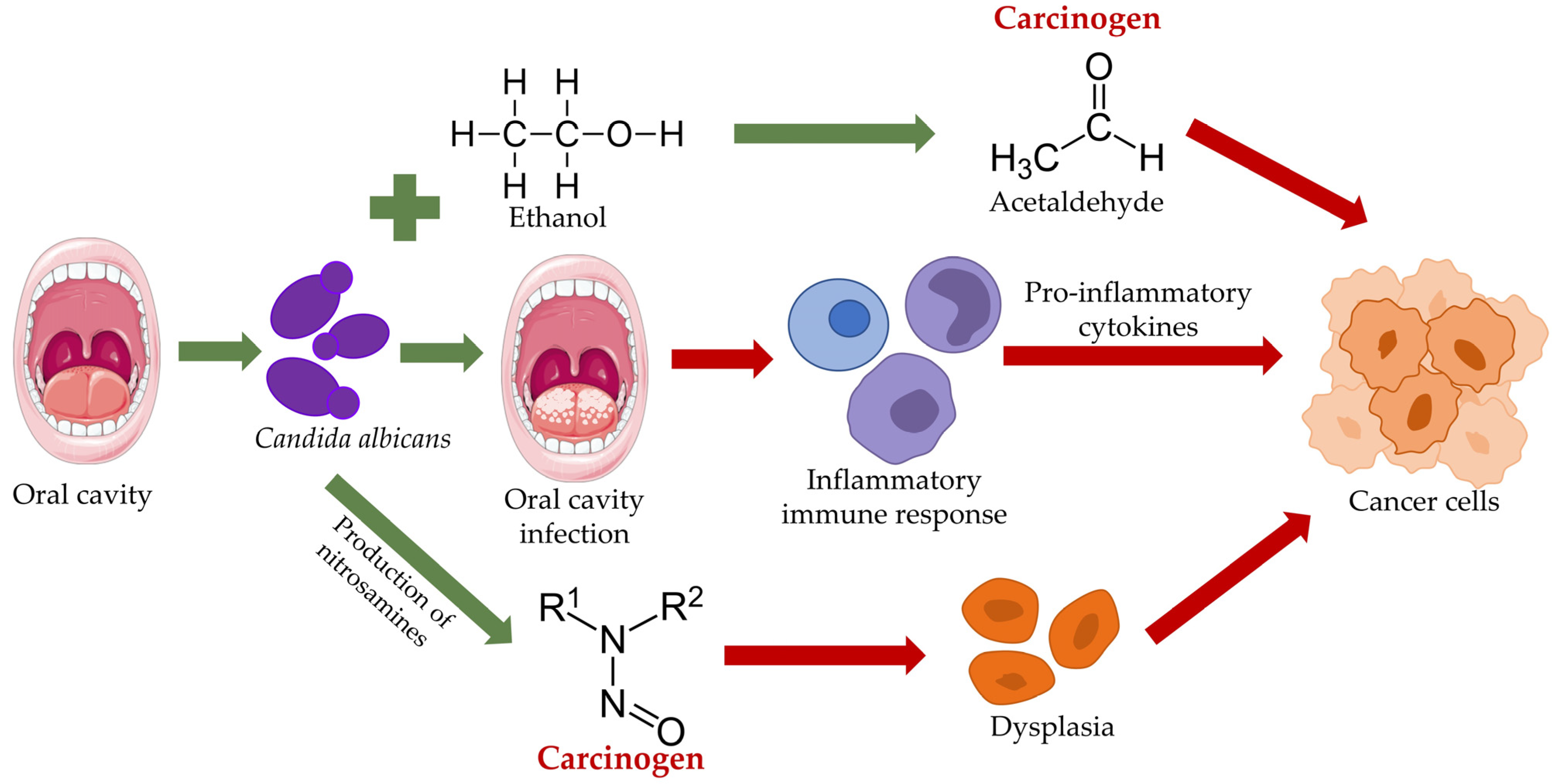
3. The Role of Candida in Oral Malignancy
This entry is adapted from the peer-reviewed paper 10.3390/microorganisms11061476
References
- Talapko, J.; Juzbašić, M.; Matijević, T.; Pustijanac, E.; Bekić, S.; Kotris, I.; Škrlec, I. Candida albicans-The Virulence Factors and Clinical Manifestations of Infection. J. Fungi 2021, 7, 79.
- Czechowicz, P.; Nowicka, J.; Gościniak, G. Virulence Factors of Candida spp. and Host Immune Response Important in the Pathogenesis of Vulvovaginal Candidiasis. Int. J. Mol. Sci. 2022, 23, 5895.
- Rahi, M.S.; Jindal, V.; Pednekar, P.; Parekh, J.; Gunasekaran, K.; Sharma, S.; Stender, M.; Jaiyesimi, I.A. Fungal infections in hematopoietic stem-cell transplant patients: A review of epidemiology, diagnosis, and management. Ther. Adv. Infect. Dis. 2021, 8, 20499361211039050.
- Dudakova, A.; Blei, C.; Groß, U.; Schulze, M.H. Impact of routine bedside infectious diseases service on clinical management and prognosis of patients with Candida fungemia—An example for Antifungal Stewardship at university level in Germany. Int. J. Infect. Dis. 2022, 119, 150–159.
- Kojic, E.M.; Darouiche, R.O. Candida infections of medical devices. Clin. Microbiol. Rev. 2004, 17, 255–267.
- Macias-Paz, I.U.; Pérez-Hernández, S.; Tavera-Tapia, A.; Luna-Arias, J.P.; Guerra-Cárdenas, J.E.; Reyna-Beltrán, E. Candida albicans the main opportunistic pathogenic fungus in humans. Rev. Argent. Microbiol. 2022, 7541, 00084-0.
- Lopes, J.P.; Lionakis, M.S. Pathogenesis and virulence of Candida albicans. Virulence 2022, 13, 89–121.
- Martin, H.; Kavanagh, K.; Velasco-Torrijos, T. Targeting adhesion in fungal pathogen Candida albicans. Future Med. Chem. 2021, 13, 313–334.
- Kadosh, D. Control of Candida albicans morphology and pathogenicity by post-transcriptional mechanisms. Cell. Mol. Life Sci. 2016, 73, 4265–4278.
- Galocha, M.; Pais, P.; Cavalheiro, M.; Pereira, D.; Viana, R.; Teixeira, M.C. Divergent Approaches to Virulence in C. albicans and C. glabrata: Two Sides of the Same Coin. Int. J. Mol. Sci. 2019, 20, 2345.
- Atriwal, T.; Azeem, K.; Husain, F.M.; Hussain, A.; Khan, M.N.; Alajmi, M.F.; Abid, M. Mechanistic Understanding of Candida albicans Biofilm Formation and Approaches for Its Inhibition. Front. Microbiol. 2021, 12, 638609.
- Singh, D.K.; Tóth, R.; Gácser, A. Mechanisms of Pathogenic Candida Species to Evade the Host Complement Attack. Front. Cell. Infect. Microbiol. 2020, 10, 94.
- Teoh, F.; Pavelka, N. How Chemotherapy Increases the Risk of Systemic Candidiasis in Cancer Patients: Current Paradigm and Future Directions. Pathogens 2016, 5, 6.
- Ramirez-Garcia, A.; Rementeria, A.; Aguirre-Urizar, J.M.; Moragues, M.D.; Antoran, A.; Pellon, A.; Abad-Diaz-De-Cerio, A.; Hernando, F.L. Candida albicans and cancer: Can this yeast induce cancer development or progression? Crit. Rev. Microbiol. 2016, 42, 181–193.
- Yu, D.; Liu, Z. The research progress in the interaction between Candida albicans and cancers. Front. Microbiol. 2022, 13, 988734.
- Vadovics, M.; Ho, J.; Igaz, N.; Alföldi, R.; Rakk, D.; Veres, E.; Szücs, B.; Horváth, M.; Tóth, R.; Szücs, A.; et al. Candida albicans Enhances the Progression of Oral Squamous Cell Carcinoma in vitro and in vivo. mBio 2021, 13, e0314421.
- Wang, X.; Wu, S.; Wu, W.; Zhang, W.; Li, L.; Liu, Q.; Yan, Z. Candida albicans Promotes Oral Cancer via IL-17A/IL-17RA-Macrophage Axis. mBio 2023, e0044723.
- Hsieh, Y.P.; Wu, Y.H.; Cheng, S.M.; Lin, F.K.; Hwang, D.Y.; Jiang, S.S.; Chen, K.C.; Chen, M.Y.; Chiang, W.F.; Liu, K.J.; et al. Single-Cell RNA Sequencing Analysis for Oncogenic Mechanisms Underlying Oral Squamous Cell Carcinoma Carcinogenesis with Candida albicans Infection. Int. J. Mol. Sci. 2022, 23, 4833.
- Wang, X.; Zhao, W.; Zhang, W.; Wu, S.; Yan, Z. Candida albicans induces upregulation of programmed death ligand 1 in oral squamous cell carcinoma. J. Oral Pathol. Med. 2022, 51, 444–453.
- Marin-Dett, F.H.; Campanella, J.E.M.; Trovatti, E.; Bertolini, M.C.; Vergani, C.E.; Barbugli, P.A. Extracellular lipids of Candida albicans biofilm induce lipid droplet formation and decreased response to a topoisomerase I inhibitor in dysplastic and neoplastic oral cells. J. Appl. Oral Sci. 2023, 30, e20220319.
- Mizumoto, A.; Ohashi, S.; Hirohashi, K.; Amanuma, Y.; Matsuda, T.; Muto, M. Molecular Mechanisms of Acetaldehyde-Mediated Carcinogenesis in Squamous Epithelium. Int. J. Mol. Sci. 2017, 18, 1943.
- Sultan, A.S.; Theofilou, V.I.; Alfaifi, A.; Montelongo-Jauregui, D.; Jabra-Rizk, M.A. Is Candida albicans an opportunistic oncogenic pathogen? PLoS Pathog. 2022, 18, e1010413.
- Develoux, M. Cancer and mycoses and literature review. Bull. Soc. Pathol. Exot. 2017, 110, 80–84.
- Walker, A.W.; Duncan, S.H.; Louis, P.; Flint, H.J. Phylogeny, culturing, and metagenomics of the human gut microbiota. Trends Microbiol. 2014, 22, 267–274.
- Domingues-Ferreira, M.; Grumach, A.S.; Duarte, A.J.D.S.; De Moraes-Vasconcelos, D. Esophageal cancer associated with chronic mucocutaneous candidiasis. Could chronic candidiasis lead to esophageal cancer? Med. Mycol. 2009, 47, 201–205.
- Zhang, Z.; Feng, H.; Qiu, Y.; Xu, Z.; Xie, Q.; Ding, W.; Liu, H.; Li, G. Dysbiosis of Gastric Mucosal Fungal Microbiota in the Gastric Cancer Microenvironment. J. Immunol. Res. 2022, 2022, 6011632.
- Zhu, Y.; Shi, T.; Lu, X.; Xu, Z.; Qu, J.; Zhang, Z.; Shi, G.; Shen, S.; Hou, Y.; Chen, Y.; et al. Fungal-induced glycolysis in macrophages promotes colon cancer by enhancing innate lymphoid cell secretion of IL-22. EMBO J. 2021, 40, e105320.
- Chung, L.M.; Liang, J.A.; Lin, C.L.; Sun, L.M.; Kao, C.H. Cancer risk in patients with candidiasis: A nationwide population-based cohort study. Oncotarget 2017, 8, 63562–63573.
- Wang, J.X.; Yu, S.H.; Hall, R.R.; McNiff, J.; Leffell, D.J.; Kibbi, N. Verrucous candidiasis of the lip: A harbinger of squamous cell carcinoma. JAAD Case Rep. 2021, 16, 168–170.
- Abati, S.; Bramati, C.; Bondi, S.; Lissoni, A.; Trimarchi, M. Oral Cancer and Precancer: A Narrative Review on the Relevance of Early Diagnosis. Int. J. Environ. Res. Public Health 2020, 17, 9160.
- Markopoulos, A.K. Current aspects on oral squamous cell carcinoma. Open Dent. J. 2012, 6, 126–130.
- Sujir, N.; Ahmed, J.; Pai, K.; Denny, C.; Shenoy, N. Challenges in Early Diagnosis of Oral Cancer: Cases Series. Acta Stomatol. Croat. 2019, 53, 174–180.
- Inchingolo, F.; Santacroce, L.; Ballini, A.; Topi, S.; Dipalma, G.; Haxhirexha, K.; Bottalico, L.; Charitos, I.A. Oral Cancer: A Historical Review. Int. J. Environ. Res. Public Health 2020, 17, 3168.
- Di Cosola, M.; Cazzolla, A.P.; Charitos, I.A.; Ballini, A.; Inchingolo, F.; Santa Croce, L. Candida albicans and Oral Carcinogenesis. A Brief Review. J. Fungi 2021, 7, 476.
- Ayuningtyas, N.F.; Mahdani, F.Y.; Pasaribu, T.A.S.; Chalim, M.; Ayna, V.K.P.; Santosh, A.B.R.; Santacroce, L.; Surboyo, M.D.C. Role of Candida albicans in Oral Carcinogenesis. Pathophysiology 2022, 29, 650–662.
- Krogh, P.; Hald, B.; Holmstrup, P. Possible mycological etiology of oral mucosal cancer: Catalytic potential of infecting Candida albicans and other yeasts in production of N-nitrosobenzylmethylamine. Carcinogenesis 1987, 8, 1543–1548.
- Bakri, M.M.; Hussaini, H.M.; Holmes, A.; Cannon, R.D.; Rich, A.M. Revisiting the association between candidal infection and carcinoma, particularly oral squamous cell carcinoma. J. Oral Microbiol. 2010, 2, 2.
- Manzo-Avalos, S.; Saavedra-Molina, A. Cellular and mitochondrial effects of alcohol consumption. Int. J. Environ. Res. Public Health 2010, 7, 4281–4304.
- Richardson, J.P.; Moyes, D.L. Adaptive immune responses to Candida albicans infection. Virulence 2015, 6, 327–337.
- Ho, J.; Camilli, G.; Griffiths, J.S.; Richardson, J.P.; Kichik, N.; Naglik, J.R. Candida albicans and candidalysin in inflammatory disorders and cancer. Immunology 2021, 162, 11–16.
- Yeoh, S.-C.; Hua, H.; Yepes, J.F.; Peterson, D.E. Oral Manifestations of Systemic Diseases and their Treatments. In Contemporary Oral Medicine; Farah, C., Balasubramaniam, R., McCullough, M., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 1–117.
- Findley, K.; Oh, J.; Yang, J.; Conlan, S.; Deming, C.; Meyer, J.A.; Schoenfeld, D.; Nomicos, E.; Park, M.; Becker, J.; et al. Topographic diversity of fungal and bacterial communities in human skin. Nature 2013, 498, 367–370.
- Mahalingam, S.S.; Jayaraman, S.; Pandiyan, P. Fungal Colonization and Infections-Interactions with Other Human Diseases. Pathogens 2022, 11, 212.
- Ascani, G.; Balercia, P.; Messi, M.; Lupi, L.; Goteri, G.; Filosa, A.; Stramazzotti, D.; Pieramici, T.; Rubini, C. Angiogenesis in oral squamous cell carcinoma. Acta Otorhinolaryngol. Ital. 2005, 25, 13.
- Engku Nasrullah Satiman, E.A.F.; Ahmad, H.; Ramzi, A.B.; Abdul Wahab, R.; Kaderi, M.A.; Wan Harun, W.H.A.; Dashper, S.; McCullough, M.; Arzmi, M.H. The role of Candida albicans candidalysin ECE1 gene in oral carcinogenesis. J. Oral Pathol. Med. 2020, 49, 835–841.
- Lewis, M.A.O.; Williams, D.W. Diagnosis and management of oral candidosis. Br. Dent. J. 2017, 223, 675–681.
- Wang, X.; Zhang, W.; Wu, W.; Wu, S.; Young, A.; Yan, Z. Is Candida albicans a contributor to cancer? A critical review based on the current evidence. Microbiol. Res. 2023, 272, 127370.
- Sanjaya, P.R.; Gokul, S.; Gururaj Patil, B.; Raju, R. Candida in oral pre-cancer and oral cancer. Med. Hypotheses 2011, 77, 1125–1128.
- Vila, T.; Sultan, A.S.; Montelongo-Jauregui, D.; Jabra-Rizk, M.A. Oral Candidiasis: A Disease of Opportunity. J. Fungi 2020, 6, 15.
- Stasiewicz, M.; Karpiński, T.M. The oral microbiota and its role in carcinogenesis. Semin. Cancer Biol. 2022, 86, 633–642.
- Huët, M.A.L.; Lee, C.Z.; Rahman, S. A review on association of fungi with the development and progression of carcinogenesis in the human body. Curr. Res. Microb. Sci. 2021, 3, 100090.
- Hellstein, J.W.; Marek, C.L. Candidiasis: Red and White Manifestations in the Oral Cavity. Head Neck Pathol. 2019, 13, 25–32.
- Tamgadge, S.; Tamgadge, A.; Pillai, A.; Chande, M.; Aacharya, S.; Kamat, N. Association of Candida sp. with the Degrees of Dysplasia and Oral Cancer: A Study by Calcofluor White under Fluorescent Microscopy—PubMed. Iran J. Pathol. 2017, 12, 348–355.
- Mohammed, F.; Fairozekhan, A. Oral Leukoplakia. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023.
- Sharma, N.; Bhatia, S.; Sodhi, A.S.; Batra, N. Oral microbiome and health. AIMS Microbiol. 2018, 4, 42–66.