1. Epidemiology of Individual Immobilisation and Immobility Syndrome
Individual risk of immobility syndrome (IS) is widely acknowledged to increase with age, owing to the very nature of the aging process itself, which tends to induce numerous bodily changes over time in all older adults. Studies indicate these changes to be further exacerbated by periods of forced immobility, which is acknowledged to cause appreciable damage to the immobilised parts of one’s body. Additionally, this promotes further disorders in other parts of the body, as if by way of a knock-on effect, thus affecting it as a whole [
25]. IS affecting older adults is not so much owing to the incidence of specific diseases, but is rather primarily a direct consequence of significantly reduced physical activity during the daytime, either owing to general weakness of the body itself, or to an individually experienced fear of falling.
Functional limitations experienced by older adults, for example serious difficulties when bending or kneeling (as frequently reported by the patients themselves), account for their preference for spending time in static postures, consequently putting themselves at risk of IS, and appreciably reduced overall quality of life [
26,
27,
28,
29]. Such individuals experience a progressive decline in their ability to carry out the routine activities of daily living, as assessed by, for example, the ADL scale [
30]. Approximately 20% of individuals over 65 years of age experience significant mobility problems, unless making use of walking aids, or being directly assisted by a third party.
Lack of recommended physical activity adversely affects the hippocampus, causing memory problems in older adults. This may manifest itself, for instance, in the anxiety of forgetting one’s way to a local grocery shop, which may then transform itself into a fear of leaving the house altogether, which would then be bound to evolve into a significant drop in one’s activity during daytime [
31]. When over the age of 75, more than half of older adults experience difficulties leaving their apartment, whereas approximately 20% opt to not venture outside at all. The scale of the problem is further highlighted by the estimate that approximately 50% of individuals affected by severe IS are likely to die within the following 6–12 months [
32].
The risk of IS varies, depending on the concomitant chronic medical conditions. Studies indicate that with regard to deep vein thrombosis, IS may be experienced by 15% of individuals who are confined to their homes, whereas in the case of disease exacerbation and resultant hospitalisation, IS may affect as many as 27% of them [
12]. IS also affects approximately 43–60% of those remaining in institutionalised care [
14].
At least two primary and two secondary criteria must effectively be satisfied prior to diagnosing IS. The primary criteria include moderate to severe cognitive deficit and spontaneous muscle cramps. Secondary criteria include skin marks attesting to the individual remaining in the same position over an extensive period, pressure ulcers, dysphagia, aphasia, and urinary incontinence [
33]. Of individuals aged 75–81 years who satisfy the IS criteria, 72% are likely to be hospitalised within the following 12 months [
34].
Published studies indicate that as far as older adults are concerned, individual lack of self-motivation is the second-most common barrier to the pursuit of any physical activity (38.4%), right after feelings of chronic fatigue (51.7%) [
35]. As a specific medical condition, IS actually precedes individual immobilisation, which is bound to be the case, given the development of medical conditions caused by a significant mobility deficit. Individual immobilisation may befall anyone, regardless of age. Individual ability to pursue routine activities of daily living tends to drop dramatically, especially in older adults [
36], owing mostly to a diversity of medical conditions and/or injuries (
Table 1) [
37,
38,
39,
40,
41,
42].
Table 1. Principal causes of immobilisation in older adults [
37,
38,
39,
40,
41,
42].
Various studies on older adults have asserted that it tends to occur mostly in hospitalized individuals, as they spend about 83% of their time in bed, whereas in some cases, for example following a hip replacement procedure, this may even be up to 99% [
43,
44].
Some studies also highlight restriction in individual motor activity of up to 97% [
45,
46]. Immobilisation is then a natural consequence that affects one in three hospitalised older adults. This also causes a significant reduction in individual physiological reserves (Frailty Syndrome), which is one of the causes of one’s immobilisation [
12,
47]. A juxtaposition of immobilisation and immobility syndrome is presented in
Table 2.
Table 2. The differences between immobilisation and IS in older adults.
2. Consequences of Immobilisation and IS
The consequences of immobilisation and IS entail the same bodily systems and structures. The difference actually lies in the development speed of pathologies and dysfunctions limiting the ADLs. Additionally, persistent IS may lead to immobility owing to the development of a diversity of medical conditions originating in the significantly restrained individual motor activity. Apart from general weakness of the body, various physiological disorders in the immobilised patient tend to affect other bodily systems, for example circulatory, respiratory, muscular, skeletal, nervous, urinary, digestive, and even the overall condition of a patient’s skin [
48,
49].
Such consequences are most likely to be encountered in 5–41% of older adults; muscle cramps being by far the most common effect of individual immobilisation (55%). Approximately 3.4% of older adults, having previously fallen victim to immobilisation, will develop pneumonia, while 1 in 100 individuals will experience inflammation of the urinary tract, deep vein thrombosis, or pressure ulcers, as far as general statistical estimates are concerned [
50,
51]. The key symptoms accompanying individual immobilisation are summarised in
Table 3 [
25,
48,
52,
53,
54,
55,
56,
57,
58,
59,
60].
Table 3. Immobilisation symptoms, stratified by their respective systems within the body [
25,
48,
52,
53,
54,
55,
56,
57,
58,
59,
60].
3. Individual Immobilisation and Increased Exposure to Fall Risk
Individual immobilisation is closely associated with hospitalisation in older adults, with the most common causes consisting of femoral neck fracture, Parkinson’s disease, arthritis, and osteoporosis. In the case of ischaemic stroke, this can be about 2–5 days, upon haemorrhagic stroke, up to several weeks, and upon intracerebral haemorrhage, this can be approximately 4 weeks [
61]. Exposure to fall risk following hospitalisation has been established to be at its highest within the first 2 weeks following hospital discharge, and tends to stabilise within 3 months or so [
62].
Approximately 14% of older adults aged 65 years and over experience a fall within the first month of hospital discharge, whereas 40% of the discharged patients experience a fall within the first 6 months [
63,
64,
65], of whom 50% will most likely sustain an injury [
66]. During IS or immobilisation, and immediately afterwards, several symptoms that interact with overall fall risk occur. Muscle strength, muscle function, and sense of balance deteriorate in such individuals [
67,
68]. In the case of immobilised individuals, their muscle strength deteriorates with each passing week. Within the first week, due to an appreciable loss of muscle mass, muscle strength may drop by 40% [
69].
4. Individual Immobilisation and Additional Fall Risk Factors
Depleted bone mass and osteoporosis contribute appreciably to an increased risk of sustaining falls, experiencing bone fractures, and requiring recurrent hospitalisations [
70]. Regular intake of medications or certain active substances affecting the nervous and circulatory systems may also prove appreciably instrumental in increasing overall fall risk by way of inducing sluggishness, disorientation, dizziness, or poor coordination of movement [
71]. Additionally, the cardiorespiratory dysfunction [
72], malnutrition, reduced body weight, and attendant postural changes are regarded legitimate risk factors for falls [
73,
74,
75].
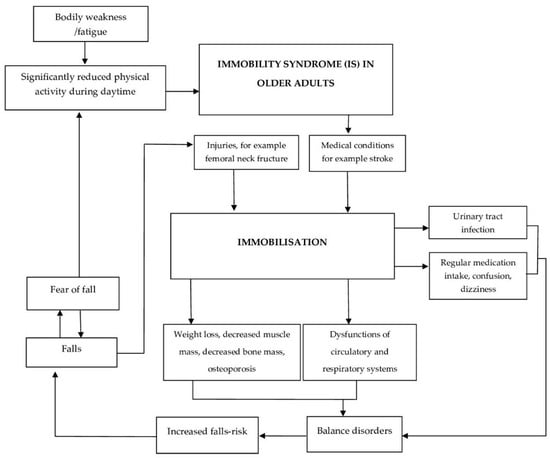
Immobilised individuals often experience a fear of falling as something instilled in them well, especially when said immobilisation is due to having sustained a fall in the first place. This also holds true for other medical conditions, for example, stroke [
76,
77,
78]. Urinary dysfunctions and various infections may also be considered potential consequences (see
Figure 1) [
79].
Figure 1. Interactions between older adults affected by IS, individual immobilisation, and falls.
5. Fall Prevention Measures for the Individuals Affected by IS, or Who Have Had Sustained Previous Episodes of Individual Immobilisation
Despite such alarming statistics, a majority of falls can be effectively prevented, and any subsequent readmission to hospital due to any post-fall injuries can also be avoided. It is crucial that health care professionals offer appropriately structured education to patients, as well as attend to implementing effective fall prevention strategies as a legitimate part of the routine hospital discharge procedure [
80,
81,
82]. As far as the individuals affected by IS are concerned, active involvement of their families is very important, as much so as the contribution made by various institutions put in charge of disseminating various pragmatically structured intervention programmes among the patients, specifically aimed at preventing decline in their functional abilities, thus appreciably minimising the overall risk of falling victim to medical conditions that might lead to likely hospitalisation and subsequent immobilisation.
The individuals suffering from a fear of falling should be encouraged to verbalise their feelings, and work on enhancing their own sense of self-reliance in moving about, be that through individual therapy, or structured group activities, or a mix of both approaches. Seniors affected by cognitive impairment should be regularly monitored for cognitive function and offered targeted behavioural therapy.
The key task consists of focusing the work on the patient’s muscular strength and balance, both static and dynamic, which, in conjunction with an appropriately structured dietary intake, would be bound to effectively prevent any detrimental reduction in bone mass.
6. Immobility Syndrome, Dietary Intake, and Optimised Use of Medications
The right amount of dietary fibre, combined with adequate hydration, fused into an individualised treatment plan, would then translate into a reduced risk of functional dysfunction, as well as addressing individual susceptibility to infections of both the urinary and excretory systems. The actual number and type of medications regularly taken by older individuals should, whenever feasible, be modified to ensure that they do not cause disorientation and dizziness [
83,
84,
85]. Even though older patients often respond quite favourably to any individually tailored education, there is no evidence that such individually targeted education alone would be sufficient to reduce overall fall risk and the actual number of fall episodes, following prior immobilisation directly associated with hospitalisation [
86].
7. Training the IS Patients in Making Use of Effective Fall Prevention Strategies
In view of the fact that IS, and the period immediately following previous immobilisation of older adults, are invariably associated with general bodily weakness (inclusive of appreciable deterioration in individual muscle strength) [
68], and a high fall risk, not only should effective measures be adopted, specifically aimed at implementing effective fall prevention strategies, but the entire approach to this task should be subject to a major rethink, with a view to making it far more comprehensive. It is absolutely vital that seniors should be trained appropriately to be able to cope well on their own (unassisted) after sustaining a fall, provided it has not resulted in any serious injuries [
87].
One of the effective ways of coping after an accidental fall is offered by the backward-chaining method [
2,
88]. This method differs quite distinctly from the conventional methods, as it relies predominantly on the implementation of a reverse sequence of movements by the victim of an accidental fall. Not only does it prove particularly effective at assisting a faller with getting up from the floor entirely on their own, i.e., without the involvement of a third party, but its application is also very user- friendly in character.
8. Unequivocal Terminology Postulated in Diagnosing the Origins of IS or Individual Immobilisation
Individual immobilisation appears now to have become an essential issue within the population of older adults worldwide. As the population of seniors swells, so does the issue at hand. Given its appreciable complexity, it is construed in terms of a diversity of disorders and medical conditions. As no sufficiently coherent and unequivocally verbalised definition has been agreed upon as yet between the academicians actually dealing with it, many terms are still being used interchangeably across the published academic studies, even though individual immobilisation may either originate in, for example individual trauma/surgical intervention, or may well be a result of the appreciable, mainly age-induced, mobility deficit encountered among a vast majority of older adults.
9. Overall Versatility and Effectiveness of VR Technology Solutions
As is well evidenced across all of the published research, the diverse VR technology solutions boast substantial versatility, which makes them, medically speaking, perfectly viable as easily adaptable therapeutic tools, and are also applicable in patients with specific needs. Their inherent versatility makes it possible to stimulate the patients effectively in many areas of their functional performance, predominantly in the case of those suffering from substantial deficits that usually hamper the pursuit of the activities of daily living, mostly due to excessive fear of falling.
In practical terms, the attending medical personnel may select specific VR solutions believed to be best suited for the task at hand by opting for one of a variety of VR platforms (e.g., Nintendo Wii, Xbox Kinect), through VR goggles (Carl Zeiss), right up to goggles fitted out with hand-held motion controllers (e.g., Oculus Rift S).
This entry is adapted from the peer-reviewed paper 10.3390/jcm12175675